心境障碍
2017-10-20 07:39
中国学术期刊文摘 2017年18期
Lesch, KP; Bengel, D; Heils, A; et al.
The validity of the hospital anxiety and depression scale: An updated literature review
Bjelland, I; Dahl, AA; Haug, TT; et al.
Common polygenic variation contributes to risk of schizophrenia and bipolar disorder
Purcell, Shaun M; Wray, Naomi R; Stone, Jennifer L; et al.
Mechanisms and functional implications of adult neurogenesis
Zhao, Chunmei; Deng, Wei; Gage, Fred H
抑郁障碍的核心脑机制——基于fMRI元分析的证据
刘耀中,柳均哲,林碗君,何振宏,张丹丹,关青,罗跃嘉
双相障碍的诊疗现状及相关研究进展
王勇,赵雅娟,符浩,吴彦
浙江省15岁及以上人群精神疾病流行病学调查
石其昌,章健民,徐方忠,等
心境障碍
·编者按·
世界卫生组织将今年的世界卫生日活动主题定为“一起来聊聊抑郁症”,国家卫生计生委对近年来精神障碍的主要趋势做了总结并指出:以抑郁症为主的心境障碍和焦虑障碍患病率呈现持续上升的趋势。
2017年4月,国家卫生部公布了全国精神障碍流行病调查结果,调查数据得出我国心境障碍患病率为4.06%,按照中国人口13.8亿计算,相当于是5600万人,而且4.06%这个数字是12个月的患病率,也就是说,只是统计在过去的12个月内有没有得过心境障碍疾病,如果计算终身患病率,这个数字会变成7.37%,也就是1亿人。这次的调查并没有涉及青少年和儿童,虽然没有数据统计,但是很多精神科研究人员表示,在近五六年的时间内,儿童和青少年抑郁症的上升趋势十分惊人。
心境障碍也称情感性精神障碍,是指由各种原因引起的以显著而持久的情感或心境改变为主要特征的一组疾病。临床上主要表现为情感高涨或低落,伴有相应的认知和行为改变和有幻觉妄想等精神病性症状。包括:抑郁症、心境恶劣、抑郁障碍未特定、双向I性障碍、双向II型障碍、其他双向障碍、物质所致心境障碍、躯体疾病所致心境障碍8个二级分类,则抑郁症是心境障碍中最为常见的类型,现患病率为2.10%。目前,在临床上无法通过化验或仪器来检测诊断患者是否有心境障碍类疾病,一些检查也是为了排除其他疾病,如:甲状腺功能减退、脑部肿瘤引发的激素异常也会让人表现出抑郁的症状。出现的一些复杂的脑成像技术只用于研究领域,离真正的临床还有一定距离。心境障碍治疗方面,中重度以药物治疗为主,心理治疗和其他治疗为辅。
目前与心境障碍相关的疾病的医疗花费高昂,给社会和家庭带来沉重负担和严重危害。心境障碍的发病和病情发展除遗传和环境等因素外,可能存在更深层次的机制,目前的研究还远未阐明其具体机制,发现新的药物治疗靶点,开发更加有效、不良反应更小的药物,是人类对心境障碍的认识翻开新的篇章具有重要作用。
本专题得到专家罗跃嘉教授(深圳大学脑疾病与认知科学研究中心)、王勇教授(上海交通大学医学院附属精神卫生中心)的大力支持。
·热点数据排行·
