髋部骨折老年患者发生严重术后谵妄的多因素分析
2017-02-08 05:37张利萍郭向阳赵一鸣
中国微创外科杂志 2017年1期
魏 滨 张 华 徐 懋 李 民 王 军 张利萍 郭向阳 赵一鸣 周 方
(北京大学第三医院麻醉科,北京 100083)
·临床论著·
髋部骨折老年患者发生严重术后谵妄的多因素分析
魏 滨 张 华①徐 懋 李 民 王 军 张利萍 郭向阳 赵一鸣①周 方②*
(北京大学第三医院麻醉科,北京 100083)
目的 探讨髋部骨折老年患者发生严重术后谵妄的危险因素。 方法 回顾性分析我院骨科2005年1月~2014年12月572例髋部骨折老年患者接受内固定手术的临床资料,对性别、年龄、术前内科合并症、术前卧床时间、手术方式、麻醉方式、手术时间和术中出血量进行单因素分析,多因素logistic回归模型分析髋部骨折老年患者发生严重术后谵妄的危险因素。 结果 25例发生严重术后谵妄(25/572,发生率4.4%)。单因素分析结果显示年龄和麻醉方式有统计学差异(P<0.05);多因素logistic回归分析显示年龄(OR=1.12,95%CI:1.05~1.19,P=0.001)和全身麻醉(OR=5.03,95%CI:2.10~12.04,P=0.000)是髋部骨折老年患者发生严重术后谵妄的独立危险因素。 结论 年龄和全身麻醉是髋部骨折老年患者发生严重术后谵妄的独立危险因素。
老年患者; 髋部骨折; 术后谵妄
髋部骨折多见于老年人,伴随人口老龄化,越来越多的老年人遭受这一疾病的困扰[1]。谵妄是髋部骨折老年患者常见的术后并发症,严重的谵妄不仅危害老年人的身心健康,增加医疗成本,甚至增加老年人的术后病死率,术后谵妄越来越引起人们的关注[2~4]。我们采用回顾性研究分析我院2005年1月~2014年12月髋部骨折老年患者接受内固定手术后住院期间发生严重术后谵妄的危险因素,旨在为临床工作提供依据和指导。
1 临床资料与方法
1.1 一般资料
选取2005年1月~2014年12月我院收治的髋部骨折572例,男205例,女367例。年龄(78.7±6.9)岁。均为低能量损伤,右侧316例,左侧256例。术前卧床等待手术时间中位数4 d(1~31 d)。术前无内科合并症91例,合并心脏疾患149例,肺部疾患55例,脑血管疾患119例,原发性高血压307例,糖尿病134例。
病例入选标准:年龄≥65岁;影像学检查诊断为髋部骨折,未合并其他部位骨折;接受内固定手术;受伤机制为低能量损伤。排除标准:临床资料不完整;病理性骨折;晚期肿瘤患者;术前谵妄、意识混乱。
1.2 方法
1.2.1 病例收集 查阅我院骨科2005年1月~2014年12月收治的髋部骨折患者的临床资料,由2名工作人员依据入选标准和排除标准共同完成病例的收集工作,见图1。对于符合入选标准的患者分别记录性别、年龄、术前主要内科合并症、术前卧床时间、手术方式、麻醉方式、手术时间和术中出血量,记录发生术后严重谵妄的情况。
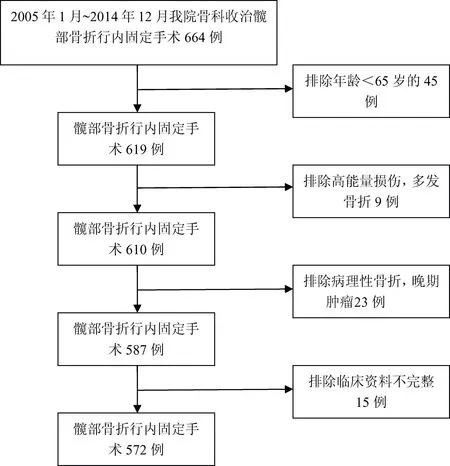
图1 病例入选流程图
1.2.2 麻醉和手术方法 手术方式均为骨折复位内固定,分为髓外内固定术(动力性髋螺钉)和髓内内固定术(股骨近端骨髓内钉)。采用气管插管全身麻醉和区域阻滞麻醉2种不同方法。
1.3 观察指标
