
Treatment of ankylosing spondylitis by fire-needle therapy plus tuina manipulations
2015-05-18 09:06ZhaoJing-jun
Special Topic for 973 Program
Treatment of ankylosing spondylitis by fire-needle therapy plus tuina manipulations
Objective: To observe the clinical effect of fire-needle therapy plus tuina manipulations for ankylosing spondylitis (AS).
Spondylitis, Ankylosing; Fire-needle Therapy; Tuina; Massage
Ankylosing spondylitis (AS) is a progressive chronic inflammatory disease, characterized mainly by involvement of the spinal column and sacroiliac joint and clinically manifested by pain, stiffness, and limited motion in the lumbar region and back, spinal deformity, peripheral arthritis or extra-articular manifestations. It is a commonly type in pain induced by serological negative and progressive and ankylosing spondyloarthropathy. The incidence rate of this disease is 0.2%-0.9% in white race[1]and about 0.2%-0.4% in yellow race[2]. AS often develops gradually and usually would not endanger the life. But, serious stiffness and deformity of the joint would appear in the later stage in some patients, resulting in serious functional disturbance. The pathological position of AS is mainly in the spinal column. The pathological mode is mostly characterized by upward involvement of the lumbar vertebrae, thoracic vertebrae and cervical vertebrae. The knowledge about this disease was first recorded in Huang Di Nei Jing (Yellow Emperor’s Classic of Internal Medicine). Acupuncture, moxibustion and tuina are common conservative therapies for this disease. From 2007 to 2014, I treated this disease by fire-needle therapy plus tuina manipulations. Now, the report is given as follows.
1 Clinical Data
1.1 Diagnostic foundation
The diagnosis of AS was based upon New York criteria modified in 1984[3]: low back pain and stiffness for more than 3 months which is relieved by physical activity but not relieved by rest; limited motion in forward, backward and lateral flexion; and chest expansion smaller than the normal value of same age and gender; bilateral sacroiliitis in grade II-IV, or unilateral sacroiliitis in grade III-IV.
If the patient has the last item and one of the additional 3 items, the diagnosis of AS could be confirmed.
For some patients not in conformity with New York criteria, they could be recruited into the therapeutic scope by the diagnostic criteria of European Sondyloarthropathy Study Group (ESSG)[4]: inflammatory spinal pain or synovitis, asymmetric or predominantly of the lower limbs, plus one of the following items: positive family history; psoriasis; inflammatory bowel disease; urethritis, cervicitis or acute diarrhea within one month before arthritis; bilateral alternating pain in the buttocks; enthesopathy, and sacroiliitis.
1.2 Inclusion criteria
Pain in the low back and thigh before the age of 40; insidious onset; duration longer than 3 months; accompanied by morning stiffness, with the symptoms alleviated after activity. Those with four of the above five items could be included.
1.3 Exclusion criteria
Those not in conformity with the above two types of the diagnostic criteria or inclusion criteria; those with acupuncture contraindications of skin infection and/or bone tumor; patients with severe spinal deformity in the later stage; those complicated with other types of rheumatoid disease; mental disorder, or primary cardiac, hepatic or renal diseases; those with open injury of soft tissue and bone and joint; and pregnant women.
1.4 Statistical methods
The data were statistically analyzed by SPSS 19.0 statistical software. The enumeration data were expressed by mean ± standard deviation (x ±s), using t-test. The grading data were compared by rank-sum test. The rate was compared by Chi-square test.
1.5 Selection of cases
Totally, 49 cases were recruited, including 28 males and 21 females. During treatment, 7 cases dropped off. Finally, there were 42 cases with complete data, including 22 males and 20 females, with the age ranging from 15 to 52 years old, at the average age of 35 years old, and the duration ranging from 2 months to 15 years, at the average of 5.3 years. In the recruited 42 cases of AS patients, the findings showed erythrocyte sedimentation rate (ESR) higher than normal in 29 cases, mild anemia in 33 cases, elevated level of C reactive protein (CRP) in 27 cases, human leukocyte antigen B27 (HLA-B27) test positive in 37 cases, and sacroiliitis above grade II in 36 cases in X-ray examination of sacroiliac joint.
2 Therapeutic Methods
2.1 Tuina treatment
The patient took a prone position and the practitioner stood at one side.