截至2017年8月28日,中国知网(CNKI)和Web of Science(WoS)的数据报告显示,以“心境障碍(mood disorder)”“情感性障碍(affective disorder)”“恶劣心境障碍(dysthymic disorder)”“双相障碍(bipolar disorder)”“抑郁障碍(depression disorder)”为词条可以检索到的期刊文献分别为34780条与154571条,本专题将相关数据按照:研究机构发文数、作者发文数、期刊发文数、被引用频次进行排行,结果如下。
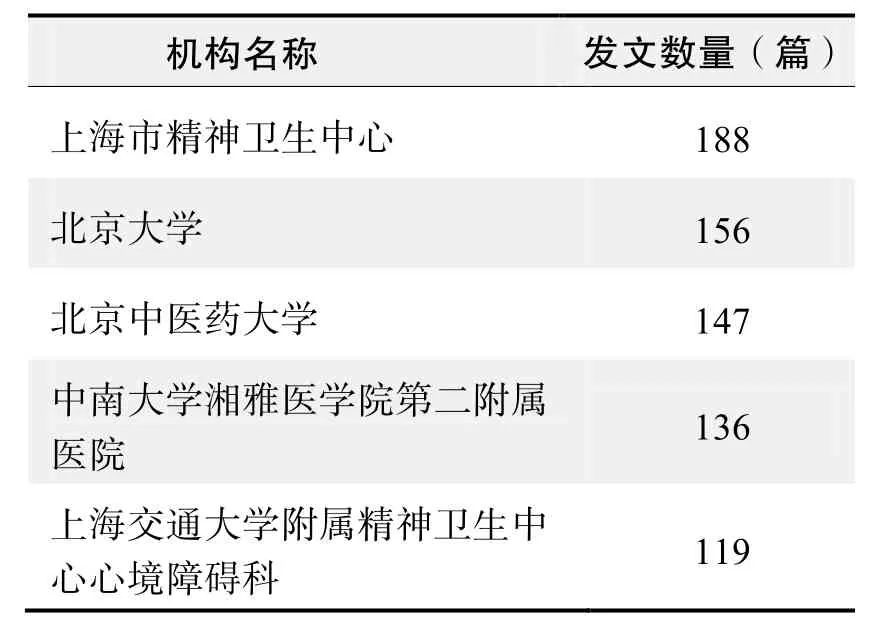
研究机构发文数量排名(CNKI)
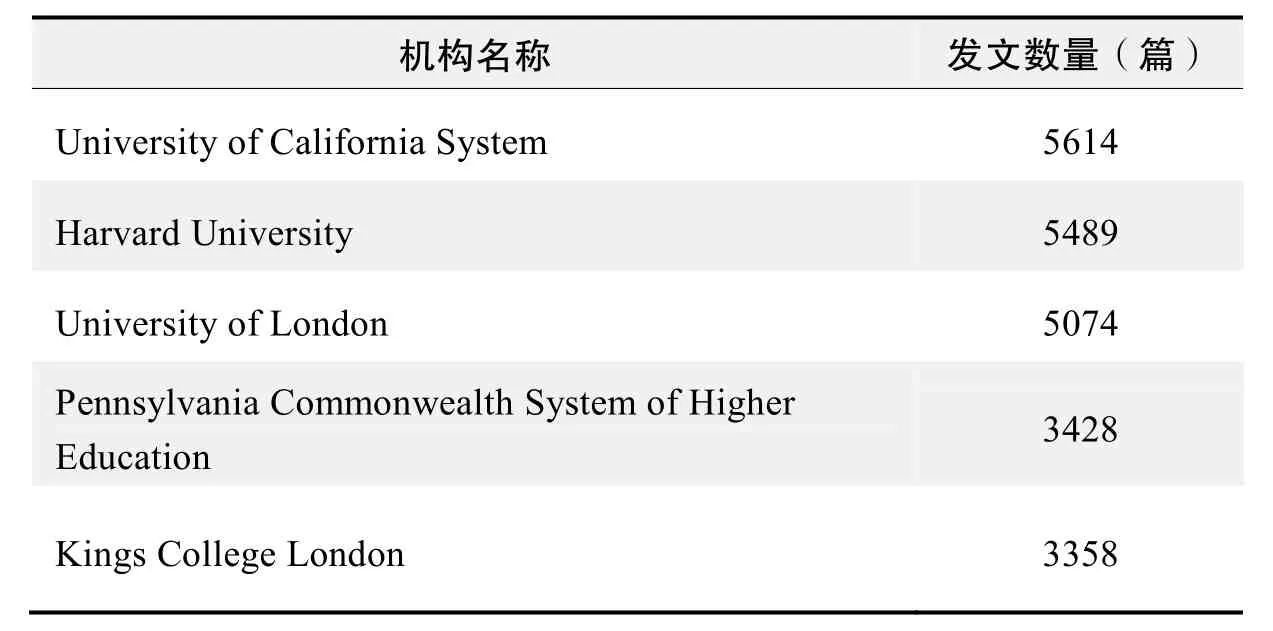
研究机构发文数量排名(WoS)
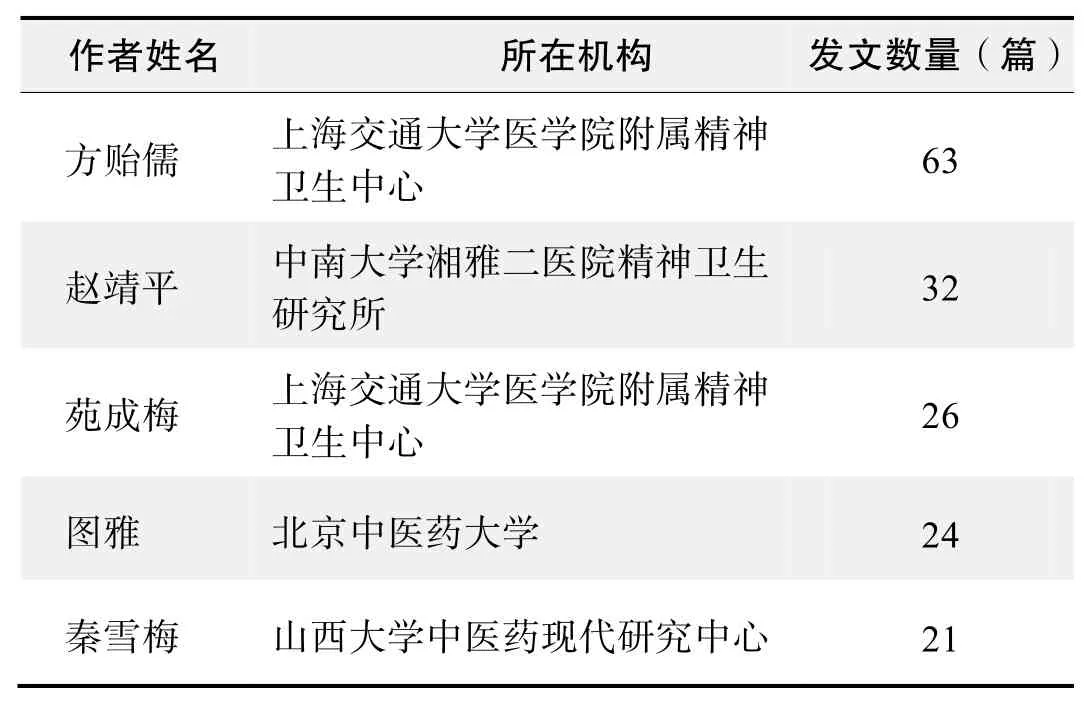
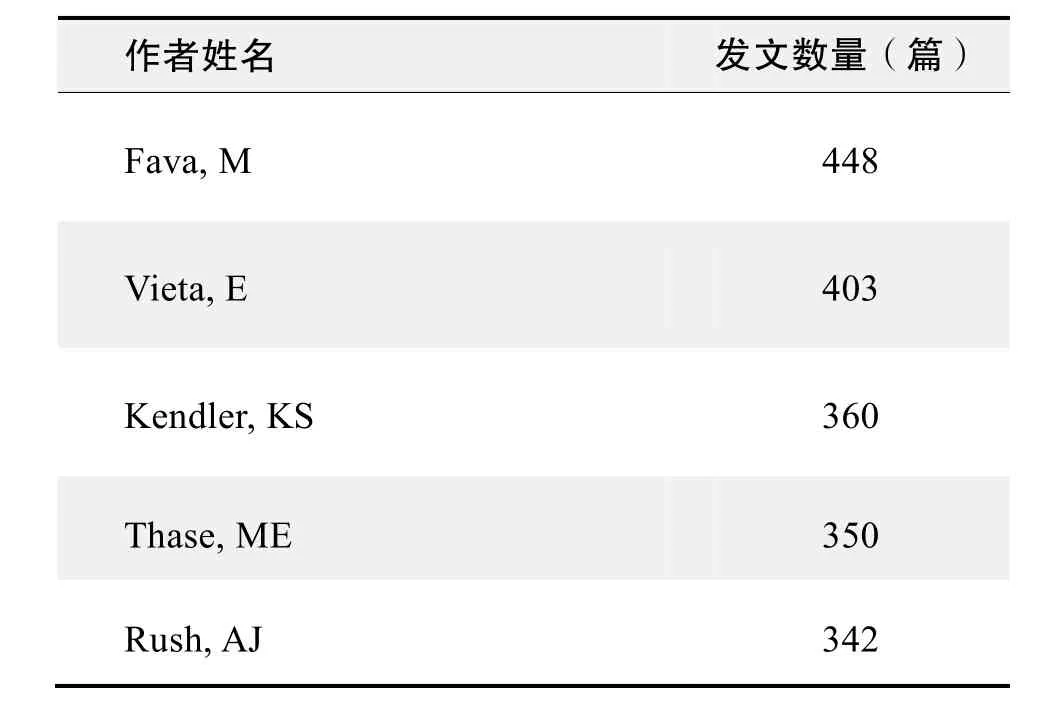
作者发文数量排名(CNKI)
作者发文数量排名(WoS)
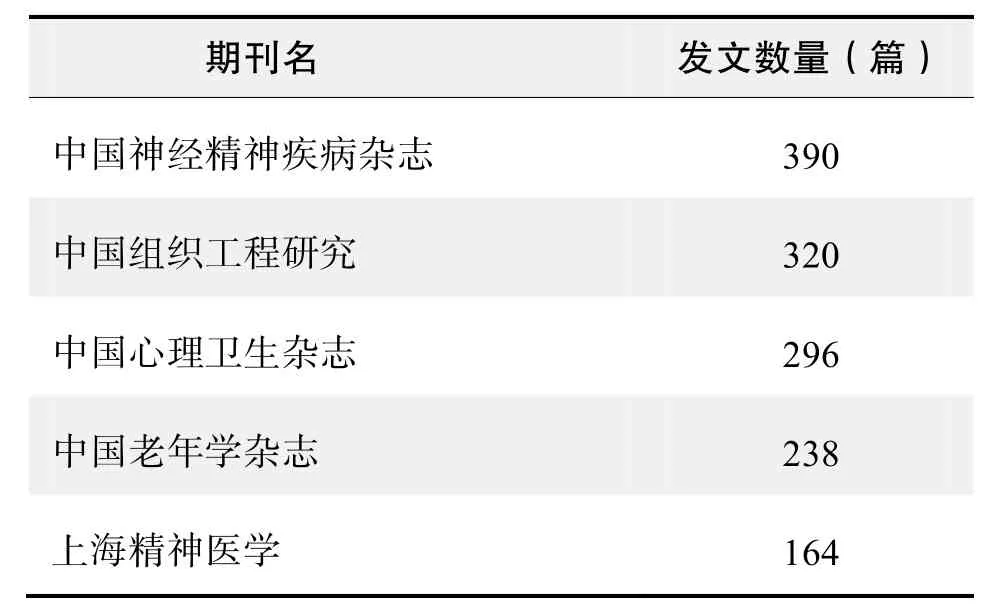
期刊发文数量排名(CNKI)
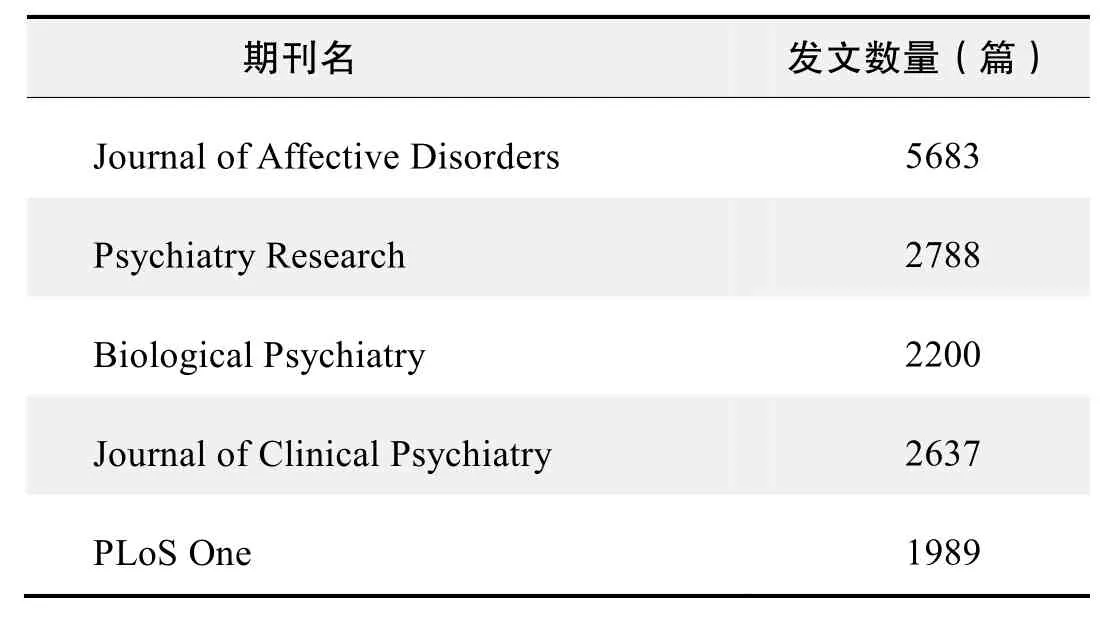
期刊发文数量排名(WoS)
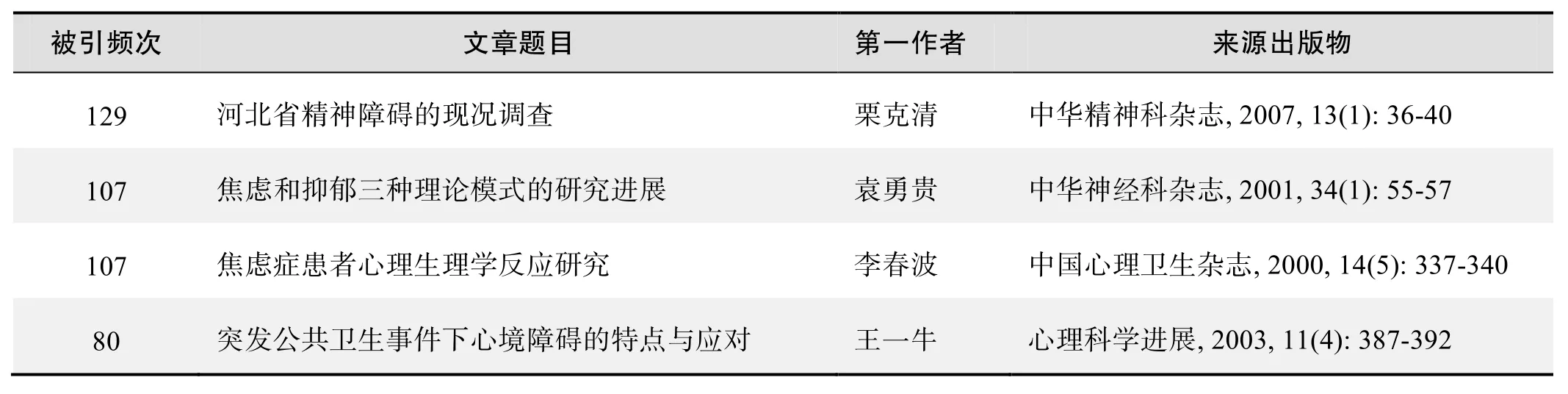
根据中国知网(CNKI)数据报告,以“心境障碍(mood disorder)”“情感性障碍(affective disorder)”“恶劣心境障碍(dysthymic disorder)”“双相障碍(bipolar disorder)”“抑郁障碍(depression disorder)”为词条可以检索到的高被引论文排行结果如下。
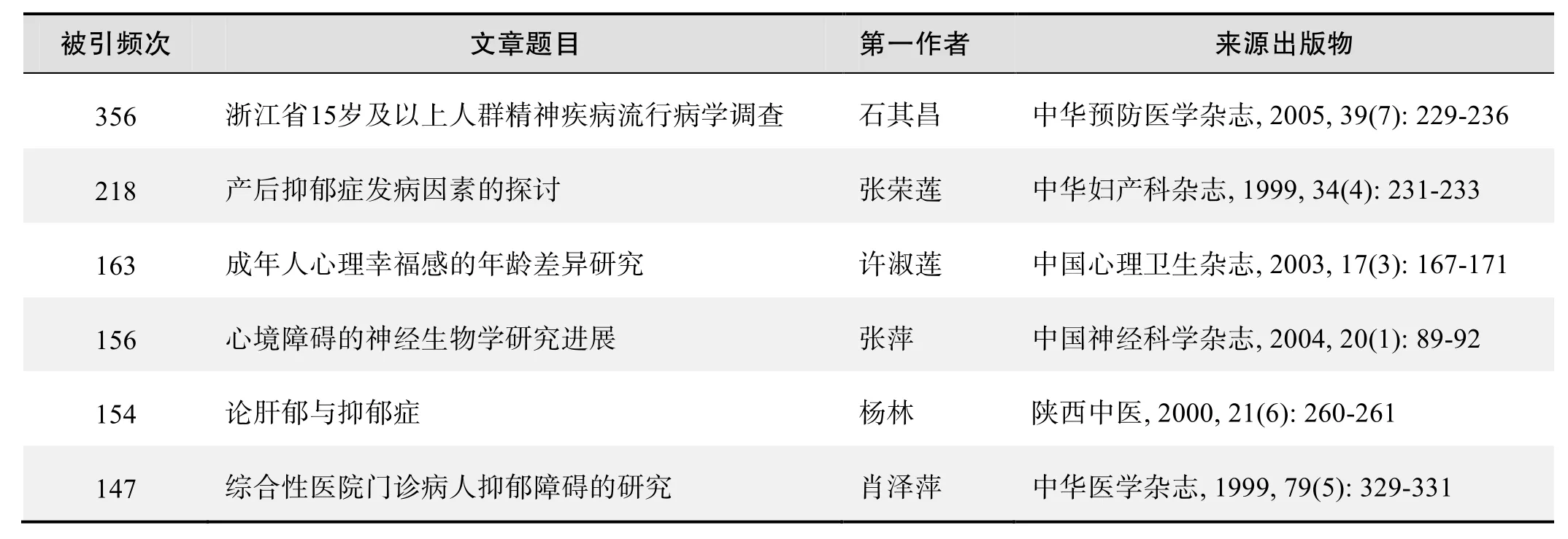
国内数据库高被引论文排行
国内数据库高被引论文排行(续表)
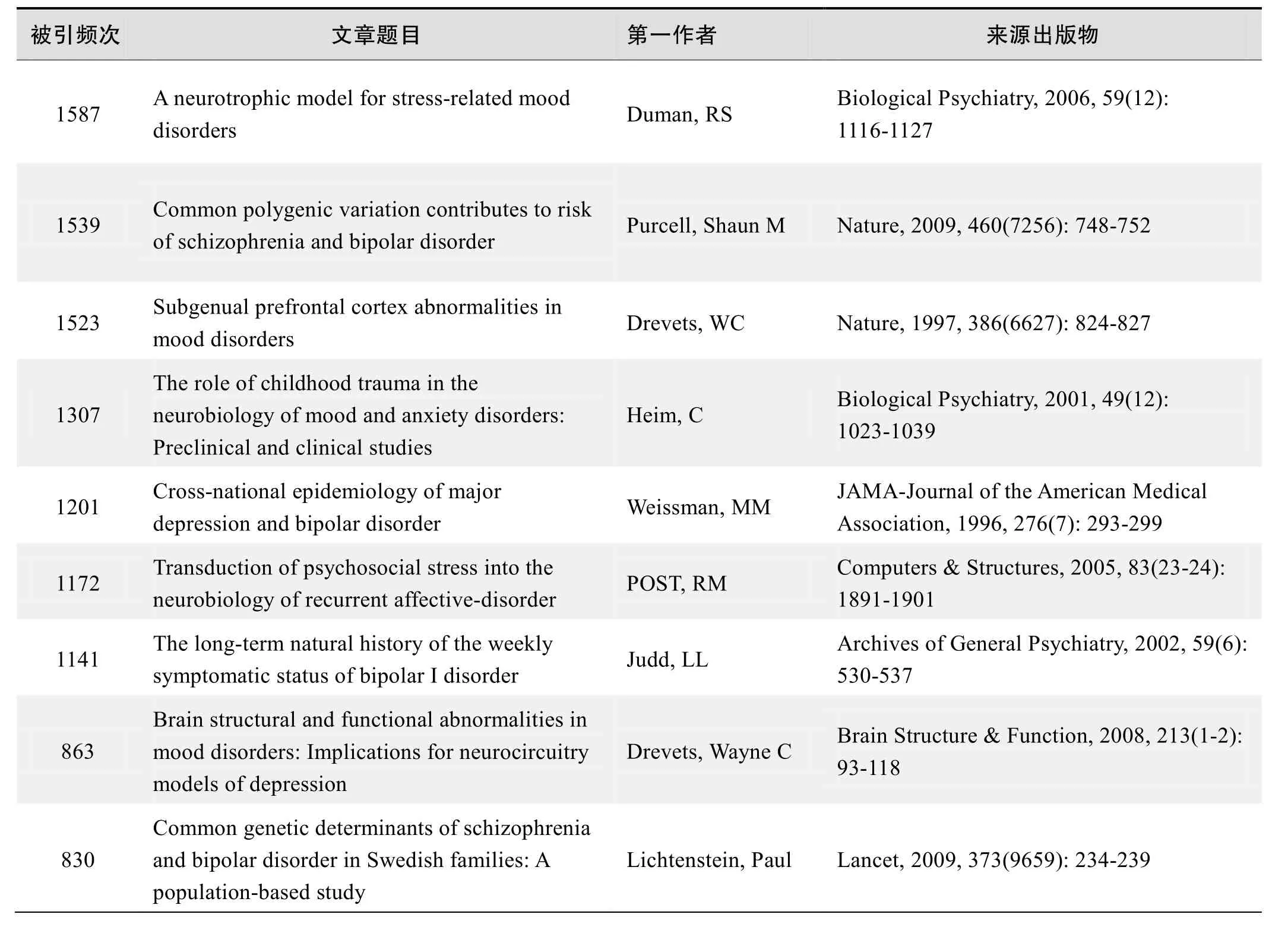
根据中国知网(CNKI)数据报告,以“心境障碍(mood disorder)”“情感性障碍(affective disorder)”“恶劣心境障碍(dysthymic disorder)”“双相障碍(bipolar disorder)”“抑郁障碍(depression disorder)”为词条可以检索到的高被引论文排行结果如下。
国外数据库高被引论文排行
·经典文献推荐·
基于Web of Science检索结果,利用Histcite软件选取LCS(Local Citation Score,本地引用次数)TOP50文献作为节点进行分析,得到本领域推荐的经典文献如下。
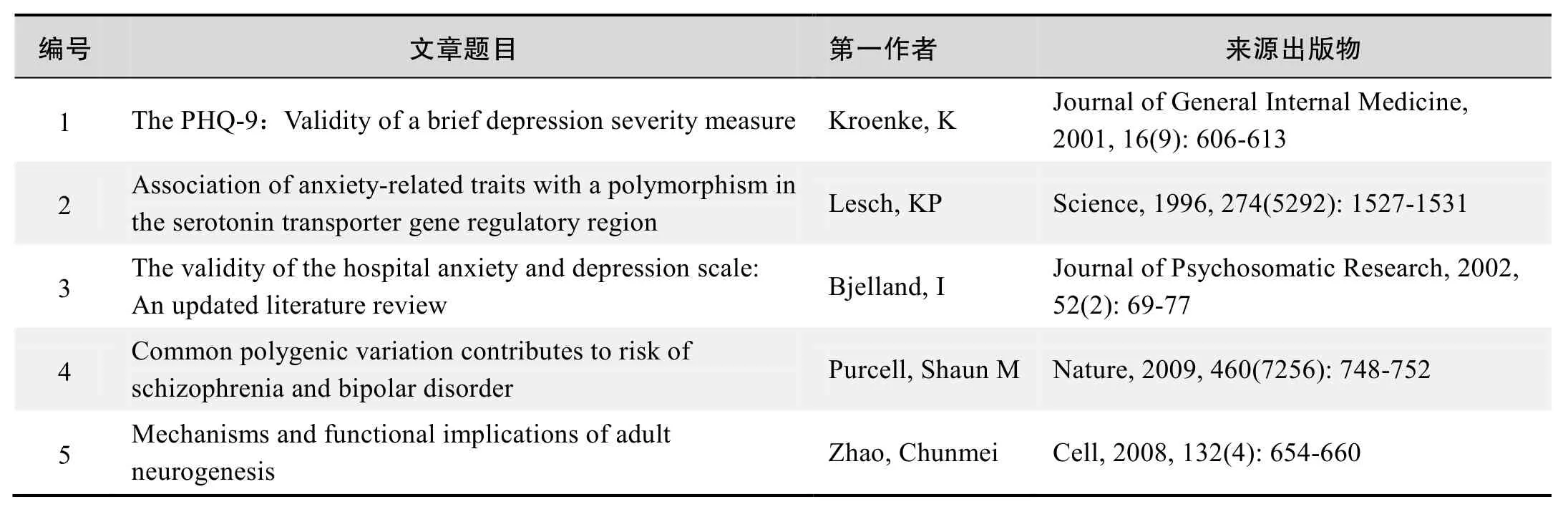
本领域经典文献
Association of anxiety-related traits with a polymorphism in the serotonin transporter gene regulatory region
Lesch, KP; Bengel, D; Heils, A; et al.
The validity of the hospital anxiety and depression scale: An updated literature review
Bjelland, I; Dahl, AA; Haug, TT; et al.
来源出版物:Journal of Psychosomatic Research, 2002,52(2): 69-77
Common polygenic variation contributes to risk of schizophrenia and bipolar disorder
