
Reticulo-cutaneous fistula due to the ingestion of a long metallic rod in a cow
2014-03-23 01:29AzariOmidAliAsgharMozaffari
Azari Omid, Ali Asghar Mozaffari
Department of Clinical Sciences, Faculty of Veterinary Medicine, Shahid Bahonar University of Kerman, Kerman, Iran
Reticulo-cutaneous fistula due to the ingestion of a long metallic rod in a cow
Azari Omid*, Ali Asghar Mozaffari
Department of Clinical Sciences, Faculty of Veterinary Medicine, Shahid Bahonar University of Kerman, Kerman, Iran
PEER REVIEW
Peer reviewer
Ehsan Sakhaee, Associated Professor, Department of Clinical Sciences, Large animal internal Medicine Section, Faculty of Veterinary Medicine, Shahid Bahonar University of Kerman, Iran.
Tel: +98 341 3202926
Fax: +98 341 3222047
E-mail: Ehsan_sakhaee@mail.uk.ac.ir
Comments
This is a good and interesting study in which the authors presented incidence of a rare case report about swallow of a very big foreign body (metallic rod) by the cow and subsequently reticulocutaneous fistula happened.
Details on Page
A five-year-old cow was referred to the veterinary faculty hospital for treatment of a swelling mass with a cutaneous fistula at the left lower part of the chest wall, between 7th till 9th intercostals space. Abdominal pain in palpation of the mass was observed with no abnormality in clinical symptoms. In surgical exploration, skin incision was carried out on the swelling mass and surprisingly a sinus tract with a sharp metallic rod (26 cm length) that continued to the reticulum lumen was identified. Because of unsuccessful attempting to remove of the foreign body, flank laparotomy and rumenotomy was performed. After one month, the cow led to complete recovery.
Reticulo-cutaneous fistula, Foreign body, Reticulum, Cow
1. Introduction
Among the numerous diseases of foreign body syndrome in ruminant species, traumatic reticuloperitonitis (TRP) are the most common. TRP is a sporadic disease in ruminants caused by perforation of the reticulum due to ingestion of foreign materials, which is a common cause of abdominal surgery in cattle[1].
Cattle’s indiscriminate eating habits make them susceptible to inadvertent ingestion of foreign bodies with subsequent penetration of a forestomach compartment[2]. Moreover, the honeycomb-like structure of the reticulum provides many sites for fixation of a foreign body, and contractions of the reticulum may be sufficient to push a sharp foreign body through the wall, inducing the disease[3]. The increase in the intra-abdominal pressure due to the pregnancy and ruminal tympany may facilitate the penetration of the foreign bodies into the reticular wall[4]. The foreign bodies ingested by cattle are most often wires (76%) and nails (30%) but also include steel objects[5]. The clinical signs of cattle with TRP are variable, depending on the severity, duration and involvement of other organs. Fever, increased heart and respiratory rate, anorexia, dehydration, decreased milk production, weight loss, ruminal stasis, chronic tympani, abdominal tension and rigid abdominal pain with grunting are the commonclinical signs observed in cattle with TRP[6-8]. Two treatment procedures for TRP were recommended; conservative therapy (magnetp.o.and antibiotics) and surgery (Rumenotomy)[9,10].
Although there are many reports about the existence of metallic foreign body in the cattle forestomach, the current study presents surprisingly reticulo-cutaneous fistula following to swallow of a long metallic rod in cow.
2. Case report
A five-year-old mixed-breed cow was referred to the surgical unit of veterinary teaching hospital for treatment of a painful swelling mass on the left lower part of the chest wall, between 7th till 9th intercostals space. The owner declared that the mass has been growing up gradually through two months prior to presentation and the cow’s milk production dropped very markedly. The cow has been treated with a broad-spectrum antibiotic for two weeks before presentation. On clinical examination, all vital signs (heart rate, respiratory rate and rectal temperature) were in the normal range but the animal was lethargic and depressed with rumen hypomotility. On laboratory findings, packed cell volume, cell blood count and differential leukocyte count were within normal limits. In close examination of the mass, a skin fistula that extended to the reticulum was diagnosed.