First, the practitioner Rou-kneaded the bilateral spinal erectors by the palm root, for 20-30 times from the top to the bottom, from Geshu (BL 17) to Xialiao (BL 34), on the pathologic segments of the patient predominantly, to fully relax the erector spinae.
And then, Rou-kneaded the Governor Vessel and two lines of the Bladder Meridian by the thumb, from the top to the bottom for 15-20 times (Figure 1). If cord-like nodules were found, the practitioner changed Roukneading into Tanbo-plucking manipulation, to pluck the cord-like stuff for 3-5 times (Figure 2).

Figure 1. Rou-kneading manipulation

Figure 2. Tanbo-plucking manipulation
Next, An-pressing and Rou-kneading manipulations were used: piled up the palms on the pathological segments, to press and knead the Governor Vessel downward to the lumbosacral region. This method was focused on the lumbosacral region. Therefore, the lumbosacral region was An-pressed and Rou-kneaded repeatedly for 5-10 times.
After the patient was completely relaxed, the Banpulling manipulation was applied.
Chest-dilating Ban-pulling manipulation for thoracic vertebrae: in a sitting position, the patient held the neck with the ten fingers crisscrossed, and the practitioner stood behind him, to prop up the pathological segmentof the patient’s thoracic vertebrae with one knee, and hold the patient’s two elbows with two palms, for enabling the patient to do the passive movement of forward and backward extension. After the patient was completely relaxed by this movement for several times, the chest was dilated with the backward extension. The key of this method was supposed to use strength in the two hands and knee simultaneously and coordinately, and the preparatory movement of forward bending and backward extension should be increased gradually (Figure 3).

Figure 3. Chest-dilating Ban-pulling manipulation
Oblique Ban-pulling method for lumbar vertebrae: after the patient took a side lying position, with the lumbar vertebrae straightened and the lower limb under the body naturally extended, and the lower limb above the body flexed, the practitioner stood facing to the patient, and held and pushed the front part of the patient’s shoulder with one forearm and held the patient’s buttocks with the elbow of the other arm, to push slowly in the opposite direction by the coordinative strength of the two arms, for rotating the patient’s low back passively for 4-6 times. After the patient’s low back was relaxed, the patient’s lumbar vertebrae were rotated passively utmost, for a comparatively large-amplitude, then controlled and suddenly pulled. If a sound of ’crack‘ was heard, it meant the manipulation was successful. The key of this manipulation was not supposed to have a ’crack‘ sound, but to be done within the patient’s range of motion, in order to prevent the adhesion in the lumbar joints from being aggravated and also prevent the patient’s adjacent pathological vertebrae from forming a bone bridge. This technique was appropriate for the patients with AS in the early stage (Figure 4). This manipulation is prohibited for the patients with osteoporosis or bone tumors, traumatic fracture, etc.
Then, the patient took a prone position and the practitioner An-pressed the patient’s spine column with the palm forcefully downward, from the top to the bottom for 10 times, on the lumbar region and pathological region predominantly (Figure 5).
Finally, the patient took a prone position, and the practitioner applied the relaxing manipulations, such as Rou-kneading with palm, Na-grasping and Kouji-tapping manipulations. At last, applied Ca-scrubbing manipulation to the lumbosacral region till a heat sensation appeared in the sick area.

Figure 4.Oblique Ban-pulling manipulation

Figure 5. An-pressing manipulation
Precautions: In the application of this manipulation, it is necessary to increase the force gradually, and it is prohibited to use the strength violently or suddenly. It is particularly necessary to be careful in An-pressing the thoracic segment. In the application of Ca-scrubbing manipulation, it is necessary to use Vaseline as a medium and use the force quickly and penetratingly, to avoid scraping the skin in the sick area.
2.2 Pricking puncture by fire needle
The fire-needle therapy was given after rest for 5 min after tuina manipulation.
Acupoints: Jizhong (GV 6), Mingmen (GV 4), Yaoyangguan (GV 3), Kunlun (BL 60), Ashi points, and Jiaji (EX-B 2) points of the corresponding pathological segments.