Purcell, Shaun M; Wray, Naomi R; Stone, Jennifer L; et al.
Abstract:Schizophrenia is a severe mental disorder with a lifetime risk of about 1%, characterized by hallucinations,delusions and cognitive deficits, with heritability estimated at up to 80%.We performed a genome-wide association study of 3322 European individuals with schizophrenia and 3587 controls.Here we show, using two analytic approaches, the extent to which common genetic variation underlies the risk of schizophrenia.First, we implicate the major histocompatibility complex.Second, we provide molecular genetic evidence for a substantial polygenic component to the risk of schizophrenia involving thousands of common alleles of very small effect.We show that this component also contributes to the risk of bipolar disorder, but not to several non-psychiatric diseases.
来源出版物:Nature, 2009, 460(7256): 748-752
Mechanisms and functional implications of adult neurogenesis
Zhao, Chunmei; Deng, Wei; Gage, Fred H
Abstract:The generation of new neurons is sustained throughout adulthood in the mammalian brain due to the proliferation and differentiation of adult neural stem cells.In this review, we discuss the factors that regulate proliferation and fate determination of adult neural stem cells and describe recent studies concerning the integration of newborn neurons into the existing neural circuitry.We further address the potential significance of adult neurogenesis in memory, depression, and neurodegenerative disorders such as Alzheimer’s and Parkinson’s disease.