以患者是否发生严重术后谵妄作为观察指标。谵妄的诊断标准参照美国精神病学协会编订的《精神病的诊断和统计手册》[5]:①急性起病,病情波动;②注意力不集中;③思维无序;④意识水平改变。如果患者特征①和特征②存在, 加上特征③或④的任意一条,即可诊断谵妄。将需要药物治疗的术后谵妄定义为严重术后谵妄。
1.4 统计学分析
2 结果
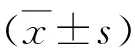
内固定手术后25例发生严重术后谵妄,发生率4.4%(25/572)。对25例发生严重术后谵妄的老年患者进行单因素分析显示:患者年龄和麻醉方式有统计学差异(P<0.05),性别、术前卧床时间、术前内科合并症、手术方式、术中出血量和手术时间无统计学差异(P>0.05),见表1。以是否发生严重术后谵妄为因变量,年龄、性别、麻醉方式、术前卧床时间、术前内科合并症、术中出血量和手术时间等为自变量,进行多因素logistic回归分析,结果显示年龄和全身麻醉是患者发生严重术后谵妄的独立危险因素,见表2。
3 讨论
老年人多伴有骨质疏松和躯体活动能力下降,跌倒等轻微外伤极易导致髋部骨折的发生[6],而接受髋部骨折手术的老年人又是发生术后谵妄的高危人群[7]。本研究结果显示髋部骨折老年患者严重术后谵妄的发生率为4.4%(25/572),年龄和全身麻醉是发生严重术后谵妄的独立危险因素。术后谵妄的发生率4%~65%[8],这种差异产生的原因可能与研究中病例纳入标准、术前医疗干预措施、患者手术类型、样本量等诸多因素有关。本研究对术后严重谵妄病例的纳入标准严格,对于症状轻微的患者,考虑到临床工作中并不需要特殊的医疗干预,疾病往往也具有自限性,故对这类病人未纳入研究;另外,受限于回顾性研究,术后病程记录对于意识状态的描述是筛选术后谵妄病人的唯一依据, 这可能是

变量发生严重术后谵妄(n=25)未发生严重术后谵妄(n=547)t(χ2,Z)值P值年龄(岁)*83.2±6.578.5±6.8t=3.3860.000性别χ2=0.7570.384 男11 194 女14 353术前卧床时间(d)*3(1~17)*4(1~31)*Z=-0.4210.674术前内科合并症 心脏合并症9140χ2=1.3440.246 肺部合并症253χ2=0.0780.779 脑血管合并症7112χ2=0.8220.365 原发性高血压16291χ2=1.1220.290 糖尿病3131χ2=1.9030.168手术方式χ2=0.0270.868 髓内固定术261 髓外固定术23486麻醉方式χ2=16.1780.000 全身麻醉17163 区域阻滞麻醉8384手术时间(min)72±1974±23t=-0.4280.669术中出血量(ml)158±55155±63t=0.2340.815
*数据以中位数(最小值~最大值)表示
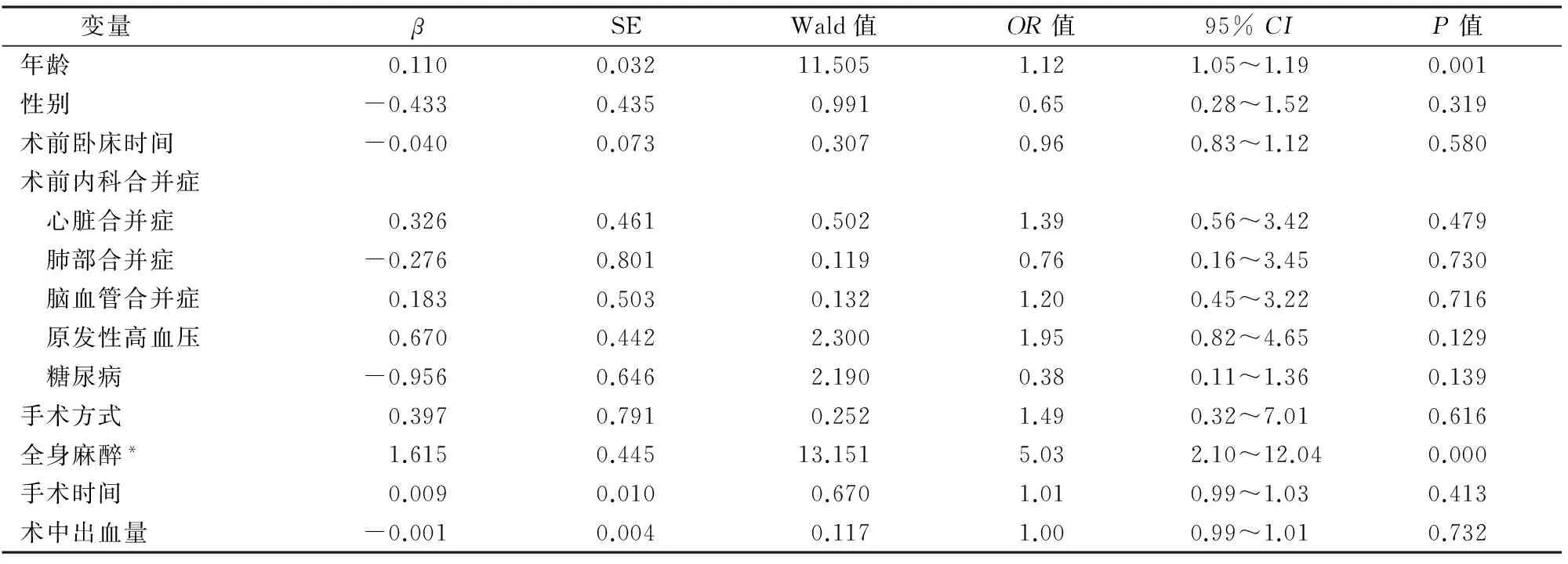
表2 髋部骨折老年患者发生严重术后谵妄相关危险因素的多重logistic回归分析结果
*以区域阻滞麻醉为参照
导致本研究术后严重谵妄发生率低的原因。手术类型的差异也会影响术后谵妄的发生率,短小手术发生率低,复杂手术发生率高[9,10]。对于髋部骨折,髋关节置换术较骨折复位内固定术创伤大、手术时间长、出血多,同时髋关节置换术还可能涉及骨水泥植入综合征、术后低氧血症等诸多问题,因此,髋关节置换术较内固定手术增加患者术后谵妄的发生率[11]。本研究未纳入接受髋关节置换术的老年人,可能也是产生术后谵妄发生率差异的原因。
