
在薄层及后处理CT图像上观察肺叶间裂的影像表现
2016-03-20 01:55关春爽
中国临床医学影像杂志 2016年6期
关春爽,崔 盾,崔 平,高 鹏
(北京丰台医院放射科,北京 100071)
在薄层及后处理CT图像上观察肺叶间裂的影像表现
关春爽,崔 盾,崔 平,高 鹏
(北京丰台医院放射科,北京 100071)
目的:在薄层正常肺CT及后处理图像上对叶间裂的影像解剖进行观察分析。方法:回顾性分析333例正常或基本正常肺CT,在横断位CT及多平面重组冠状位、矢状位CT及最大密度投影CT上观察叶间裂及不完整叶间裂的形态表现,对不完整叶间裂进行分型并确定缺失部位。统计分析应用SPSS 17.0。结果:三种叶间裂均完整的病例仅占20.72%。不完整叶间裂包括42.94%左斜裂,38.74%右斜裂及56.46%水平裂。93.70%不完整叶间裂缺失部位为肺门及纵隔旁。在薄层横断位CT上,表现为线影的叶间裂包括94.29%左斜裂和71.47%右斜裂,而82.58%水平裂表现为高密度带影。所有叶间裂在矢状位及冠状位CT上均表现为线影。在不完整叶间裂分型中常见类型包括左斜裂Ⅰ型、Ⅱ型,右斜裂Ⅰ型、Ⅲ型及水平裂Ⅰ型、Ⅳ型。结论:不完整叶间裂是常见变异。薄层CT扫描及后处理CT技术有助于准确识别肺叶间裂及其变异。
肺;体层摄影术,X线计算机
肺叶间裂是由脏层胸膜向肺内凹陷折叠形成的双层膜结构,将肺组织分为左肺上叶、下叶及右肺上叶、中叶和下叶[1]。随着多层螺旋CT的不断发展,及多平面重组(Multiplanar reformat,MPR)、最大密度投影法(Maximal intensity projection,MIP)后处理技术的进步,为肺叶间裂的研究提供了设备及技术基础。识别肺叶间裂及其变异有助于肺内病变的定位、疾病进展的评估、手术方式的选择、胸腔镜治疗的实施等[2-4]。因此,本文通过容积薄层CT及MPR、MIP后处理CT图像上对肺叶间裂及其变异进行研究。
1 资料与方法
1.1 一般资料
回顾性分析2014年9月—2015年3月进行容积薄层肺CT扫描的患者1 226例。排除标准包括肺、胸膜、纵隔病变,胸部手术等影响叶间裂形态改变的病例。选择肺部正常或基本正常的18岁以上患者333例,其中男170例,女163例,年龄18~89岁,平均(55.120±14.697)岁。
1.2 方法
扫描设备为64排美国通用CT(GE,Discovery CT750 HD),扫描方法为患者仰卧位吸气末屏气扫描,扫描范围从肺尖至膈肌。
扫描参数:管电压120 kV,自动管电流。层厚、层间隔均为1.25mm的连续图像。MPR重建层厚1 mm的冠状位、矢状位观察叶间裂,必要时可以采用斜位或不同层厚进行观察。MIP图像可以观察不完整叶间裂的血管来源及走行方向。观察影像的窗宽为1 500,窗位为-500,必要时可以采用不同的窗宽窗位进行观察。
由2名具有10年以上胸部诊断经验的放射科医师协商读片明确诊断。完整叶间裂定义为叶间裂连续,在任意层面均与肺门或纵隔结构相连。不完整叶间裂定义为叶间裂中断或者不能与肺门、纵隔相连,不连续部分的肺组织相互融合[2-4]。在横断位CT上叶间裂形态分为线影、乏血管带影、高密度带影及混合影像。
将不完整叶间裂分为4种类型(图1~4):Ⅰ型叶间裂不连续,呈乏血管区;Ⅱ型为邻近肺叶的血管交叉通过叶间裂区;Ⅲ型为肺内血管,特别是肺静脉穿过叶间裂区;Ⅳ型为肺静脉位于叶间裂区,而且与邻近肺叶血管相连[5]。叶间裂缺失部位根据位置分为内侧、中间、外侧及混合缺失。不完整叶间裂分型及缺失部位的诊断都通过横断位、冠状位、矢状位及MIP影像进行观察。
1.3 统计学分析
采用SPSS 17.0进行统计学分析。描述性统计用于描述叶间裂的各种比率。率的比较采用χ2检验。P<0.05表示差异有统计学意义。三重比较P<0.017表示有统计学差异。
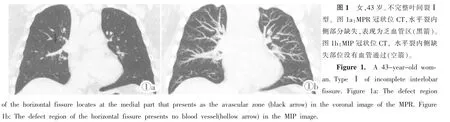