Keywords:microcells; distributed antenna systems; handoff;high speed train; mobile communications; radio over fiber
来源出版物:Cell, 2008, 132(4): 654-660
·推荐综述·
抑郁障碍的核心脑机制——基于fMRI元分析的证据
刘耀中,柳均哲,林碗君,何振宏,张丹丹,关青,罗跃嘉
抑郁症又称抑郁障碍,是情感障碍的主要类型之一其典型临床症状包括心境低落、认知功能损伤、思维迟缓、意志活动减退等。普通人群中约13%~20%有过抑郁体验,6.1%~9.5%终身抑郁;多数病例有反复发作的倾向,70%~80%的患者存在多次复发,需要终身服药。抑郁症的病因复杂,受到生物、心理和环境等多因素的影响。近年随着脑影像技术,特别是功能性磁共振(functional magnetic resonance imaging, fMRI)的发展,研究者对抑郁症背后的神经机制已经有了很多了解。
脑结构上,抑郁症患者的边缘系统,如杏仁核,海马体积往往小于正常被试,其中病人杏仁核的体积大小与抑郁症的首发年龄相关显著,首发年龄越小,杏仁核体积越小,而海马体积存在性别差异,男性患者的海马体积萎缩表现得更加明显。抑郁症患者的前额叶各部分(背外侧前额叶、腹内侧前额叶和前扣带回皮层)也存在不同程度的萎缩,其中扣带皮层体积大小与病人的愈后情况有关,拥有较大扣带皮层的患者相对扣带皮层较小的患者有更好的药物治疗结果。脑功能上,抑郁症患者的三大功能网络:认知控制网络(cognitive control network),默认网络(default mode network)和情感网络(affective network)都有不同程度的损伤。认知控制网络主要包括额叶、顶叶皮层和前扣带回皮层,负责自上而下的认知加工,如注意、工作记忆,执行功能如决策、运动检测、冲突解决等。而默认网络主要包括腹内侧前额叶,负责自我参照加工,如评估内外部线索,回忆过去和规划未来。情感网络,包括前扣带皮层的前膝部和膝下部分,下丘脑,杏仁核,内嗅皮质和伏隔核等。其通过与其他脑区的广泛连接,在恐惧、警觉、自主性神经活动中起重要作用,主要负责情绪加工。
虽然人们对抑郁障碍背后的神经机制已有了很多了解,但越来越多的实验结果并没有带来聚敛性的证据。相反,更多的脑区被发现与抑郁障碍有关。例如,利用经典的伦敦塔任务(Tower of London task),研究者发现高负荷下中等和重度抑郁症患者的背外侧前额叶表现为过度激活,而非激活减弱。一方面,这说明抑郁症的确是多维度、多层次的情感障碍,其神经机制无法由单一脑区的异常来解释。但另一方面,当前研究方法的局限性也值得考虑。单独的脑成像研究往往效果量不足,如被试量不够或有偏,容易得到假阳性结果,而不同课题组,独立实验得到的一致结果则会相对稳健,因此定量地综合分析多个研究成果以获得聚敛性实验证据即元分析(meta-analysis),显得至关重要。本文基于元分析的结果,尝试对目前尚不清楚的抑郁障碍的核心脑机制进行探讨。
当前fMRI研究的元分析方法有3种,分别为ALE(activation likelihood estimate),MKDA(multilevel kernel density analysis)和Neurosynth。前两者主要基于以往研究中激活区域一致性的程度,做出前向推论(forward inference),即辨别被试在进行某一具体认知过程中(如注意、记忆)一致激活的脑区;这两种方法主要依靠研究者手动挑选文献,流程相对繁琐,分析结果也可能存在选择偏差。而Neurosynth是由Yarkoni等人基于自然语言处理(natural language processing, NLP)和机器学习开发的无偏的全自动化分析技术,主要依靠python语言和多线程处理能力,能在短时间内完成元分析流程。Neurosynth最重要的特点是可以根据现有的脑激活模式推断相应的心理认知过程,即逆向推断(reverse inference)。相对于前向推断,逆向推断可以提供更加关键和有价值的信息。前向推断主要关注与某一特定认知过程或情绪状态相关的脑区。但值得注意的是并非所有相关脑区都特异于这个认知过程,其反映的可能是更一般的加工过程。例如,前额叶在许多认知过程中均被激活,但对特定认知过程缺乏特异性。逆向推断则弥补了这一缺陷,它能够回答“逆向推断”问题,即揭示抑郁症患者哪些脑区的异常具有诊断意义。因此,本文使用Neurosynth方法以定位抑郁障碍的特异性脑区。
1 元分析方法
本文的文献分析基于“Neurosynth”数据库。截至2014年4月13日,该数据库共有9721篇功能性磁共振成像(functional magnetic resonance imaging, fMRI)文献。本元分析的起始时间为2014年12月9日,元分析所选取文献的发表时间为1990年至2014年12月的相关文献。具体而言:1)提取坐标,通过NLP自动提取数据库中现存文献的所有激活坐标(全部转化到标准(montreal neurological institute,MNI) 2 mm空间坐标体系中);2)离析全文,根据文中关键词由使用者输入,如“depression”或近义词(如“depressive”“depressed”)的出现次数(至少出现20次)和占全文字数的比例(至少大于0.1%,即至少平均1000字中就有一个关键词出现)挑选出与关键词直接相关的所有文献;3)人工检查(排除无关文献11篇,其中没有直接比较病人与正常人的文献6篇;病人群体中不包含抑郁症患者的文献3篇;被试人数少于10人2篇),确保所挑选文献确实与抑郁症障碍相关;4)分类,根据关键词,所有的激活坐标分为两类:与抑郁障碍有关和与抑郁障碍无关;5)元分析。前向推论:类似于ALE,映射出己有抑郁障碍研究中一致激活的区域P(activation|depression)。逆向推论:根据文献分析,计算全脑每个voxel能推断抑郁障碍的后验概率(P(activation|depression))。后验概率本质是条件概率,在贝叶斯统计中,一个随机事件或者一个不确定事件的后验概率是指在考虑和给出相关证据或数据后所得到的条件概率。因此,在这里,P(activation|depression)是指在考虑activation结果时,出现depression的概率,可以理解为当出现了这种激活模式时,计算有多大概率其与抑郁症有关;6)多重校正,标准为FDR(false discovery rate)校正P<0.01,即平均而言有小于1%的voxel激活为假阳性;7)考虑到不同抑郁障碍的异质性以及抑郁与焦虑的高并发性,依照上面方法也分别进行了重度抑郁障碍(major depression disorder)(搜索关键词为“major depression”)和焦虑障碍(anxiety disorder)(搜索关键词为“anxiety”或者“anxious”)的元分析。最后确认与抑郁障碍相关的fMRI研究有307篇,其中与重度抑郁障碍有关的研究为137篇;与焦虑障碍相关的研究有252篇。
Neurosynth的逆向推断主要基于贝叶斯统计。贝叶斯流派认为概率估计需要考虑之前的信息,并根据之前的信息改变更新概率估计。例如,假设有两个事件A,B,那么事件A在另外一个事件B己经发生条件下的发生概率即为条件概率或后验概率,可以表示为P(A|B),即“在B条件下A的概率”。其计算公式为:P(A|B)=P(B|A)*P(A)/P(B)。其中P(B)和P(A)为先验概率。具体到本文Neurosynth的逆向推断中,首先通过自然语言处理离析文献,已知不同脑区激活的分布,即P(activation),同时也知道了抑郁研究的在脑成像研究的分布,即P(depression),要求的是P(activation| depression),即当出现了这种激活模式时,计算有多大概率其与抑郁症有关。
2 元分析结果
3个元分析(抑郁障碍、重度抑郁障碍和焦虑障碍)结果中均涉及的脑区包括皮层下结构—杏仁核(amygdala)、海马(hippocampus)、尾状核(caudate);皮层结构—梭状回(fusiform face area,FFA)、前扣带回(anterior cingulated cortex,ACC)、腹内侧前额叶(ventromedial prefrontal cortex,VMPFC)和背外侧前额叶(dorsolateral prefrontal cortex,DLPFC)。针对这7个脑区,分别比较了前向推论和逆向推论的结果。
针对抑郁障碍,前向推论在杏仁核、海马、尾状核、扣带前回、背外侧前额叶和腹内侧前额叶发现了最一致的激活,与前人的元分析结果一致。而逆向推论表明只有杏仁核,背外侧前额叶和腹内侧前额叶才特异于抑郁障碍。针对重度抑郁障碍,最主要的抑郁障碍亚型,本研究组也发现了类似结果:只有杏仁核,背外侧前额叶和腹内侧前额叶特异于重度抑郁障碍。有趣的是,焦虑障碍的前向推论结果与抑郁和重度抑郁障碍结果相似,逆向推论也发现了杏仁核,腹内侧前额叶的特异性,但没有背外侧前额叶。综上,与抑郁障碍直接相关的核心脑区为杏仁核、背外侧和腹内侧前额叶,而相对于焦虑障碍,最特异于抑郁障碍的异常激活脑区为背外侧前额叶。以下将重点讨论在抑郁障碍中具有推断价值的3个脑区,即杏仁核、背外侧前额叶以及腹内侧前额叶。
3 讨论
通过Neurosynth综合分析了抑郁障碍、重度抑郁障碍和焦虑障碍的相关脑区,前向推断和逆向推断结果类似。抑郁障碍的逆向推断明确的指向了3个核心脑区:杏仁核、背外侧前额叶和腹内侧前额叶。抑郁症患者的杏仁核反应过激是目前公认的结论。杏仁核是皮质下情绪加工的核心脑区,与丘脑(thalamus)相连,主要参与刺激的显著性检测(salience detection),解析刺激的情绪意义。结构上,相对于正常被试,抑郁症患者的杏仁核体积较小,且其体积与抑郁症的首发年龄显著相关。功能上,相对于正常被试,抑郁症患者的杏仁核在处理负性情绪时更加明显的激活(能达到正常人的1.7倍),且反应更加持久(持续时间为正常人的3倍)。抑郁症患者的杏仁核反应和负性情绪的强度成正比,例如,当加工面孔的悲伤程度越来越高时,患者左侧杏仁核的激活也越来越强。进一步的研究发现,杏仁核的过激活是高度自动化的,即在没有意识到负性刺激存在时,阈下情绪加工也会过度激活抑郁症患者的杏仁核,且反应强度与患者的心理健康水平成反比。
但同时,元分析结果提示,杏仁核的异常激活模式并非是抑郁症患者所独有的,其他情感障碍如焦虑症也会存在此种现象.本文的结果证明,杏仁核的功能异常也是焦虑障碍的核心脑机制之一研究发现相对于正常被试,焦虑症患者处理情绪信息,特别是负性信息时其杏仁核也会过度激活,且激活强度与焦虑障碍的严重程度成正比。静息状态下焦虑患者的杏仁核与前额叶皮层如内侧前额叶的功能连接强度降低,其连接强度与患者焦虑程度成反比。考虑到抑郁和焦虑的高并发现象,杏仁核异常激活可能是一般情感障碍的普遍神经机制,如普遍对负性刺激敏感,对负性刺激的反应过激等。
背外侧前额叶与前运动皮层、眶额叶以及外侧颖叶有丰富的双向连接,该脑区主要负责执行控制特别是抑制功能.研究发现静息状态下,相对于正常被试,抑郁症患者的背外侧前额叶活动强度偏低,且与皮质下的海马和杏仁核的功能连接强度减弱任务状态下,当执行stroop或n-back等需要执行控制能力的任务时,抑郁症患者为了达到与正常被试相同的行为成绩需要付出更大的认知努力,于是表现为更强的背外侧前额叶的激活。而当患者服用抗抑郁药物(如百忧解)后,相对于服药前,其背外侧前额叶的激活显著增强。这些结果表明,背外侧前额叶的功能异常可能是导致抑郁障碍的核心机制之一,但明确的因果关系还需借助fMRI以外的研究手段,如经颅磁刺激(ranscranial magnetic stimulation,TMS)才能确定。本文基于文献的逆向推断表明,相对于其他心境障碍,如焦虑障碍,背外侧前额叶的功能异常是特异于抑郁障碍的。脑损伤和干预方面的研究结果也支持这一结果,例如,双侧背外侧前额叶损伤的病人更可能患抑郁症,且患病程度更高,当用TMS暂时兴奋患者的背外侧前额叶时,其抑郁症状显著减轻。抑郁症患者背外侧前额叶的激活降低也常伴随着杏仁核的过度激活,更进一步的研究表明,背外侧前额叶对杏仁核的激活具有抑制功能,这种抑制功能是个体自上而下情绪调节,控制注意和记忆的核心机制。Beck认为,抑郁患者无法从负性刺激上转移注意的缺陷正是其临床症状上表现出过度反当负性体验的主要原因。元分析结果也表明,最特异于抑郁障碍的异常脑区是背外侧前额叶。因此相对于杏仁核的过度激活,抑郁患者对负性情绪的抑制能力下降可能才是最核心的问题。综上,背外侧前额叶对抑郁障碍具有临床诊断和治疗意义,该脑区功能异常可能是抑郁障碍的核心脑机制之一,针对背外侧前额叶的治疗可有效缓解抑郁症状。