Operation: After the patient took a sitting position, He’s fire needles of 0.50 mm in diameter and 35 mm in length were selected. First, a cross was marked with the nail on the acupoint, and then the skin of the acupoint area was disinfected with 75% alcohol. The patient was told to close the eyes or look at other place during treatment, in order to reduce tension. Then, after the needle was burnt over alcohol lamp till shining white, it was quickly inserted into the selected acupoint about 0.3-0.5 cun and quickly taken out. After the needle was taken out, the needle hole was not closed. In case of bleeding, it was necessary to press the needle hole to stop bleeding.
Precautions: First, it is necessary to mark a cross with the nail on the selected acupoint, in order to prick the acupoint accurately. After disinfection, it is necessary to burn the fire needle shining white for puncture. Otherwise, it will cause serious pain during the puncture. The above acupoints need to be pricked one by one. After each puncture, the needle should be burnt shining white again, before the next puncture.
Tuina and fire-needle therapy were given once every other day. Ten days made one course. A two-day rest was needed between two courses. After treatment for six courses, the therapeutic effects were assessed.
3 Observation of Therapeutic Effects
3.1 Criteria for assessment of therapeutic effects
The therapeutic effects were assessed based upon the criteria of the therapeutic effects for AS, stipulated in 1998 National Conference on Rheumatoid Diseases of Integrated Chinese and Western Medicine[5].
Clinical recovery: The clinical symptoms basically disappeared, and the joint activity basically returned to normal level, with various laboratory examinations returned to normal or almost normal.
Remarkable effect: Four items of the efficacy indexes of morning stiffness, number of painful joints, thoracic mobility, joint tumefaction, Schober test, etc., were improved over 50%.
Effect: Four items of the above seven efficacy indexes were improved over 20%.
Failure: Not reached the above criteria or the pathological situation aggravated.
3.2 Criteria for assessment of clinical symptoms and signs
The spinal mobility was mainly assessed by two parts of the neck and chest-low back. Respectively, four indexes of forward flexion, backward extension, rightward rotation and leftward rotation were assessed by the patients themselves.
Remarkable improvement: The improvement in three of the four measurements.
Effect: The improvement in two measurements.
Failure: The improvement only in one index or no measurement.
Number of painful joints, stiffness and pain in the lumbosacral region, neck and shoulder pain, Gaenslen test (in Gaenslen test, pain as an index for assessment) were assessed by visual analogue scale (VAS). Namely, in a straight line with 0-10 marks, the end marked with‘0’ means normal, and the end marked with ‘10’ means severe condition. In the assessment, the patients were told to label on the corresponding marks of the straight line according to their subjective symptoms and signs. 0 point means normal; 1-3 points mean mild symptoms or signs and the patients could tolerate. 4-5 points mean severe symptoms or signs, influencing the patient’s sleep, and should be dealt with clinically. But, the patient could still tolerate. 4-6 points mean the symptoms or signs are very severe and the patient cannot tolerate. Before and after treatment, the patients were respectively assessed into the four levels of 0, 1-3, 4-6 and 7-19 points. After treatment, if the point was 0 or improved by two levels, it was assessed as clinical recovery. If the point was improved by only one level and did not decline to 0, it was assessed as remarkable effect. If the point was improved by only one level but did not decline to 0, or at the same level but the point declined, it was assessed as effect. If no change was present in the points or the points were increased, it was assessed as failure.
The criteria of the therapeutic effects were self-stipulated for occiput-wall distance, thoracic mobility, Schober test in accordance with the relevant literature[6-8].
Occiput-wall distance: namely, the horizontal distance between the occipital node and wall was measured, when the patient stood straightly, with the heel, buttocks and back leaning against the wall, looking straight forward. After treatment, the remarkable improvement was that the occiput-wall distance was 0-2 cm or shortened by over 2.5 cm than before treatment. After treatment, the effect was that the occiput-wall distance was 2.1-4.4 cm or shortened by 1-2.4 cm. After treatment, failure was that the occiput-wall distance was over 4.5 cm or no change happened. Thoracic mobility: namely, the difference value between the fourth rib in deep exhalation and the chest circumference in deep inhalation was measured in the patients by the chest-dilating test. The remarkable improvement was 4-5 cm or lengthened over 3 cm, and the effect was 3-3.9 cm or lengthened over 2 cm, and below 3 cm was failure.
Schober test: in the standing position, 0 was labeled on the posterior superior iliac crest level of the back midline of the patient, and 10 cm above was labeled with another mark. Then, after the patient was told tostraighten the leg and bend the body in maximum, the distance between the two spots was measured. The remarkable improvement was that the distance was 4-5 cm or lengthened by 3 cm or above, and the effect was that the distance was 3-3.9 cm or lengthened by 2 cm. The failure was below 3 cm.