图1 女,43岁。不完整叶间裂Ⅰ型。图1a:MPR冠状位CT,水平裂内侧部分缺失,表现为乏血管区(黑箭)。图1b:MIP冠状位CT,水平裂内侧缺失部位没有血管通过(空箭)。Figure 1. A 43-year-old woman.TypeⅠ of incomplete interlobar fissure.Figure 1a:The defect regionof the horizontal fissure locates at the medial part that presents as the avascular zone(black arrow)in the coronal image of the MPR.Figure 1b:The defect region of the horizontal fissure presents no blood vessel(hollow arrow)in the MIP image.

图2 男,36岁。不完整叶间裂Ⅱ型。图2a:横断位CT,左侧斜裂内侧缺失部位见左肺上叶下舌段动脉分支(黑箭)与下肺静脉细小分支(空箭)交叉穿行。图2b:MIP横断位CT,左肺上叶下舌段动脉分支(黑箭)及下肺静脉细小分支(空箭)交叉穿过左侧斜裂缺失部位。Figure 2.A 36-year-old man.TypeⅡ of incomplete interlobar fissure.Figure 2a:The branch of inferior lingular segmental artery(black arrow)and the fine branch of inferior pulmonary vein(hollow arrow)cross over the defect region of the left oblique in the axial CT image.Figure 2b:The branch of inferior lingular segmental artery(black arrow)and the fine branch of inferior pulmonary vein(hollow arrow)cross over the defect region of the left oblique in the MIP image.

图3 男,48岁。不完整叶间裂Ⅲ型。图3a:横断位CT,右侧斜裂(箭头)内侧缺失部位见上叶后段静脉分支(黑箭)通过,左侧斜裂内侧缺失部位见细小血管分支 (白箭)通过。图3b:MIP横断位CT,右肺上叶后段静脉分支(黑空箭)通过斜裂缺失部位,左肺上叶尖后段动脉细小分支 (白空箭)通过斜裂缺失部位。Figure 3. A 48-year-old man.TypeⅢ of incomplete interlobar fissure.Figure 3a:In the axial image,the branch of the right posterior segmental vein penetrates the defect region of the oblique fissure(arrowhead),and the fine vascular branches penetrate the defect region of the left oblique fissure(white arrow).Figure 3b:The branch of the right posterior segmental vein(black hollow arrow)penetrates the defect region of the oblique fissure,and the fine vascular branches penetrate the defect region of the left oblique fissure(white hollow arrow)in the MIP image.