另外,本文发现对抑郁症同样具有诊断意义的脑区还包括腹内侧前额叶的功能异常。腹内侧前额叶主要负责情绪整合和自我参照加工,其反向投射至下丘脑(hypothalamus),调节自动化情绪加工;投射至腹侧纹状体(ventral striatum),调节奖赏加工。另外,腹内侧前额叶还与杏仁核有丰富的双向连接,参与威胁检测和恐惧条件学习。静息状态下,抑郁症患者腹内侧前额叶与丘脑的功能连接强度显著高于正常被试,且与被试的主观负性情感感受成正比。任务状态下,当执行自我参照任务时(如判断人格形容词是否适合描述自己),抑郁症患者腹内侧前额叶的激活相对于正常被试显著减弱。抑郁症患者的腹内侧前额叶异常主要与其过度的自我关注有关。当腹内侧前额叶损伤时,病人的自我觉知能力也降低或丧失,对负性情感如羞愧、内疚、尴尬和后悔(这些均属于与自我相关的社会情绪)的感受显著降低,同时抑郁症状也显著改善。这一结果与尾核下神经束切断术(subcaudate tractotomy)结果非常吻合:切断抑郁症患者腹内侧前额叶后部与皮层下结构相连的双侧白质,显著减缓了患者的抑郁症状,术后患者体验到欣快,对自我状态漠不关心。但值得注意的是,与杏仁核的功能异常类似,腹内侧前额叶的过度激活模式也不完全特异于抑郁障碍。逆向推断结果表明,腹内侧前额叶异常也能显著推断焦虑障碍。研究发现,与抑郁症患者类似,相对于正常被试,焦虑症患者的腹内侧前额叶在静息状态时反应更强烈,与杏仁核的功能连接更弱,而在患者完成自我参照任务时激活减弱。临床上,焦虑患者和其他情感障碍患者也同样表现出对自我的过度关注和偏低的自我评价。因此,腹内侧前额叶的功能异常可能是情感障碍的共同表现。
虽然Neurosynth相对于传统元分析方法有很大进步,特别是能进行逆向推断。但是这种方法也不能完全避免元分析方法本身的不足。元分析的对象是己发表的文献结果而不是原始数据,无法保证数据结果的有效性,更无法避免文章发表的偏倚性,如阴性结果难以发表,领域冷热影响接收难度等。另外,Neurosynth只能分析其数据库收集的文献,但该数据库只包含了主流神经科学杂志(主要是英文为主的期刊),可能会忽视潜在的国别间差异。因此,本文的结论还需进一步实证研究的支持。还有,本次元分析没有考虑不同年龄发展阶段的特性,抑郁症在不同年龄段发病机制存在不同。尽管如此,仍可以看到本文基于抑郁障碍fMRI元分析的逆向推断结果与前人的fMRI研究、脑损伤研究、干预研究结果都非常吻合,对未来抑郁症脑机制的研究有一定指导意义。
综上所述,抑郁障碍核心的脑机制为杏仁核、背外侧前额叶和腹内侧前额叶的异常。杏仁核的过度激活体现了过敏化的情绪加工,而背外侧前额叶的激活减弱则体现了抑郁患者自上而下的抑制功能障碍。另外,过度激活的腹内侧前额叶是抑郁患者过度自我关注的神经机制。值得注意的是,杏仁核和腹内侧前额叶的过度激活也是焦虑障碍的核心机制,逆向推断表明这两个脑区均能推断焦虑障碍和抑郁障碍。因此本文的结果提示,相对于焦虑障碍,最特异于抑郁障碍的神经机制是背外侧前额叶的功能异常,这表明无法抑制过敏化的情绪加工是抑郁障碍的核心机制,也是导致患者过度反当负性情感的原因。本研究的主要贡献是通过对3种抑郁分型分别进行前向和逆向推断的统计分析,最终确定了最特异于抑郁症患者的一致性的脑机制损伤,即背外侧前额叶。
这对当前研究有重大的启发和指导意义,特别是当前研究中过分关注抑郁症患者杏仁核或奖赏系统缺陷,而一定程度上忽略了对抑郁症患者记忆和情绪抑制脑机制的研究。♦
【作者单位:暨南大学管理学院;北京师范大学认知神经科学与学习国家重点实验室;深圳大学情绪与社会认知科学研究所;深圳大学医学部;成都医学院四川养老与老年健康协同创新中心】
(摘自《中国科学:生命科学》2015年第12期)
双相障碍的诊疗现状及相关研究进展
王勇,赵雅娟,符浩,吴彦
双相障碍是一种严重精神疾病,具有高患病率、高复发率、高致残率、高死亡率、高共病率和低龄化的特点。目前,临床上对双相障碍的认识还不一致,其流行病学数据也有较大差异。随着“双相谱系障碍”的概念日益获得精神科医师的认可,除传统意义上的I型和II型双相障碍外,有学者提出了“软双相障碍”和“阈下双相障碍”的概念,甚至情绪不稳或烦躁等亦被归入了双相谱系障碍。从双相障碍所致疾病负担来看,在世界卫生组织1993年报告的伤残调整生命年(disability adjusted life years,DALY)减少最多的前10种疾病中,精神疾病占5种,双相障碍列第3位;中国数据显示,在DALY减少1%的前25种疾病中,双相障碍列第13位。因此,双相障碍的临床诊疗研究函待重视与加强。
1 诊疗现状
1.1 识别率低
双相障碍的识别率低。欧美国家的资料显示,患者自首次出现肯定的双相障碍临床症状后,平均要经8年才能得到确诊;在现症双相障碍患者中,69%曾被误诊为单相抑郁、焦虑障碍、精神分裂症、人格障碍和物质依赖/滥用等。
1.2 治疗率低
美国1994年的调查显示,双相障碍患者发病后平均要经10年才能得到首次治疗,50%以上的现症患者在长达5年以上的时期内未接受过治疗,其中36%甚至在长达10年以上的时期内未接受过治疗。
1.3 治疗不规范
临床医师治疗双相障碍时“乱拳迭出”,难言规范。对双相抑郁的治疗方法包括药物治疗(心境稳定剂、抗精神病药物、抗抑郁药物)、改良的电休克治疗(modified electroconvulsive therapy,MECT)和心理健康教育等。面对多样治疗选择,临床医师往往表现为无所适从,导致多种治疗方法联合应用的不合理和治疗方法的频繁更替,影响患者的预后。一项对欧洲精神科医师的调查显示,超过60%的双相障碍患者在病情稳定前至少经历了2次治疗方法变更,平均治疗方法变更次数为2.4次。
1.4 疗效不令人满意
双相障碍急性期的治疗疗效仍然不能令人满意,尤其是双相抑郁的治疗,患者的各种残留症状和社会功能损害往往较单相抑郁更常见,抗抑郁药物的不当使用也非常普遍。由于多种药物的联用和更替,导致药物不良反应问题更为突出,患者的治疗依从性亦差。而双相障碍的临床特征决定了对其维持治疗和预防复发同等重要,但此却未引起临床医师的足够重视,全病程管理措施的缺失往往导致患者病情多次反复、频繁发作,严重影响患者的社会功能。此外,双相障碍在特殊人群(如儿童、老年人、孕产妇、绝经期妇女、同时患有躯体或其他精神疾病患者)中的临床症状常不典型,影响因素也更复杂,临床识别和治疗的难度都趋增加,需要强调个体化治疗的重要性。
2 原因分析
2.1 疾病自身特点
双相障碍的临床表现复杂、症状多种多样,既有各种情感症状,又有精神病性症状、躯体症状、认知症状等,且往往与多种疾病同时存在,因此临床识别和治疗的难度较高。从纵向病程来看,双相障碍呈现躁狂、轻躁狂、抑郁、轻抑郁、混合状态、正常情绪等多种极性的无规律交替起伏变化,尤其是轻躁狂、轻抑郁与正常情绪之间很难区分,导致临床识别困难。然而,无论是躁狂发作、还是抑郁发作,都无法改变双相障碍的“永不稳定”和“反复摇摆”的疾病性质。
2.2 医疗相关因素
由于双相障碍的复杂性、相关研究发现及概念处于动态变化中和临床医师专业背景及经验的差异,综合医院和基层医院的临床医师对双相障碍的基础知识、尤其是最新进展的了解不足。即使在专科医院,不同亚专科和不同资历背景的临床医师对双相障碍的认识也有很大差异。此外,由于对双相障碍危害的认识不足、缺乏相关专业培训和受到时间紧、工作量大等客观因素的制约,双相障碍早期识别和规范化治疗的重要性往往被临床医师忽视。医疗机构对双相障碍等精神疾病知识的宣传及普及也不够。
2.3 患者相关因素
目前,精神卫生医疗资源的分布不均衡,主要集中于三级精神疾病专科医院和综合医院的精神或心身科,这些医院的临床医师或有双相障碍早期识别和规范化治疗的能力,但其他医院临床医师的专业水平不足。同时,客观条件也使得精神卫生服务的可及性受到限制。对上海地区社区居民精神卫生知识知晓率和服务需求状况的调查结果显示,尽管逾70%的居民认为精神卫生知识很重要,但近90%的居民对精神卫生信息来源渠道的便利性表示不满意。由于时间、地域、交通、经济状况等客观条件的制约,患者对精神卫生服务的需求往往得不到满足。而且,患者对双相障碍的认识往往不足,多在抑郁发作时才可能主动求医,严重躁狂发作时往往就需家属强制送医,而轻躁狂发作时又往往不认为自己有病。此外,病耻感、症状不典型(尤是双相抑郁时)、个体就医偏好(首诊于综合医院或基层医院)等因素也阻碍了双相障碍的早期识别和规范化治疗。
3 相关研究进展
3.1 识别与评估
双相障碍是一种慢性致残性疾病,《中国双相障碍防治指南(第二版)》强调了充分评估、量化监测和全病程治疗原则,建议临床上采用“基于评估的治疗(measurement-based care,MBC)”策略。MBC的实施流程应当包括筛查、初始治疗、监测疾病进展并调整治疗方案、长期监测及维持治疗4个步骤。MBC应当体现在双相障碍全病程的管理中,其中对疾病的量化评估是MBC实施的基础。目前,一些双相障碍的筛查量表已在临床上得到广泛使用,包括《犯项轻躁狂症状清单》《心境障碍问卷》《双相抑郁指数量表》《双相谱系诊断量表》《双极性指数》和简版《气质评定量表》等。有助于提高双相障碍的识别率与正确诊断率。
但是,服务对象多、成本高、流程繁琐、对临床医师要求高等因素在很大程度上制约了MBC在临床上的推广实施。近年来“移动健康(mobile health)”发展迅速,其整合了即时通讯、互联网和移动传感3项关键技术,可即时提供各种服务和信息资源,尤其适用于医疗资源不足的地区。随着新媒体技术的快速发展,电子化精神卫生服务成为对公众健康教育的主要形式之一。上海市精神卫生中心于2014年发布、上线了手机应用软件“心情温度计”,可筛查焦虑、抑郁情绪以及早期识别双相障碍,帮助心境障碍高危人群或患者自我监测情绪变化并提供医学指导或建议,宣传、普及心境障碍疾病知识,对提高公众对情绪问题和双相障碍的认识、规范临床诊疗行为将起到良好的促进作用。
3.2 诊断与治疗
有关双相障碍的诊疗问题一直备受关注。自2007年中国《双相障碍防治指南(第一版)》发布以来,双相障碍的临床诊断和治疗水平有了一定的改善,但与国际水准和现实需求还有相当的差距。2010年9月—2011年2月,中华医学会精神病学分会发起、组织了一项“中国双相障碍患者诊断评估服务”调查,对在全国13家精神卫生机构(6家综合医院的精神/心身科和7家精神疾病专科医院)中的1487例被诊断为抑郁症并正按抑郁症治疗的住院或门诊成年患者重新应用《简明国际神经精神访谈》予以诊断,结果发现双相障碍总体及I,II型双相障碍被误诊为抑郁症的比例分别为20.8%,7.9%,12.8%。美国精神医学学会出版的《精神障碍诊断与统计手册(第五版)》中除将双相障碍与精神分裂症、抑郁症等并列为大类疾病外,还有以下4个方面的变化:1)纳入了物质/药物(包括抗抑郁药物)及其他医学状况引起的双相及相关障碍,而不再作为排除标准;2)将活动增加或精力旺盛与心境高涨、易激惹并列为A类核心症状;3)明确了“其他特定的双相及相关障碍”的含义,包括有抑郁发作史的短暂轻躁狂发作(2~3 d)、有抑郁发作史的不充分轻躁狂发作症状、无抑郁发作史的轻躁狂发作和短暂环性心境(<24个月);4)以“伴混合特征”的标注替代混合发作,并增加了“伴焦虑困扰特征”等标注。随着脑科学的发展,今后双相障碍的分类诊断会更趋向于病因学诊断,会更细化和精确,与精神分裂症和抑郁症等疾病的界线会更明晰、鉴别更科学化,由此治疗也会相应地更精准。
尽管国内外发布的基于循证医学证据的双相障碍治疗指南数不少,但临床实践与治疗指南推荐的不一致现象仍很普遍。总体上看,临床医师治疗双相抑郁时与治疗指南推荐的符合率明显低于治疗躁狂发作时,治疗疾病严重程度较轻者时与治疗指南推荐的符合率也较低。中国双相障碍协作组开展的“中国双相躁狂路径调查”结果显示,在3906例双相障碍患者中,11.1%的轻躁狂、躁狂或混合发作患者的药物治疗与加拿大的双相障碍治疗指南推荐不符,而双相抑郁患者药物治疗的不符率更高达50.2%,双相障碍维持期药物治疗的不符率也达35.6%。2015年8月,《中国双相障碍防治指南(第二版)》正式问世,其更新内容参考了国际上最新的双相障碍治疗指南并结合了我国的实际情况及最新研究成果。
3.3 病因与发病机制
双相障碍的病因不明。自从全球“脑计划”研究启动以来,神经科学工作者对双相障碍、孤独症(自闭症)等被认为是最具生物学基础的精神疾病开展了全方位、多层面的病因学与发病机制探索。研究表明,遗传和环境因素对双相障碍发病均有重要影响。
但是,双相障碍的遗传方式尚不明晰,普遍认为是一种复杂的多基因遗传病。近年来,国内学者积极开展双相障碍的遗传学机制探索,多聚焦于神经营养失衡假说和神经递质紊乱假说。相关研究结果显示:1)双相障碍的易患性和临床特征与miRNA 206基因的多态性及表达水平无关;2)双相障碍的易患性和治疗疗效与脑源性神经营养因子(brain-derived neurotrophic factor,BDNF),基因的多态性rs6265相关,但与BDNF血浆浓度的相关性不明显;3)双相障碍的易患性与神经营养性酪氨酸激酶受体-2(neurotrophic tyrosine kinase receptor type 2,NTRK2)基因的多态性rs1387923相关,I型双相障碍的治疗疗效与NTRK2基因的多态性s2769605相关;4)miRNA 206与BDNF/NTRK2基因的多态性及外周表达无关。
随着神经影像学从结构影像学向功能影像学发展,我们对精神疾病的认识不再仅限于神经结构方面的显著异常,而可更多地关注各个脑区和神经环路中的更为细微的功能异常。近期,双相障碍的神经影像学研究主要聚焦于双相抑郁和单相抑郁、双相躁狂和双相抑郁、双相障碍和精神分裂症之间在各个与情绪和认知相关的脑区以及不同脑区之间连接的异同点。
此外,人们在继续研究神经递质(如5-轻色胺、去甲肾上腺素、多巴胺等)系统和神经内分泌系统(如下丘脑-垂体-肾上腺轴、下丘脑-垂体-甲状腺轴等)与双相障碍发病间的关联。近年来,神经内分泌系统以及与此相关的神经免疫学标志物(如炎性细胞因子α-肿瘤坏死因子、白介素类物质等)与双相障碍的关系成为新的研究热点。