老年人随着年龄增长,器官功能日渐减退,给手术和麻醉安全带来一定的风险。因此,髋部骨折的治疗模式渐渐从“骨折”为中心转变为以“高龄患者”为中心[12]。本研究结果显示年龄OR=1.12,95%CI:1.05~1.19,P=0.001,提示年龄是髋部骨折老年人发生严重术后谵妄的独立危险因素。高龄是术后谵妄的高危因素已达成共识[13],伴随年龄的增长,一方面老年人的中枢神经系统功能逐渐退化,另一方面躯体生理功能的改变也会影响到中枢神经系统的功能[14],最终导致高龄患者易于并发术后谵妄。麻醉方式的差异对术后谵妄的影响仍然存在争议[15],本研究多因素logistic回归分析结果显示全身麻醉OR=5.03,95%CI:2.10~12.04,P<0.001,提示全身麻醉是髋部骨折老年人发生严重术后谵妄的独立危险因素。全身麻醉会涉及抗胆碱能药物、麻醉性镇痛药和镇静催眠类药物,这些药物会诱发老年人术后谵妄的发生[16~18]。除此之外,髋部骨折的老年人常常术前合并多种系统性疾病,全身麻醉会影响围术期血流动力学的稳定性,增加老年人心脑血管意外的风险。髋部骨折,特别是股骨粗隆间骨折,术前可能存在大量的隐性失血,若叠加病人术前禁食水等因素,全身麻醉后极易出现因有效血容量不足导致的低血压,术中长时间持续的低血压更会导致大脑低灌注,出现脑组织缺血缺氧,从而易出现术后认知功能的改变。常规气管插管全麻增加肺部感染的风险,而肺部感染导致的低氧血症又是谵妄的诱发因素[19]。因此,对于合并重要脏器功能受损而接受手术治疗的髋部骨折老年患者,区域阻滞麻醉可能是更好的选择。
本研究结果显示性别不是髋部骨折老年人出现严重术后谵妄的危险因素,性别对于老年人术后谵妄发生率的影响仍然存在争议,有研究[20,21]显示性别是发生术后谵妄的危险因素,男性病人更容易出现术后谵妄,推测可能与男性人群中普遍存在吸烟、酗酒等不良嗜好,且治疗依从性差有关。众所周知,谵妄的发生是多种因素造成的,术前营养状况、体重指数、术后低氧血症、疼痛和低体温等都与术后谵妄有相关性[22],本研究受限于回顾性病例分析,并未探讨上述因素,有待于进一步研究。
综上所述,年龄和麻醉方式是髋部骨折老年患者发生严重术后谵妄的独立危险因素,对高龄患者应行全面的麻醉和手术风险评估,提供合适的麻醉方法,才能有效降低严重术后谵妄的发生。
1 White SM, Griffiths R. Projected incidence of proximal femoral fracture in England: a report from the NHS Hip Fracture Anaesthesia Network (HIPFAN). Injury,2011,42(11):1230-1233.
2 McDaniel M,Brudney C. Postoperative delirium: etiology and management. Curr Opin Crit Care,2012,18(4):372-376.
3 Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. N Engl J Med,2012,367(1):30-39.