2 结果
2.1 叶间裂的影像表现
叶间裂的基本数据统计见表1。左斜裂、右斜裂及水平裂分别在完整、不完整及缺如叶间裂方面,不同性别间没有统计学差异。在333例患者999条叶间裂中包含522条完整叶间裂、460条不完整叶间裂及17条缺如叶间裂。3种叶间裂均完整的有69例 (20.72%)。不完整叶间裂包括42.94%左斜裂、38.74%右斜裂,56.46%水平裂。在横断位薄层CT上,所有存在的叶间裂没有表现为乏血管带的。94.29%左斜裂表现为线影,71.47%右斜裂表现为线影,82.58%水平裂表现为高密度带影。左斜裂、右斜裂及水平裂相互之间均有统计学差异(P<0.001)。在MPR的冠状位及矢状位CT上,存在的叶间裂均表现为线影,观察水平裂尤其清晰(表2)。

图4 男,61岁。不完整叶间裂Ⅳ型。图4a:MPR矢状位CT,右肺中叶内侧段静脉(黑箭)在水平裂区走行。图4b:MIP矢状位CT,右肺中叶内侧段静脉(空箭)与中叶静脉相连,沿水平裂区走行。Figure 4. A 61-year-old man.TypeⅣ of incomplete interlobar fissure.Figure 4a:The right medial segmental vein(black arrow)is observed in the defect region of the horizontal fissure in the sagittal image of MPR.Figure 4b: The right medial segmental vein(hollow arrow)connects to the middle lobar vein in the MIP image.
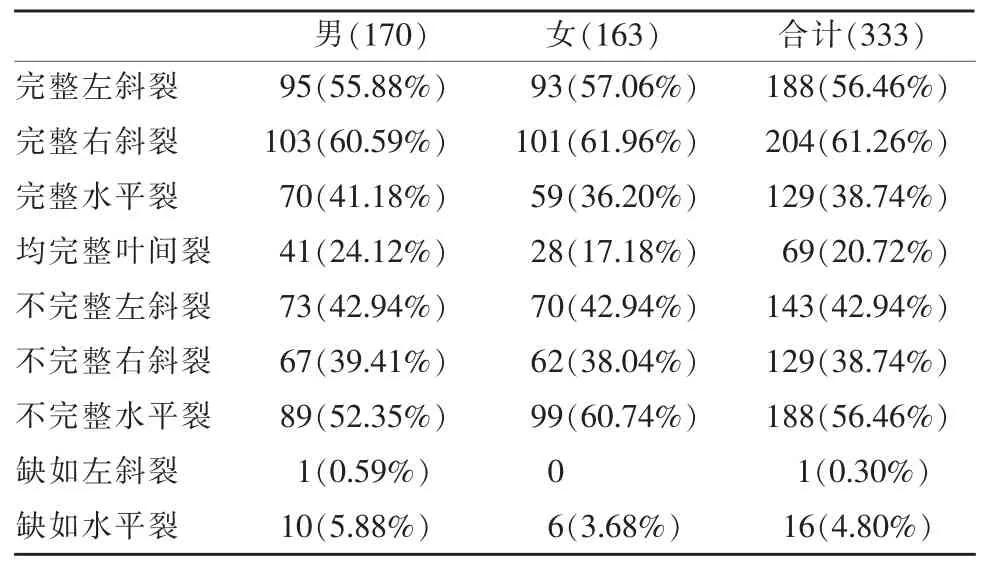
表1 肺叶间裂的基本数据
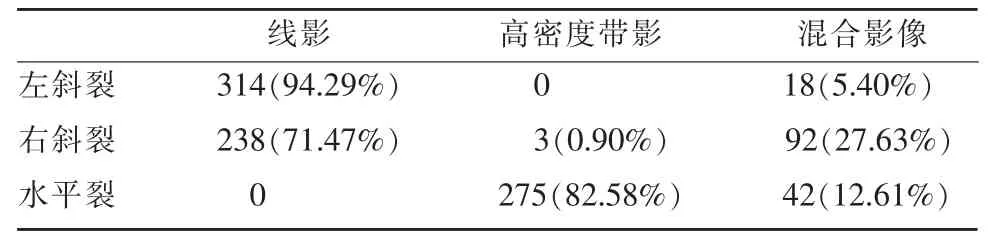
表2 叶间裂的形态表现
左、右斜裂分别出现双裂征的比例分别为25.83%(86/333)、8.11%(27/333),双侧同时出现双裂征为2.40%(8/333),水平裂没有出现双裂征。
2.2 不完整叶间裂缺失部位
在460条不完整叶间裂中,93.70%(431/460)缺失部分位于内侧缘即肺门或纵隔旁,4.78%(22/460)叶间裂中间缺失,1.52%(7/460)为混合缺失。只有水平裂存在中间缺失,在矢状位及冠状位CT上显示清晰。混合缺失为左斜裂上、下部分缺失分别3例、2例,右斜裂的上部分缺失2例(表3)。水平裂分别与左斜裂(χ2=28.320,P<0.001)、右斜裂(χ2=22.833,P<0.001)有统计学差异,而左、右斜裂之间没有统计学意义。
2.3 不完整叶间裂的分型
在460条不完整叶间裂分型中 (表4),Ⅰ型(39.78%,183/460)最常见,而Ⅲ型 (21.09%,97/ 460),Ⅳ型 (23.26%,107/460)基本相当,Ⅱ型(15.87%,73/460)最少见。MPR和MIP可以辅助观察血管来源及走行方向。水平裂分别与左斜裂(χ2= 35.880,P<0.001)、右斜裂(χ2=25.398,P<0.001)有统计学差异,而左、右斜裂之间没有统计学意义。

表3 460个不完整叶间裂缺失部位

表4 460个不完整叶间裂分型
3 讨论
肺叶间裂是重要的解剖结构,其影像研究开始于X光胸片,随后CT的出现,为叶间裂的影像与解剖对照研究提供了平台。但是标准CT扫描会丢失有价值的信息[6]。窄的准直,高空间分辨率重建算法和小视野,是提高图像质量的三种方法[7]。随着多层螺旋CT技术的提高,层厚不断变薄,分辨率不断提高以及各项同性数据的采集,基本上能与解剖相对应。目前,容积薄层CT是评价肺叶间裂最常用的方法[4,8-9]。