Morning stiffness was assessed by time[6]: 0-0.2 h was clinical recovery. 0.3-0.4 h or shortened by 15 min was remarkable effect. 0.5-0.7 h or shortened by 10 min was effect. Longer than 0.7 h or no change in morning stiffness and even lengthened was failure.
Anemia was assessed upon the results of blood routine tests of the patients before and after treatment, mainly by hemoglobin (Hb) and red blood count (RBC). Normal Hb is 120-160 g/L in males, and 110-150 g/L in females. Normal RBC is (4.0-5.5)×1012/L in males, and (3.5-5.0)×1012/L in females. After treatment, the value that reached the normal scope was clinical recovery. After treatment, the value increased but did not reach the normal scope was effect. After treatment, no change in the value or even lower was failure.
Low-grade fever, joint tumefaction, fatigue and lassitude were assessed based upon the self-criteria stipulated in reference to VAS[9]and Bath ankylosing spondylitis disease activity index (BASDAI)[6]. By a straight line labeled with 0-10 marks, the end labeled with ‘0’ means normal situation, the end labeled with‘10’ means severe condition. In the assessment, the patients were asked to label a sign on the corresponding mark of the straight line according to the severity of their symptoms. After treatment, 0 point means clinical recovery, 1-2 points mean remarkable effect, 4-6 points mean effect, and 7-10 points mean failure.
3.3 Therapeutic results
In 42 cases, the results showed clinical recovery in 16 cases, remarkable effect in 13 cases, effect in 7 cases, failure in 6 cases, and the total effective rate was 85.7%. Moreover, no adverse reaction was noticed during treatment. After treatment, the clinical symptoms and signs of the patients were improved in different degrees. Please see Table 1 and Table 2 for concrete situation.
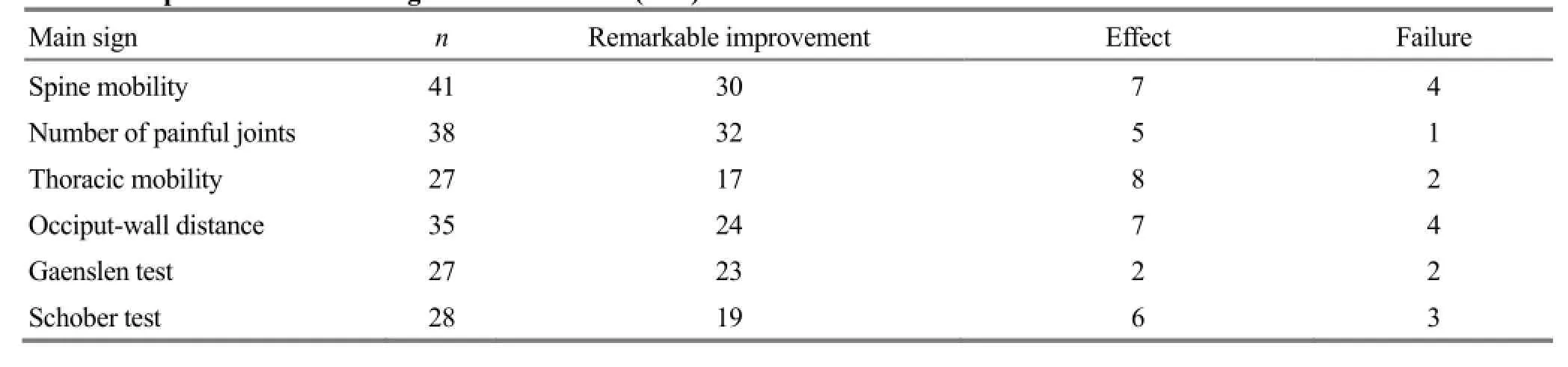
Table 1. Improvement of main signs after treatment (case)
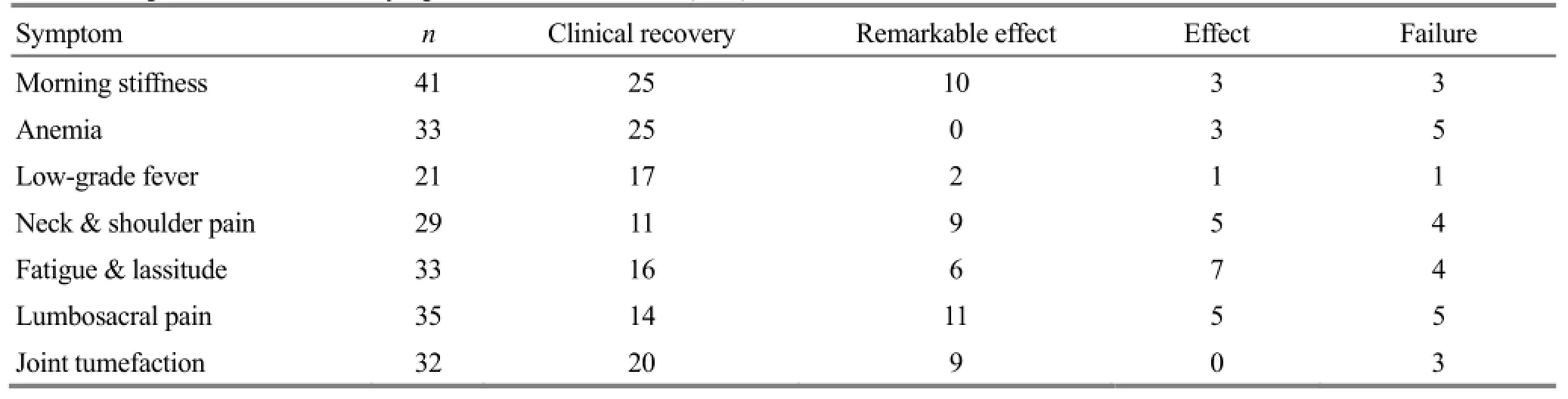
Table 2. Improvement of main symptoms after treatment (case)
4 Discussion
It is believed in Zhu Bing Yuan Hou Lun (Treatise on the Pathogenesis and Manifestations of All Diseases) that this disease is caused by invasion of wind and cold, leading to damage in blood, yin and yang. Because wind and cold are important factors to induce AS, therefore, the better therapeutic effect can be obtained by yang-warming and collateral-dredging