4 Gunther ML, Morandi A, Ely EW. Pathophysiology of delirium in the intensive care unit. Crit Care Clin,2008,24(1):45-65.
5 American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington DC: American Psychiatric Association, 2013.596.
6 Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int,2004.15(11):897-902.
7 Smith T, Hameed Y,Cross J, et al. Assessment of people with cognitive impairment and hip fracture: a systematic review and meta-analysis. Arch Gerontol Geriatr,2013,57(2):117-126.
8 Rudolph JL, Marcantonio ER. Postoperative delirium: acute change with long-term implications. Anesth Analg,2011,112(5):1202-1211.
9 Sethi S, Ghai B, Ram J, et al. Postoperative emergence delirium in pediatric patients undergoing cataract surgery-a comparison of desflurane and sevoflurane. Pediatric Anesthesia,2013,23(12):1131-1137.
10 Wolters AE, Slooter AJC, Kooi AWVD, et al. Cognitive impairment after intensive care unit admission: a systematic review. European Journal of Intensive Care Med,2013,39(3):376-386.
11 White SM, Moppett IK, Griffiths R. Outcome by mode of anaesthesia for hip fracture surgery. An observational audit of 65 535 patients in a national dataset. Anaesthesia,2014,69(6):224-230.
12 Lawrence VA, Hilsenbeck SG, Noveck H, et al. Medical complications and outcomes after hip fracture repair. Arch Intern Med,2002,162(18):2053-2057.
13 Bickel H, Gradinger R, Kochs E, et al. Incidence and risk factors of delirium after hip surgery. Psychiatr Prax,2004,31(7):360-365.