叶间裂在CT上可以表现为线影、乏血管带影及高密度带影。层厚10 mm的标准CT扫描时,左斜裂的乏血管带影、线影及高密度带影比例分别为58.00%~82.00%、1.00%~22.00%、0%~18.00%,右斜裂分别为60.00%~94.00%、1.00%~18.00%、0%~8.00%[2,10],而在层厚2 mm,1.25 mm或1 mm的薄层CT扫描时,文献中报道左斜裂乏血管带影、线影及高密度带影分别为 0、90.00%~98.00%、2.00%~4.00%,右斜裂分别为 0、74%~94.00%、6.00%~18.00%[2,11]。本研究与文献中的结果相一致,可见,斜裂在标准CT上常表现为乏血管带影,而在薄层CT上不会出现乏血管带影,基本上表现为线影。本研究中还发现在冠状位及矢状位CT上,叶间裂均表现为线影,观察水平裂尤其清晰。叶间裂的不同影像表现可能与CT扫描的层厚、分辨率、扫描角度及叶间裂的厚度、走行方向等相关[2,8-9]。由此可见,层厚越薄,分辨率越高,扫描角度与叶间裂越垂直,叶间裂线影越常见,高密度带影及乏血管带影越少见。在CT上还观察到叶间裂的双裂征,此征象为由呼吸运动或心脏搏动形成的运动伪影,文献中左、右斜裂及双侧斜裂同时出现双裂征的比例分别为19.0%、7.1%、7.1%[12],与本研究结果基本一致。由于左侧心尖搏动性比较大,所以左侧斜裂出现双裂征的比例较高。
通过尸检肺标本研究显示不完整叶间裂比例分别为左斜裂 7.14%~46.67%,右斜裂 36.67%~70.00%,水平裂46.88%~94.00%[13-14]。通过标准CT、高分辨率CT及薄层CT研究后发现,左斜裂为18.60%~62.50%,右斜裂为17.40%~69.73%,水平裂为20.40%~86.91%[3,5,8,15]。而本文中不完整左斜裂、右斜裂及水平裂的比例分别为42.94%、38.74%、56.46%。通过尸检肺标本及临床薄层肺CT的研究中发现水平裂是最常见的不完整叶间裂[4]。而尸检肺标本的不完整叶间裂比例基本上高于临床研究结果,这可能与肺标本的数量较少、单侧肺研究、肺的充气状态等有关。不完整叶间裂常见的好发部位为肺门及纵隔旁区[16],本研究只有水平裂出现中间部位缺失,这可能与水平裂的走行方向有关。文献中报道在不完整叶间裂的四种类型中,斜裂的缺失部位常表现为乏血管区,而水平裂的缺失部位常可见静脉穿行[3,5],而本研究发现水平裂缺失部位表现乏血管区及静脉穿行比例基本相当,因此,Ⅰ型不完整水平裂也是常见的。
文献中完整叶间裂比例分别为左斜裂40.28%~80.80%,右斜裂37.50%~82.60%,水平裂13.09%~78.20%[1,3,5,8,16], 而本研究比例分别为 56.76%、61.26%、38.74%。同时还观察到,叶间裂均完整的比例为20.72%,而文献中对此报告较少。文献中水平裂缺如3.24%[3],本研究4.80%,而且出现1例左斜裂缺如。
本文中没有就肺叶间裂的临床意义进行分析,但是文献中已经对肺叶间裂的临床价值研究很多,如肺内病变的定位、胸腔积液的分布、炎症的播散及肿瘤的侵犯、外科手术方式的选择、严重肺气肿的内镜治疗、与正常结构及病理结构的鉴别诊断等[4,8]。
总之,不完整叶间裂的好发部位是肺门及纵隔旁区,水平裂是最常见的不完整叶间裂。在容积薄层CT上,叶间裂显示为线影的几率不断提高,而MPR及MIP影像能够辅助叶间裂及其变异的诊断,为影像医师对肺内病变的定位和诊断以及临床医生对患者的进一步诊治提供依据。