method[10-13]. In view of the above etiology and pathogenesis of AS and characteristics of patterns, the treatment by fire-needle therapy plus tuina manipulations can restore the human anatomical relationship of the pathological change, and correct the ankylosing and deformed spinal joint and hip joint, so as to relieve spasm, lubricate the joints, active blood, disperse blood stasis, dredge the collaterals and stop pain. It has been proven by the studies[14-16]that tuina manipulations can excite the participation of endorphin system, enhance pain threshold, and canalso influence the secretion of the central 5-hydroxytryptamine (5-HT), peripheral acetyl choline (ACH) and catecholamine (CA), so as to jointly realize the analgesic effect. Fire-needle therapy is more advantageous than other needling therapies in warming the meridians, dispersing cold, dredging the meridians and activating the collaterals. In the selection of the acupoints, Jiaji (EX-B 2) points accompanying the Governor Vessel and the Bladder Meridian have the effects to regulate yin and yang, dredge the meridian and collaterals, and harmonize qi and blood[17-18]. Jizhong (GV 6) is used to treat stiffness and pain of the spine and low back. Mingmen (GV 4) and Yaoyangguan (GV 3) are used to warm the kidney and disperse cold, expel wind and remove dampness. Kunlun (BL 60) is an acupoint from the Bladder Meridian and can be used to treat back pain, activate blood and dredge the collaterals[19]. To prick the above acupoints by fire needle can promote the circulation of yang, qi and blood and relieve pain. Fire-needle therapy plus tuina manipulations can dredge the meridians, activate the collaterals, improve the nutrition in the surrounding tissues of the spine, and accelerate the restoration of the spinal joints. Particularly, Kunlun (BL 60) has the instant effect in treatment of lumbosacral pain induced by AS by pricking method of fire-needle therapy. But, its functional mechanism is unknown. This phenomenon is provided for further investigation and study.
This disease is long in duration and mostly intractable. During treatment, the patients need to sleep on the hard mattress, in order to guarantee the normal physiological curve of the spinal column. In the consideration of the diminished thoracic mobility, the patients need to do some extension persistently to resist fusion in the joints of the thoracic vertebrae.