4 小结
综上所述,双相障碍发病的生物学机制非常复杂,是生物学因素和环境因素交互作用的结果。随着研究的技术手段的不断发展以及对双相障碍临床现象学的深入研究,人们正在逐渐归纳并整理出一些相对集中的线索,这些线索的相互借鉴及验证可能有助于我们不断接近双相障碍发病的真谛,而此对临床上更规范化、个体化地治疗双相障碍也具有重要的指导意义。双相障碍治疗指南往往是基于最新的研究成果和专家建议制定出来的,因此也是现阶段最有借鉴价值的双相障碍诊疗工具,值得更好地推广应用。♦
【作者单位:上海交通大学医学院附属精神卫生中心】
(摘自《上海医药》2017年第7期)
·高被引论文摘要·
被引频次:356
浙江省15岁及以上人群精神疾病流行病学调查
石其昌,章健民,徐方忠,等
目的:了解浙江省15岁以上人群各类精神疾病的时点患病率和分布特点,为制定全省精神卫生规划提供科学依据。方法:2001年9至12月采用多阶段分层整群抽样方法随机抽取14个县(市)、70个乡镇(街道)、140个村(居委会)中15000名≥15岁的人为调查对象,由精神科护士用扩展的一般健康问卷(GHQ12)将调查对象分为患精神疾病高、中、低危险组,然后由精神科医生以美国精神障碍诊断标准(DSMIV)依次对100%、40%、10%的调查对象进行定式检查(SCID),对各类精神障碍进行诊断。结果14639人完成筛选,4788人完成诊断。调整后精神疾病总时点患病率为17.3%(95%CI为16.0%~18.7%),除外各类未特定障碍后,总时点患病率下降至13.4%(12.2%~14.7%)。最常见的疾病为心境障碍(8.6%,7.9%~9.5%)、焦虑障碍(4.3%,3.6%~5.1%)和物质使用障碍(3.0%,2.4%~3.8%)。最常见的特定精神疾病为重性抑郁障碍(4.3%,3.7%~4.9%)、酒精使用障碍(2.9%,2.3%~3.7%)、心境恶劣障碍(1.6%,1.3%~1.9%)和特殊恐怖症(1.2%,0.8%~1.8%)。总患病率农村高于城市(RR=1.23,95%CI为1.11~1.37),女性略高于男性(RR=1.11,1.00~1.22)。结论:精神障碍是严重影响浙江省社会经济发展的、迫切需要解决的公共卫生问题,有必要在全省范围内开展和实施全面性的精神卫生规划并定期评估其效果。
精神障碍;流行病学研究
来源出版物:中华预防医学杂志, 2005, 39(7): 229-236
被引频次:218
产后抑郁症发病因素的探讨
张荣莲,陈起燕,李艳华,等
摘要:目的:探讨产后抑郁症的发生率及其影响因素。方法:随机抽取在本院产前门诊初诊并决定在本院分娩的1052例孕妇进行医院焦虑及抑郁情绪自评量表调查,其中以艾迪产后抑郁量表(EPDS)跟踪调查至产后7 d内共866例。结果:EPDS阳性率为15.01%(130/866,并用单因素和多元逐步回归分析了产后抑郁症的影响因素,发现孕妇健康状况、孕期夫妻关系、分娩时医务人员的态度、丈夫企盼生男孩的程度及孕妇孕期听课次数、孕期焦虑情绪及抑郁情绪等7个因素与产后抑郁症发生的关系最密切,其中孕期听课次数与产后抑郁症的发生呈负相关,余6项均与产后抑郁症呈正相关。结论:孕期焦虑和抑郁情绪是发生产后抑郁症的最主要因素。
关键词:抑郁症;产后;病因学
来源出版物:中华妇产科杂志, 1999, 34(4): 231-233
被引频次:163
成年人心理幸福感的年龄差异研究
许淑莲,吴志平,吴振云,等
摘要:目的:了解成年人心理幸福感的年龄差异和有关因素。方法:采用Ruff的心理幸福感量表对777名20~94岁的人进行测查。结果:1)量表的信度合格,与抑郁症患者反映的差异显著。2)6个分量表除自主性无明显年龄差异外,个人成长较年青组均高于较年长组;与他人积极关系及生活目的较年青三组均高于老老年组;环境掌握中年组与老年组高于老老年组;自我接受老年组显著高于青年组。3)自主性、个人成长、生活目的和自我接受分均男性显著高于女性,与他人的积极关系分女性稍高于男性。4)影响心理幸福感的因素,青年组以工作学习、教育程度、疾病和心境,中年组以工作学习量、婚姻状态以及人际交往,老年组以心境、健康情况,老老年组则以心境、人际交往、疾病情况、教育程度、家庭关系等因素为主;5)与美国比较,个人成长结果基本一致;中国人生活目的、自我接受评价较低,可能受我国传统的中庸之道影响。结论:心理幸福感受年龄影响,量表从积极心理功能角度考虑是合理的,但对除婚姻外的家庭关系涉及过少。
关键词:健康心理学;心理幸福感;年龄差异;断面调查;成人;中国人;美国人
来源出版物:中国心理卫生杂志, 2003, 17(3): 167-171
被引频次:156
心境障碍的神经生物学研究进展
张萍,王雪琦
摘要:近年的研究发现,心境障碍患者在脑、神经细胞和信号分子水平都存在异常。边缘-丘脑-皮质环路和边缘-皮质-纹状体-苍白球-丘脑环路参与了心境障碍行为的发生,这些部位的糖代谢和脑血流量、皮质容量、神经元和胶质细胞的数量和形态均发生改变,同时心境障碍患者脑内磷酸肌醇环路、Wnt信号通路和神经营养因子下游信号转导通路也有相应变化。
关键词:心境障碍;边缘-丘脑-皮质环路;边缘-皮质-纹状体-苍白球-丘脑环路;神经元;胶质细胞;信号转导
来源出版物:中国神经科学杂志, 2004, 20(1): 89-92
被引频次:154
论肝郁与抑郁症
杨林
摘要:认为抑郁症系情志致病,结合现代医学和祖国医学的病理生理理论论述其原发在肝,兼及脾肾,初期多实,久病兼虚。基本病机为肝气郁结,贯穿疾病始终。提出从肝郁辨证分型,调肝为主,兼顾他脏,结合辨病用药,身心并治的治疗模式。
关键词:忧郁病/中医药疗法;辨证论治;中医学术发掘
来源出版物:陕西中医, 2000, 21(6): 260-261
被引频次:147
综合性医院门诊病人抑郁障碍的研究
肖泽萍,严和骏,肖世富,等
摘要:研究综合性医院门诊病人抑郁障碍的患病率、识别和诊治状况。方法以两步筛选法,对15个国家或地区共26969例门诊病人进行了GHD-12,GHQ-28、复合式国际诊断检查(CI-DI)、内科医生检查表等测定。在上海市共有583例完成以上量表测定,男、女比例分别为38.0%和62.0%。结果在检查出的所有心理问题中,抑郁障碍患病率居首位;总样本抑郁症和心境恶劣的患病率分别为10.4%和2.1%。上海市则分别为4.0%和0.6%;上海市内科医生对抑郁障碍的识别率为21%,远低于15个国家资料的中位数55.6%;内科医生对抑郁障碍的治疗不充分,在上海市内科医生未给予检出病人任何抗抑郁剂治疗。结论在综合性医院的内科病人中,抑郁障碍是最常见的心理障碍。但抑郁障碍多未被内科医师检出且治疗不充分。内科医生的精神医学知识再教育应受到全社会的重视。
关键词:抑郁障碍;门诊病人
来源出版物:中华医学杂志, 1999, 79(5): 329-331
被引频次:129
河北省精神障碍的现况调查
栗克清,崔泽,崔利,等
摘要:目的:了解河北省≥18岁人群各类精神障碍的患病率和分布特点。方法:2004年10月至2005年3月采用多阶段分层整群抽样方法随机抽取≥18岁人群,共24000名,以美国精神障碍诊断与统计手册第4版(DSM-Ⅳ)轴Ⅰ障碍定式临床检查患者版进行调查,用DSM-Ⅳ对各类精神障碍进行诊断。结果:(1)患病率:20716人完成调查,精神障碍的时点患病率为162.43‰[95%可信区间(95%CI)为15.8%~16.7%],排在前三位的是重性抑郁障碍(27.01‰)、未特定的焦虑障碍(25.09‰)和心境恶劣障碍(23.12‰);终生患病率为185.12‰(95%CI为18.0%~19.0%),排在前3位的是重性抑郁障碍(47.47‰)、酒精依赖性和滥用性障碍(38.62‰)和未特定抑郁障碍(25.51‰)。(2)时点患病率:女性(167.95‰)高于男性(156.95‰),农村(165.63‰)高于城市(144.31‰),P<0.05~0.01;并随年龄的增长而不断上升,其中30~49岁为137.17‰~156.71‰,50~≥70岁为201.44‰~285.41‰。结论:河北省精神 疾病的患病率较高,其中女性和农村的患病率高;重性抑郁障碍是省内患病率最高的精神疾病。
关键词:精神障碍;流行病学方法;河北
来源出版物:中华精神科杂志, 2007, 13(1): 36-40
被引频次:107
焦虑和抑郁三种理论模式的研究进展
袁勇贵,张心保,吴爱勤
摘要:焦虑和抑郁是临床上常见的两组症状,二者常同时存在。目前,关于焦虑和抑郁的关系不外有三种观点:(1)一元论:即连续谱论,认为焦虑和抑郁是同一疾病的不同表现形式;(2)二分论:认为焦虑障碍和抑郁障碍是两种不同性质的疾病;(3)共病论:认为焦虑和抑郁共存时,是一种不同于焦虑障碍或抑郁障碍的独特的疾病实体。
来源出版物:中华神经科杂志, 2001, 34(1): 55-57
被引频次:107
焦虑症患者心理生理学反应研究
李春波,吴文源,何康梅,等
摘要:目的:探讨焦虑症患者心理生理学指标的特点。方法:对31例焦虑症患者和23名健康志愿者应用多导电生理仪对模拟应激前后的心理生理学指标进行检测,并在治疗1月后复查。结果:焦虑症患者的心率及低频峰功率显著高于对照组,其心理生理学指标在治疗前后无显著性差别;低频峰功率与高频峰功率比值(静息状态)、脉搏图血流量面积变化(模拟应激前后)与HAMA分数变化呈负相关。结论:焦虑症患者存在交感神经系统功能亢进,可能是一种特性标志,一些心理生理学指标与临床疗效有一定的相关性。
关键词:焦虑症;心理生理学;模拟应激
来源出版物:中国心理卫生杂志, 2000, 14(5): 337-340
被引频次:80
突发公共卫生事件下心境障碍的特点与应对
王一牛,罗跃
摘要:突发公共卫生事件会给较大范围的人群造成相当的心理压力和情绪问题。突发事件发生时,社会心理因素对突发事件控制效果和进程的影响越来越显著,因疫情、疾病、生活、工作以及社会和人际关系等因素而致的情绪问题非常突出。突发事件时情绪问题的表现有疑病、恐慌、焦虑、抑郁和强迫心理等,对此应采取相应的对策,而不同群体如罹患人群、隔离人群、家属、普通就医者及一般公众的情绪问题有其独特的表现和应对措施。突发事件为情绪问题的研究提供了广阔的前景。
关键词:突发公共卫生事件;重症急性呼吸综合征(SARS);心境障碍;心理应对
来源出版物:心理科学进展, 2003, 11(4): 387-392
被引频次:1587
A neurotrophic model for stress-related mood disorders
Duman, RS; Monteggia, LM
Abstract:There is a growing body of evidence demonstrating that stress decreases the expression of brainderived neurotrophic factor (BDNF) in limbic structures that control mood and that antidepressant treatment reverses or blocks the effects of stress.Decreased levels of BDNF,as well as other neruotropbic factors, could contribute to the atrophy of certain limbic structures, including the hippocampus and prefrontal cortex that has been observed in depressed subjects, Conversely, the neurotrophic actions of antidepressants could reverse neuronal atrophy and cell loss and thereby contribute to the therapeutic actions of these treatments.This review provides a critical examination of the neurotropbic hypothesis of depression that has evolved from this work, including analysis of preclinical cellular(adult neurogenesis) and behavioral models of depression and antidepressant actions, as well as clinical neuroimaging and postmortem studies.Although there are some limitations, the results of these studies are consistent with the hypothesis that decreased expression of BDNF and possibly other growth factors contributes to depression and that up-regulation of BDNF plays a role in the actions of antidepressant treatment.