[1]Gülsün M,Ariyürek OM,Comert RB,et al.Variability of the pulmonary oblique fissures presented by high-resolution computed tomography[J].Surg Radiol Anat,2006,28(3):293-299.
[2]Glazer HS,Anderson DJ,DiCroce JJ,et al.Anatomy of the major fissure:evaluation with standard and thin-section CT[J].Radiology,1991,180(3):839-844.
[3]Hermanová Z,Ctvrtlík F,Herman M.Incomplete and accessory fissures of the lung evaluated by high-resolution computed tomography[J].Eur J Radiol,2014,83(3):595-599.
[4]Koenigkam-Santos M,de Paula WD,Owsijewitsch M,et al.Incomplete pulmonary fissures evaluated by volumetric thin-section CT:semi-quantitative evaluation for small fissure gaps identification,description of prevalence and severity of fissural defects[J].Eur J Radiol,2013,82(12):2365-2370.
[5]Mahmut M,Nishitani H.Evaluation of pulmonary lobe variations using multidetector row computed tomography[J].J Comput Assist Tomogr,2007,31(6):956-960.
[6]Wei Q,Hu Y,MacGregor JH,et al.Automatic recognition of major fissures in human lungs[J].Int J Comput Assist Radiol Surg,2012,7(1):111-123.
[7]Yildiz A,Golpinar F,Calikoglu M,et al.HRCT evaluation of the accessory fissures of the lung[J].Eur J Radiol,2004,49(3): 245-249.
[8]Cronin P,Gross BH,Kelly AM,et al.Normal and accessory fissures of the lung:evaluation with contiguous volumetric thinsection multidetector CT[J].Eur J Radiol,2010,75(2):e1-8.
[9]Schieman C,MacGregor JH,Kelly E,et al.Can preoperative computed tomography of the chest predict completeness of the major pulmonary fissure at surgery?[J].Can J Surg,2011,54(4): 252-256.