It has been proven in the study that fire-needle therapy plus tuina manipulation has a better effect to improve the symptoms and signs of morning stiffness, fatigue and limited motion of AS patients. More importantly, no adverse reaction appeared in the patients during treatment. Because of limitation in the actual condition, the patients seeking fire-needle treatment refused to accept medications (non-steroid anti-inflammatory drugs, such as Indometacin and Nabumetone). Therefore, this study is just a simple clinical observation. I hope that we will start a more strict randomized controlled study and design the clinical observation of multiple centers and large samples for this disease, in order to find out more clinical evidence for treatment of AS by fire-needle therapy plus tuina manipulations, and also to explore the best treatment protocol of traditional Chinese medicine for AS patients.
Conflict of Interest
The authors declared that there was no potential conflict of interest.
Acknowledgments
This work was supported by the National Basic Research Program of China (973 Program, No. 2012CB518503); Self-selected Project of China Academy of Chinese Medical Sciences (No. ZZ07006). Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
Received: 30 August 2014/Accepted: 28 September 2014
[1]Braun J, Bollow M, Remlinger G, Eggens U, Rudwaleit M, Distler A, Sieper J. Prevalence of spondylarthropathies in HLA-B27 positive and negative blood donors. Arthritis Rheum, 1998, 41(1): 58-67.
[2]Huang JX, Gu JR.Ankylosing spondylitis gene mapping defined by genome search meta analysis. J Mod Clin Med Bioeng, 2006, 12(6): 10-15.
[3]Chinese Society of Rheumatology. Guidelines for diagnosis and treatment of ankylosing spondylitis. J Rheumatol, 2003, 7(10): 641-644.
[4]Huang F. Ankylosing Spondylitis. Beijing: People’s Medical Publishing House, 2011: 72.
[5]Sun GM. Observation of clinical effects of integrated therapy of Chinese and Western medicine for 20 cases of ankylosing spondylitis. Liaoning Zhongyi Zazhi, 2010, 37(11): 2210-2211.
[6]Van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum, 1984, 27(4): 361-368.
[7]Anderson JJ, Baron G, van der Heijde D, Felson DT, Dougados M. Ankylosing spondylitis assessment group preliminary definition of short-term improvement in ankylosing spondylitis. Arthritis Rheum, 2001, 44(8): 1876-1886.
[8]Wang YP, Wang XL, Liang SY, Hu J. Quantitative assessment of fatigue in the patients with ankylosing spondylitis and analysis of relevant factors. Zhonghua Wuli Yixue Yu Kangfu Zazhi, 2003, 25(3): 146-150.
[9]Van der Heijde D, Dougados M, Davis J, Weisman M H, Maksymowych W, Braun J, Hallegua DS, Bruckel J. Assessment in Ankylosing Spondylitis International Working Group and Spondylitis Association of America recommendations for conducting clinical trials in ankylosing spondylitis. Arthritis Rheum, 2005, 52 (2): 386-394.
[10]Zhang Y, Lu FQ. Treatment of 16 cases of ankylosing spondylitis by topical application in the hottest and the coldest days plus acupuncture. Shanghai Zhenjiu Zazhi, 2013, 32(2): 137-138.
[11]Li L. Clinical observation on acupuncture-moxibustion therapy in treating ankylosing spondylitis. J Acupunct Tuina Sci, 2012, 10 (5): 318-320.
[12]Zhou N, Liu FM. Treatment of 20 cases of ankylosing spondylitis by acupotomy plus herbal fumigation. Shanghai Zhenjiu Zazhi, 2013, 32(2): 136.
[13]Zhang N, Yan XP. Clinical observation on treatment of 101 cases of ankylosing spondylitis by oral administration of kidney-reinforcing and bonestrengthening formula plus topical cold Bi-impediment formula. Zhongyi Zazhi, 2013, 54(16): 1394-1397.
[14]Su SY, Huang JJ, Lei LM, Pang J, Huang XQ, Gan W. The influence on peripheral monoamine neurotransmitters in rats with acute gouty arthritis treated by tuina therapy. Guangxi Zhongyiyao, 2010, 33(6): 53-55.
[15]Ying SL. Ankylosing Spondylitis. Beijing: Chinese Medical Science and Technology Press, 2003: 58-59.