Keywords:antidepressant; depression; neurogenesis;behavior; BDNF; VEGF
来源出版物:Biological Psychiatry, 2006, 59(12):1116-1127
被引频次:1539
Common polygenic variation contributes to risk of schizophrenia and bipolar disorder
Purcell, Shaun M; Wray, Naomi R; Stone, Jennifer L; et al.
Abstract:Schizophrenia is a severe mental disorder with a lifetime risk of about 1%, characterized by hallucinations,delusions and cognitive deficits, with heritability estimated at up to 80%.We performed a genome-wide association study of 3322 European individuals with schizophrenia and 3587 controls.Here we show, using two analytic approaches, the extent to which common genetic variation underlies the risk of schizophrenia.First, we implicate the major histocompatibility complex.Second, we provide molecular genetic evidence for a substantial polygenic component to the risk of schizophrenia involving thousands of common alleles of very small effect.We show that this component also contributes to the risk of bipolar disorder, but not to several non-psychiatric diseases.
来源出版物:Nature, 2009, 460(7256): 748-752
被引频次:1523
Subgenual prefrontal cortex abnormalities in mood disorders
Drevets, WC; Price, JL; Simpson, JR; et al.
Abstract:Pathological disturbances of mood may follow a ‘bipolar’ course, in which normal moods alternate with both depression and mania, or a ‘unipolar’ course, in which only depression occurs.Both bipolar and unipolar disorders can be heritable illnesses associated with neurochemical,neuroendocrine and autonomic abnormalities.The neurobiological basis for these abnormalities has not been established.Using positron emission tomographic (PET)images of cerebral blood flow and rate of glucose metabolism to measure brain activity, we have now localized an area of abnormally decreased activity in the pre-frontal cortex ventral to the germ of the corpus callosum in both familial bipolar depressives and familial unipolar depressives.This decrement in activity was at least partly explained by a corresponding reduction in cortical volume as magnetic resonance imaging (MRI)demonstrated reductions in the mean grey matter volume in the same area of 39% and 48% in the bipolar and unipolar samples, respectively.This region has previously been implicated in the mediation of emotional and autonomic responses to socially significant or provocative stimuli, and in the modulation of the neurotransmitter systems targeted by antidepressant drugs.
来源出版物:Nature, 1997, 386(6627): 824-827
被引频次:1307
The role of childhood trauma in the neurobiology of mood and anxiety disorders: Preclinical and clinical studies
Heim, C; Nemeroff, CB
Abstract:Epidemiologic studies indicate that children exposed to early adverse experiences are at increased risk for the development of depression, anxiety disorders, or both.Persistent sensitization of central nervous system(CNS) circuits as a consequence of early life stress, which are integrally involved in the regulation of stress and emotion, may represent the underlying biological substrate of art increased vulnerability to subsequent stress as well as to the development of depression and anxiety, A number of preclinical studies suggest that early life stress induces long-lived hyper (re) activity of corticotrophin-releasing factor (CRF) systems as well as alterations in other neurotransmitter systems, resulting in increased stress responsiveness.Many of the findings from these preclinical studies are comparable to findings in adult patients with mood and anxiety disorders.Emerging evidence from clinical studies suggests that exposure to early life stress is associated with neurobiological changes in children and adults, which may underlie the increased risk of psychopathology.Current research is focused on strategies to prevent or reverse the detrimental effects of early life stress on the CNS The identification of the neurobiological substrates of early adverse experience is of paramount importance for the development of novel treatments for children, adolescents, and adults.
Keywords:stress; development; animal; human;depression; anxiety
来源出版物:Biological Psychiatry, 2001, 49(12): 1023-1039
被引频次:1201
Cross-national epidemiology of major depression and bipolar disorder
Weissman, MM; Bland, RC; Canino, GJ; et al.
Abstract:Objective: To estimate the rates and patterns of major depression and bipolar disorder based on cross-national epidemiologic surveys.Design and Setting: Population based epidemiologic studies using similar methods from 10 countries: the United States, Canada, Puerto Rico, France,West Germany, Italy, Lebanon, Taiwan, Korea, and New Zealand.Participants: Approximately 38000 community subjects.Outcome Measures: Rates, demographics, and age at onset of major depression and bipolar disorder.Symptom profiles, comorbidity, and marital status with major depression.Results: The lifetime rates for major depression vary widely across countries, ranging from 1.5 cases per 100 adults in the sample in Taiwan to 19.0 cases per 100 adults in Beirut.The annual rates ranged from 0.8 cases per 100 adults in Taiwan to 5.8 cases per 100 adults in New Zealand.The mean age at onset shows less variation (range, 24.8-34.8 years).In every country, the rates of major depression were higher for women than men.By contrast, the lifetime rates of bipolar disorder are more consistent across countries (0.3/100 in Taiwan to 1.5/100 in New Zealand); the sex ratios are nearly equal; and the age at first onset is earlier (average, 6 years) than the onset of major depression.Insomnia and loss of energy occurred in most persons with major depression at each site.Persons with major depression were also at increased risk for comorbidity with substance abuse and anxiety disorders at all sites.Persons who were separated or divorced had significantly higher rates of major depression than married persons in most of the countries, and the risk was somewhat greater for divorced or separated men than women in most countries.Conclusions: There are striking similarities across countries in patterns of major depression and of bipolar disorder.The differences in rates for major depression across countries suggest that cultural differences or different risk factors may affect the expression of the disorder.
Keywords:channel modeling; composite transportation;cuttings and tunnels; high-speed railway (HSR); operation control system; train control data; viaducts
来源出版物:JAMA-Journal of the American Medical Association, 1996, 276(7): 293-299
被引频次:1172
Transduction of psychosocial stress into the neurobiology of recurrent affective disorder
Post, RM
Abstract:Early clinical observations and recent systematic studies overwhelmingly document a greater role for psychosocial stressors in association with the first episode of major affective disorder than with subsequent episodes.The author postulates that both sensitization to stressors and episode sensitization occur and become encoded at the level of gene expression.In particular, stressors and the biochemical concomitants of the episodes themselves can induce the proto-oncogene c-fos and related transcription factors, which then affect the expression of transmitters,receptors, and neuropeptides that alter responsivity in a long-lasting fashion.Thus, both stressors and episodes may leave residual traces and vulnerabilities to further occurrences of affective illness.These data and concepts suggest that the biochemical and anatomical substrates underlying the affective disorders evolve over time as a function of recurrences, as does pharmacological responsivity.This formulation highlights the critical importance of early intervention in the illness in order to prevent malignant transformation to rapid cycling,spontaneous episodes, and refractoriness to drug treatment.
Keywords:high-speed railway; train-bridge system;dynamic interaction; experiment
来源出版物:Computers & Structures, 2005, 83(23-24):1891-1901
被引频次:1141
The long-term natural history of the weekly symptomatic status of bipolar I disorder
Judd, LL; Akiskal, HS; Schettler, PJ; et al.
Abstract:Background: To our knowledge, this is the first prospective natural history study of weekly symptomatic status of patients with bipolar I disorder (BP-I) during long-term follow-up.Methods: Analyses are based on ongoing prospective follow-up of 146 patients with Research Diagnostic Criteria BP-1, who entered the National Institute of Mental Health (Bethesda, Md)Collaborative Depression Study from 1978 through 1981.Weekly affective symptom status ratings were analyzed by polarity and severity, ranging from asymptomatic, to subthreshold levels, to full-blown major depression and mania.Percentages of follow-up weeks at each level as well as number of shifts in symptom status and polarity during the entire follow-up period were examined.Finally,2 new measures of chronicity were evaluated in relation to previously identified predictors of chronicity for BP-I.Results: Patients with BP-I were symptomatically ill 47.3%of weeks throughout a mean of 12.8 years of follow-up.Depressive symptoms (31.9% of total follow-up weeks)predominated over manic/hypomanic symptoms (8.9% of weeks) or cycling/mixed symptoms (5.9% of weeks).Subsyndromal, minor depressive, and hypomanic symptoms combined were nearly 3 times more frequent than syndromal-level major depressive and manic symptoms(29.9% vs 11.2% of weeks, respectively).Patients with BP-I changed symptom status an average of 6 times per year and polarity more than 3 times per year.Longer intake episodes and those with depression-only or cycling polarity predicted greater chronicity during long-term follow-up,as did comorbid drug-use disorder.Conclusions: The longitudinal weekly symptomatic course of BP-I is chronic.Overall, the symptomatic structure is primarily depressive rather than manic, and sub-syndromal and minor affective symptoms predominate.Symptom severity levels fluctuate,often within the same patient over time.Bipolar I disorder is expressed as a dimensional illness featuring the full range (spectrum) of affective symptom severity and polarity.