In surgical exploration, skin incision was carried out on the swelling mass and after debridment of necrotic tissues; surprisingly a sinus tract with a sharp metallic rod that continued to the reticulum lumen was identified (Figure 1A). The metallic rod was extracted from the sinus tract, but the end of the rod was stuck in 8th intercostal space. Because of unsuccessful attempting to remove of the foreign body from the sinus tract, left flank laparotomy and rumenotomy was performed. In exploratory laparotomy, local peritonitis and adhesion of reticulum to the abdominal wall was confirmed. After incision on rumen wall, exploration in reticulum lumen was performed and the metallic object easily was found and removed. Then the rumen, abdominal muscles and skin were sutured routinely. The sharp metallic rod was 26 cm length and 14 mm diameter with a small vertical pin at its blunt end (Figure 1B).
Post-operative care included daily irrigation of sinus tract with copious amounts of sterile saline and povidone-iodine 1%, and a dose of penicillin-streptomycin (20 000 IU/kg-20 mg/kg, IM), every 12 h for seven days. After one month, the fistula was closed via second-intention wound healing process and the cow recovered uneventfully, although the amount of milk production has not returned to the normal level.
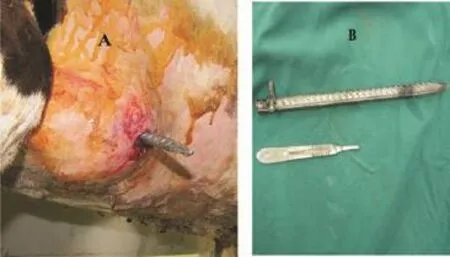
Figure 1.Penetration of the reticulum of the caw due to the metallic rod.A: The swelling mass on the left ventral part of the chest wall with skin fistula, the sharp metallic rod extracted from reticulo-cutaneous sinus tract; B: The metallic rod (26 cm length and 14 mm diameter) with a small vertical pin at its blunt end that was removed from reticulum lumen.
3. Discussion
Foreign body penetration of the reticulum in older cows is one of the most common causes of disease of the forestomach compartments requiring surgical intervention[5]. Diagnose of TRP in cow is based on clinical and hematological examinations, biochemical analysis, radiology and ultrasonographic examinations[3]. The results of blood fibrinogen and protein concentrations, enzymatic alterations and calcium variations in TRP show that blood biochemistry may be considered a useful index in early diagnosis of TRP[11,12]. In the current study, because of easy identification of the perforating foreign body during close examination of the fistula, it didn’t need to use the paraclinic examinations for diagnosis confirmation. In our study, twoweek administration of board spectrum antibiotic caused insignificant alteration in vital symptoms and hematological parameters.
Medical treatment of TRP is directed at preventing further perforation of the reticulum and treating the septic reticulitis and peritonitis[5]. Non surgical treatment of TRP includes the use of antibiotics and dosing with magnet. Under influence of antibiotic (penicillin and streptomycin) some cases improve and appear to recover, if the foreign object doesn’t remain in the wall of the reticulum but returns to the lumen. However, if the foreign body has been dislodged the antibiotic will help to control the local infection. Oral administration of a magnet fixes ferromagnetic foreign body that has not penetrated deeply or lies loose in reticulum lumen. In valuable cattle, conservative therapy is not recommended because its uncertainty[5]. In chronic cases, if the animal fails to respond to conservative therapy, or if a reticular abscess is suspected, surgery is indicated. Thearea of interest is best explored by left flank celiotomy[5,13]. In the current study, it seemed because of the vertical pin at the end of metallic red, extraction of the rod from intercostal space was impassible, and therefore rumenotomy operation and remove of the rod from the reticulum lumen was inevitable.
The rumenotomy procedure can be a safe and effective way to retrieve ingested foreign bodies and address other problems of the ruminant forestomachs. Rumen surgery has been associated with few postoperative complications. Morbidity and mortality in cases that have had a previous rumenotomy have mostly been associated with complications related to the original presurgical condition or from causes unrelated to the rumen surgery[13].
In the current report, because of long-term involvement, and existence of fibrotic and necrotic tissues around the perforation site of the reticulum, suturing of the fistula wound was impossible; consequently the skin wound was irrigated with saline solution and povidone-iodine 1% every day until healed via second intention wound healing process. Till now, it has still remained unclear for the authors how the calf swallowed such a long object.
Conflict of interest statement
We declare that we have no conflict of interest.
Comments
Background
The incidence of ingestion of foreign body is high in ruminants, but in the current case report swallow of the incredible foreign body (metallic rod) and induce of reticulucutaneous fistula is very interesting and rarely reported.
Research frontiers
The manuscript has reported a rare case of ingestion of wonderful foreign body in cow.