[16]Lin CX, Sun Aj, Zhao YL, Zhang LF, Ma WZ, Yu TY, Zhou PJ, Pan L, Han DW. Influence of massage on the content of β-EP and 5-HT and morphology of rabbits with soft tissue injury. Chin J Trad Med Traum & Orthop, 2009, 17(1): 20-22.
[17]Zhu YY, Ling X, Wu XH. Treatment of 30 cases with ankylosing spondylitis by acupuncture at Jiaji (EX-B 2) points. Shandong Zhongyi Zazhi, 2009, 28(11): 787-788.
[18]Chen YH. Clinical effect observation on acupuncturemoxibustion at Huatuo Jiaji (EX-B 2) points for ankylosing spondylitis. Hebei Zhongyiyao Xuebao, 2008, 23(3): 38.
[19]Yu SZ. Treatment of low back pain with Tanbo-plucking Kunlun (BL 60). Zhongyi Zazhi, 1987, 28(6): 59.
Translator: Huang Guo-qi (黄国琪)
火针点刺结合推拿手法治疗强直性脊柱炎
Zhao Jing-jun (赵敬军)
Institute of Acupuncture and Moxibustion, China Academy of Chinese Medical Sciences, Beijing 100700, China
目的:观察火针点刺结合推拿手法治疗强直性脊柱炎(AS)的临床疗效。方法:对符合纳入标准的 49 例AS 患者予以火针点刺及推拿手法治疗, 隔日治疗 1 次,10 d 为 1 个疗程,连续治疗 6 个疗程后统计疗效, 并观察临床症状及体征的变化。结果:治疗过程中,脱落 7 例。完成 6 个疗程治疗的 42 例患者中临床缓解 16 例, 显效13 例,有效 7 例, 无效 6 例。患者的各项观察指标均较治疗前有不同程度的改善,且治疗过程中未出现不良反应。结论:火针点刺联合推拿手法治疗 AS 疗效确切, 无不良反应。
脊柱炎, 强直性; 火针疗法; 推拿; 按摩
R245.3
A
Author: Zhao Jing-jun, master degree candidate. E-mail: tongchengzjj@163.com
Zhao JJ. Treatment of ankylosing spondylitis by fire-needle therapy plus tuina manipulations. J Acupunct Tuina Sci, 2015, 13 (1):15-21
10.1007/s11726-015-0816-z
Methods: A total of 49 eligible cases were treated by fire-needle therapy plus tuina manipulations, once every other day. Ten days made one course. After the continuous treatment for six courses, the therapeutic effects were summarized and the changes in the clinical symptoms and signs were observed.
Results: During treatment, 7 cases dropped off. In 42 patients who had completed treatment for six courses, the results showed clinical recovery in 16 cases, remarkable effect in 13 cases, effect in 7 cases and failure in 6 cases. The measurements of the patients were all improved in different degrees than those before treatment. Moreover, no side effect was noticed during treatment.
Conclusion: The therapeutic effect is precise and free of adverse reaction in treatment of AS by fire-needle therapy plus tuina manipulations.
猜你喜欢
中国民间疗法(2021年6期)2021-06-09
基层中医药(2020年9期)2020-11-27
中华养生保健(2020年5期)2020-11-16
基层中医药(2020年4期)2020-09-11
中国民间疗法(2020年22期)2020-01-14
中国中西医结合皮肤性病学杂志(2016年4期)2016-07-18
中医研究(2014年2期)2014-03-11
中国中医药现代远程教育(2014年19期)2014-03-01
中医研究(2013年10期)2013-03-11
 Journal of Acupuncture and Tuina Science2015年1期
Journal of Acupuncture and Tuina Science2015年1期
- Journal of Acupuncture and Tuina Science的其它文章
- Subtle adjustment of the cervical spine combined with Shu Jing Ding Xuan Decoction for cervical vertigo
- Electroacupuncture combined with traction and tuina for lumber intervertebral disc herniation
- Observation on therapeutic effect of electroacupuncture plus acupoint-injection for nerve root sciatica
- Effect of rapid point pressure on therapeutic efficacy and pulmonary function in patients with chronic persistent bronchial asthma
- Observation on the efficacy of acupoint massage plus moxibustion for refractory insomnia
- Observation on clinical effect of acupuncture plus Zi Shen Tiao Gan Decoction for perimenopausal insomnia