[10]Proto AV,Ball JB Jr.Computed tomography of the major and minor fissures[J].Am J Roentgenol,1983,140(3):439-448.
[11]薛贞龙,李一鸣,李澄,等.16层螺旋CT薄层及后处理影像显示肺叶间裂[J].中国医学影像学杂志,2013,21(7):539-542.
[12]Mayo JR,Müller NL,Henkelman RM.The double-fissure sign: a motion artifact on thin-section CT scans[J].Radiology,1987, 165(2):580-581
[13]Murlimanju BV,Prabhu LV,Shilpa K,et al.Pulmonary fissures and lobes:a cadaveric study with emphasis on surgical and radiological implications[J].Clin Ter,2012,163(1):9-13.
[14]Meenakshi S,Manjunath KY,Balasubramanyam V.Morphological variations of the lung fissures and lobes[J].Indian J Chest Dis Allied Sci,2004,46(3):179-182.
[15]OzmenCA,NazarogluH,BayrakAH,etal.Evaluationof interlobar and accessory pulmonary fissures on 64-row MDCT[J].Clin Anat,2010,23(5):552-558.
[16]徐冰,迟永堃,李晓婷,等.64排螺旋CT观察肺裂变异[J].中国医学影像技术,2011,27(5):975-978.
Pulmonary fissures presented on thin-section and reconstructed CT images
GUAN Chun-shuang,CUI Dun,CUI Ping,GAO Peng
(Department of Radiology,Beijing Fengtai Hospital,Beijing 100071,China)
Objective:To analyze the imaging manifestations of interlobar fissures on thin-section and reconstructed CT images.Methods:Three hundred and thirty-three patients were scanned by thin-section CT.Interlobar fissures were observed on axial CT images and reconstructed CT images by multiplanar reformat(MPR)and maximal intensity projection(MIP).The interlobar fissures were characterized by lines,bands,avascular zones,and mixed imaging on the axial CT.The incomplete interlobar fissures were categorized into four types,and the locations of incompleteness were confirmed.Results:Only 20.72% showed fully complete interlobar fissures in all the three types of interlobar fissures.The cases with incomplete fissures included 42.94%of left oblique fissures(LOFs),38.74%of right oblique fissures(ROFs),and 56.46%of horizontal fissures(HFs).The incomplete parts of interlobar fissures were most likely near the hilar or mediastinal region.On the axial CT,no interlobar fissures with avascular zones,94.29%of LOFs appeared as lines,71.47%of ROFs appeared as lines,and 82.58%of HFs appeared as bands.All the interlobar fissures appeared as lines on the coronal and sagittal CT.In classifications of incomplete interlobar fissures,typesⅠ andⅡ were the most frequently observed in LOFs,typesⅠ andⅢ in ROFs,and typesⅠ andⅣ in HFs.Conclusion:Incomplete interlobar fissures are common manifestation on thin-section CT.The techniques of thin-section CT and post-processing techniques can assist in the recognition for interlobar fissures and their variations.
Lung;Tomography,X-ray computed
R563;R814.42
A
1008-1062(2016)06-0403-04
2015-10-28;
2015-11-29
关春爽(1980-),女,河北唐山人,主治医师。E-mail:guanchunshuang@163.com
崔盾,北京丰台医院放射科,100071。E-mail:cuidun_cd@163.com
猜你喜欢
颈腰痛杂志(2022年2期)2022-04-27
中医正骨(2022年1期)2022-04-18
昆明医科大学学报(2022年1期)2022-02-28
医学研究杂志(2021年6期)2021-07-09
中华肩肘外科电子杂志(2020年1期)2020-12-20
中华肩肘外科电子杂志(2020年1期)2020-08-24
中国临床医学影像杂志(2019年1期)2019-04-25
初中生世界(2018年22期)2018-11-30
中国骨与关节杂志(2018年11期)2018-11-20
山西文学(2014年8期)2014-08-22