Related reports
The authors have cited some references related to surgery of the ruminant forestomach. However, according to my search, there is no report about the current case report topic.
Innovations and breakthroughs
This manuscript has just reported the rare case report. And according to my search, there is no report about the current case report topic.
Applications
The manuscript shows the penetrating foreign bodies can pass from the reticular lumen to the intra-costal space and make reticulo-cutaneous fistula in ruminant.
Peer review
This is a good and interesting study in which the authors presented incidence of a rare case report about swallow of a very big foreign body (metallic rod) by the cow and subsequently reticulo-cutaneous fistula happened.
[1] Braun U. Ultrasonography in gastrointestinal disease in cattle. Vet J 2003; 166: 112-124.
[2] Ducharme NG, Fubini SL. Surgery of the ruminant forestomach compartments. In: Fubini SL, Ducharmi NG, editors. Farm animal surgery. USA: Elsevier Science; 2004, p. 184-194.
[3] Ghanem MM. A comparitive study on traumatic reticuloperitonitis and traumatic pericarditis in Egyptian cattle. Turk J Vet Anim Sci 2010; 34: 143-153.
[4] Torki E, Dezfoli M, Sasani F, Baghban F, Shahabi M, Motaghinejad M. Traumatic reticulo-pericarditis (TRP) in sheep: a report of 4 cases in a herd. Slov Vet Res 2011; 48(2): 45-50.
[5] Ducharme NG. Surgery of the bovine forestomach compartments. Vet Clin North Am Food Anim Pract 1990; 6(2): 371-397.
[6] Hajighahramani S, Ghane M. Traumatic reticuloperitonitis in cattle of Khorramabad (Center of Lorestan Provenience, West of Iran). Global Vet 2010; 5: 135-139.
[7] Radostits OM, Gay CC, Hinchcliff KW, Constable PD. Veterinary medicine. 10th ed. Philadelphia: W. B. Saunders; 2007, p. 337-344.
[8] Ward JL, Ducharme NG. Traumatic reticoluperitonitis in dairy cattle. J Am Vet Med Assoc 1994; 204: 874-877.
[9] Braun U, Gansohr B, Flückiger M. Radiographic findings before and after oral administration of a magnet in cows with traumatic reticuloperitonitis. Am J Vet Res 2003; 64: 115-120.
[10] Venkataramanan R, Selvan P, Sreekumar C. Bovine traumatic reticuloperitonitis (TRP) and its surgical management-a report of two cases. Intas Polivet 2010; 11: 204-205.
[11] Ramin AG, Hashemi M, Asri-Rezaie S, Batebi E, Tamadon A, Ramin S. Prediction of traumatic pericarditis in cows using some serum biochemical and enzyme parameters. Acta Vet (Beograd) 2011; 61: 383-390.
[12] Alsaad KM. Evaluation of hemogram, haptoglobine and clotting indices in cattle affected with acute and chronic peritonitis. J Anim Vet Adv 2011; 10: 11-17.
[13] Niehaus AJ. Rumenotomy. Vet Clin North Am Food Anim Pract 2008; 24: 341-347.
10.12980/APJTB.4.2014B102
*Corresponding author: Omid Azari, Department of Clinical Sciences, Faculty of Veterinary Medicine, Shahid Bahonar University of Kerman, Kerman, Iran.
Tel: 00983413202926
Fax: 00983413222047
E-mail: omidazari@mail.uk.ac.ir
Article history:
Received 10 Mar 2014
Received in revised form 27 Mar, 2nd revised form 15 Apr, 3rd revised form 17 Apr 2014
Accepted 15 Jun 2014
Available online 28 Jul 2014
 Asian Pacific Journal of Tropical Biomedicine2014年7期
Asian Pacific Journal of Tropical Biomedicine2014年7期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- Antimicrobial activity against periodontopathogenic bacteria, antioxidant and cytotoxic effects of various extracts from endemic Thermopsis turcica
- Proteomics analysis of antimalarial targets of Garcinia mangostana Linn.
- The presence of eucalyptol in Artemisia australis validates its use in traditional Hawaiian medicine
- Jeju seaweeds suppress lipopolysaccharide-stimulated proinflammatory response in RAW 264.7 murine macrophages
- Antioxidant potential of Rumex vesicarius L.: in vitro approach
- Cytotoxicity screening of Melastoma malabathricum extracts on human breast cancer cell lines in vitro