14 Watne LO, Torbergsen AC, Conroy S, et al. The effect of a pre- and postoperative orthogeriatric service on cognitive function in patients with hip fracture: randomized controlled trial(Oslo Orthogeriatric Trial). BMC Med,2014,12:63.
15 Rashiq S,Vandermeer B,Abou-Setta AM,et al.Efficacy of supplemental peripheral nerve blockade for hip fracture surgery: multiple treatment comparison. Can J Anaesth,2013,60(3):230-243.
16 Maldonado J. Pathoetiological model of delirium: a comprehensive understanding of the neurobiology of delirium and an evidence-based approach to prevention and treatment. Crit Care Clin,2008,24(4):789-856.
17 Radtke FM,Franck M,Lorenz M,et al. Remifentanil reduces the incidence of post-operative delirium. J Int Med Res,2010,38(4):1225-1232.
18 Royse CF,Andrews DT,Newman SN,et al. The influence of propofol or desflurane on postoperative cognitive dysfunction in patients undergoing coronary artery bypass surgery.Anaesthesia,2011,66(6):455-464.
19 魏 滨,张 华,王 军. 2种不同麻醉方法对髋部骨折老年患者术后肺部并发症发生的多因素分析.中国微创外科杂志,2015,15(4):289-292.
20 Gleason OC. Delirium. Am Fam Physician,2003,67(5):1027-1034.
21 Ashare RL, Falcone M, Lerman C. Cognitive function during nicotine withdrawal: Implications for nicotine dependence treatment. Neurophamacology,2014,76(1):581-591.
22 Culp KR, Cacchione PZ. Nutritional status and delirium in long-term care elderly individuals. Appl Nurs Res,2008,21(2):66-74.
(修回日期:2016-10-17)
(责任编辑:李贺琼)
A Multivariate Analysis of Risk Factors of Serious Postoperative Delirium in Elderly Patients Undergoing Hip Fracture Surgery
WeiBin*,ZhangHua,XuMao*,etal.
*DepartmentofAnesthesiology,PekingUniversityThirdHospital,Beijing100083,China
ZhouFang,E-mail:zhou.md@126.com
Objective To investigate the risk factors of serious postoperative delirium after hip fracture surgery in elderly patients. Methods A retrospective analysis was conducted according to the medical records of 572 elderly patients with hip fractures admitted to our hospital from January 2005 to December 2014. The age, gender, preoperative comorbidities, length of preoperative bedridden time, surgical types, anesthetic methods, operation time and blood loss were recorded. Multivariate logistic regression analysis was applied to analyze the risk factors of serious postoperative delirium after hip fracture surgery in elderly patients. Results Of the 572 patients, serious postoperative delirium occurred in 25 (25/572, 4.8%). Univariate analysis showed that the independent variables of serious postoperative delirium were age and anesthetic methods (P<0.05). Multiple logistic regression analysis showed that age (odds ratio: 1.12, 95%CI: 1.05-1.19,P=0.001) and anesthetic methods (odds ratio: 5.02, 95%CI: 2.10-12.04,P=0.000) were risk factors for serious postoperative delirium after hip fracture surgery in elderly patients.Conclusion The independent risk factors to serious postoperative delirium after hip fracture surgery in elderly patients include age and anesthetic methods.
Elderly patients; Hip fracture; Postoperative delirium
A
1009-6604(2017)01-0038-04
10.3969/j.issn.1009-6604.2017.01.011
2016-06-03)
*通讯作者,E-mail:zhou.md@126.com
①临床流行病学研究中心
②骨科
猜你喜欢
小猕猴智力画刊(2022年9期)2022-11-04
全科护理(2022年29期)2022-10-21
中老年保健(2021年10期)2021-08-24
中老年保健(2021年8期)2021-08-24
中老年保健(2021年9期)2021-08-24
中华养生保健(2020年9期)2021-01-18
护理实践与研究(2020年8期)2020-01-10
电影新作(2018年3期)2018-10-26
小学生作文选刊·低年级版(2017年2期)2017-03-06
小学生导刊(低年级)(2016年8期)2016-09-24