来源出版物:Archives of General Psychiatry, 2002, 59(6):530-537
被引频次:863
Brain structural and functional abnormalities in mood disorders: Implications for neurocircuitry models of depression
Drevets, Wayne C; Price, Joseph L; Furey, Maura L; et al.
Abstract:The neural networks that putatively modulate aspects of normal emotional behavior have been implicated in the pathophysiology of mood disorders by converging evidence from neuroimaging, neuropathological and lesion analysis studies.These networks involve the medial prefrontal cortex (MPFC) and closely related areas in the medial and caudolateral orbital cortex (medial prefrontal network), amygdala, hippocampus, and ventromedial parts of the basal ganglia, where alterations in grey matter volume and neurophysiological activity are found in cases with recurrent depressive episodes.Such findings hold major implications for models of the neurocircuits that underlie depression.In particular evidence from lesion analysis studies suggests that the MPFC and related limbic and striato-pallido-thalamic structures organize emotional expression.The MPFC is part of a larger “default system”of cortical areas that include the dorsal PFC, mid- and posterior cingulate cortex, anterior temporal cortex, and entorhinal and parahippocampal cortex, which has been implicated in self-referential functions.Dysfunction within and between structures in this circuit may induce disturbances in emotional behavior and other cognitive aspects of depressive syndromes in humans.Further,because the MPFC and related limbic structures provide forebrain modulation over visceral control structures in the hypothalamus and brainstem, their dysfunction can account for the disturbances in autonomic regulation and neuroendocrine responses that are associated with mood disorders.This paper discusses these systems together with the neurochemical systems that impinge on them and form the basis for most pharmacological therapies.
来源出版物:Brain Structure & Function, 2008, 213(1-2):93-118
被引频次:830
Common genetic determinants of schizophrenia and bipolar disorder in Swedish families:A population-based study
Lichtenstein, Paul; Yip, Benjamin H; Bjork, Camilla; et al.
Abstract:Background: whether schizophrenia and bipolar disorder are the clinical outcomes of discrete or shared causative processes is much debated in psychiatry.We aimed to assess genetic and environmental contributions to liability for schizophrenia, bipolar disorder, and their comorbidity.Methods: We linked the multi-generation register, which contains information about all children and their parents in Sweden, and the hospital discharge register,which includes all public psychiatric inpatient admissions in Sweden.We identified 9009202 unique individuals in more than 2 million nuclear families between 1973 and 2004.Risks for schizophrenia, bipolar disorder, and their co-morbidity were assessed for biological and adoptive parents, offspring, full-siblings and half-siblings of pro-bands with one of the diseases.We used a multivariate generalized linear mixed model for analysis of genetic and environmental contributions to liability for schizophrenia,bipolar disorder, and co-morbidity.Findings First-degree relatives of pro-bands with either schizophrenia (n=35985)or bipolar disorder (n=40487) were at increased risk of these disorders.Half-siblings had a significantly increased risk (schizophrenia: relative risk [RR] 3.6, 95%CI2.3-5.5 for maternal half-siblings, and 2.7, 1.9-3.8 for paternal half-siblings; bipolar disorder: 4.5, 2.7-7.4 for maternal half-siblings, and 2.4, 1.4-4.1 for paternal half-siblings),but substantially lower than that of the full-siblings(schizophrenia: 9.0, 8.5-11.6; bipolar disorder: 7.9,7.1-8.8).When relatives of pro-bands with bipolar disorder were analyzed, increased risks for schizophrenia existed for all relationships, including adopted children to biological parents with bipolar disorder.Heritability for schizophrenia and bipolar disorder was 64% and 59%,respectively.Shared environmental effects were small but substantial (schizophrenia: 4.5%, 4.4%-7.4%; bipolar disorder: 3.4%, 2.3%-6.2%) for both disorders.The comorbidity between disorders was mainly (63%) due to additive genetic effects common to both disorders.Interpretation Similar to molecular genetic studies, we showed evidence that schizophrenia and bipolar disorder partly share a common genetic cause.These results challenge the current nosological dichotomy between schizophrenia and bipolar disorder, and are consistent with a reappraisal of these disorders as distinct diagnostic entities.Funding: Swedish Council for Working Life and Social Research, and the Swedish Research Council.
来源出版物:Lancet, 2009, 373(9659): 234-239
·推荐论文摘要·
北京市社区人群心境障碍、焦虑障碍及物质使用障碍的现况调查
刘肇瑞,黄悦勤,陈曦,等
摘要:目的:描述北京市心境障碍、焦虑障碍及物质使用障碍的流行病学特点。方法:按照现况调查多阶段分层抽样的方法于2010年选取北京市3387名16岁及以上社区居民,采用复合性国际诊断交谈表3.0计算机版进行入户访谈,按美国精神病学协会诊断和统计手册第4版的标准对心境障碍、焦虑障碍及物质使用障碍进行诊断。结果:接受访谈者2469人,应答率为72.9%。心境障碍30 d患病率和调整率分别为0.81%和0.87%,12月患病率和调整率分别为3.32%和3.40%,终生患病率和调整率分别为7.21%和6.55%。焦虑障碍30天患病率和调整率分别为3.16%和3.08%,12月患病率和调整率分别为3.93%和3.90%,终生患病率和调整率分别为5.95%和6.37%。物质使用障碍30 d患病率和调整率分别为0.33%和0.37%,12月患病率和调整率分别为1.15%和1.92%,终生患病率和调整率分别为5.30%和5.58%。心境障碍、焦虑障碍以及物质使用障碍间存在共病现象;首发年龄中位数分别为38岁、15岁和28岁。结论:本次调查显示北京市9人中约有1人曾患有心境障碍、焦虑障碍或物质使用障碍中的一种,应大力加强精神卫生知识宣传和防治。
关键词:心境障碍;焦虑障碍;物质使用障碍;患病率;复合性国际诊断交谈表;现况调查
来源出版物:中国心理卫生杂志,2013, 27(2): 102-110
认知疗法提升恶劣心境障碍大学生心理韧性个案研究
王平
摘要:目的:初步探索认知疗法对提升恶劣心境障碍大学生心理韧性的效果。方法:1例恶劣心境障碍大学生接受连续9周、每周一次的认知治疗。采用青少年心理韧性量表、抑郁自评量表、焦虑自评量表和领悟社会支持量表在干预前、干预后和干预后3个月对患者分别实施测评,并收集患者的主观报告。结果:患者经过干预后,心理韧性水平提高,同时抑郁、焦虑水平下降。自我报告治疗后社会支持感提高,生活满意度提高,其效果在干预结束后3个月内的跟踪期间仍保持稳定。结论:认知治疗对有效地提升恶劣心境障碍患者的心理韧性存在一定的可能性,但未来仍需更多的实证研究来证实。
关键词:认知治疗;心理韧性;恶劣心境障碍;大学生;个案
来源出版物:中国临床心理学杂志, 2013, 21(2): 334-338
双相情感障碍:综述
周淑新,李雯(译)
摘要:双相情感障碍为常见、致残、反复发作、严重度不同的精神卫生问题。常发生于儿童晚期或青春早期。双相情感障碍患者患其他精神障碍及躯体疾病的比率较高。双相情感障碍若能早期识别则可改善结果。心境发作治疗取决于呈现的病程阶段:躁狂、轻躁狂、混合状态、抑郁或维持阶段。双相情感障碍常在出现症状数年后的青春期或成人早期才被诊断出来。症状包括躁狂、轻躁狂、精神病症状或相对健康期夹杂抑郁。双相情感障碍的临床病程呈多变性。单相发作的患者罕见,据报道其5年复发率>70%。虽然双相情感障碍用出现躁狂或轻躁狂症状来定义,但多数患者多数时间都处于抑郁状态,这也是致残的主要原因。
关键词:双相情感障碍;诊断;治疗
来源出版物:中国全科医学, 2013, 16(2B): 473-477
抑郁症的多机制发病
刘春林,阮克锋,高君伟,等
摘要:抑郁症(depression)是一种严重的精神疾病,对社会危害极大。最新研究表明抑郁症病因复杂,涉及神经系统和内分泌系统的多种神经递质与激素,以及相应的受体。本文对近几年抑郁症发病机制的研究进行了综述。
关键词:抑郁症;机制;抗抑郁
来源出版物:生理科学进展, 2014, 44(4): 253-258
双相障碍的诊治与研究——机遇与挑战
方贻儒,吴志国,陈俊
摘要:双相障碍临床表现复杂、病程多变,常导致临床识别不足、诊断不确定以及治疗困难。由此,学界开展了一系列研究,探索该病的特征与本质,并在循证医学的基础上践行有关诊断标准的修正以及治疗理念的纠正。该文从概念与诊断、神经生物学研究进展以及心境稳定剂治疗等方面对双相障碍的探索现状和前景进行评述。
关键词:双相障碍;诊断;精神疾病诊断与统计手册;神经生物学;心境稳定剂
来源出版物:上海交通大学学报(医学版), 2014, 34(4):413-416
长沙地区社区人群酒精使用障碍与心境障碍共病调查
谭奔腾,杨梅,郭田生,等
摘要:目的:了解长沙地区居民酒精使用障碍与心境障碍共病的患病情况。方法:采用多阶段整群抽样方法,对15岁及以上人群进行入户调查,共抽样12475人。以增补后的一般健康问卷12(GHQ-12)为筛选工具,将调查对象分为患精神疾病高、中、低危险组。以美国精神障碍诊断与统计手册第4版(DSM-IV)轴Ⅰ障碍定式临床检查病人版(SCID-I/P)为诊断工具。12094人完成GHQ-12,2351人完成SCID-I/P,对这2351名居民中酒精使用障碍和心境障碍的共患情况进行分析。结果:酒精使用障碍和心境障碍的时点患病率分别为1.76%(46/2351)和6.01%(141/2351)。酒精使用障碍患者有心境障碍者占60.9%(28/46),心境障碍患者有酒精使用障碍者为19.9%(28/141)。控制年龄、性别、居住地、受教育程度、家庭年收入以后,酒精使用障碍患者发生心境障碍的风险性高于非现患酒精使用障碍者(OR=33.54, 95%CI: 17.52~64.20);心境障碍患者发生酒精使用障碍的风险性高于非现患心境障碍者(OR=35.11,95%CI: 18.02~68.39)。结论:酒精使用障碍与心境障碍容易发生共患,应引起精神卫生工作者的重视。
关键词:酒精使用障碍;心境障碍;患病率;共病;现况调查
来源出版物:中国心理卫生杂志, 2014, 28(5): 349-355
从“焦虑性抑郁症”概念解析抑郁障碍的复杂性
吴志国,吴彦,方贻儒
摘要:抑郁障碍是一类极为复杂的精神疾病,目前已发展出诸多临床描述亚型以试图“精准对焦”解析抑郁障碍的复杂化现象,其中焦虑性抑郁症受到了越来越多的关注。该文将通过对以症状维度定义的焦虑性抑郁症研究进展进行综述,从共患焦虑的角度对抑郁障碍的复杂性进行解析。
关键词:抑郁障碍;焦虑性抑郁症;焦虑障碍;共病
来源出版物:上海交通大学学报:医学版, 2014, 34(4):450-454
抗炎性细胞因子与抑郁症
徐说,林文娟
摘要:细胞因子假说是关于抑郁症发病机理的重要假说,为探讨抑郁症的发病机理和临床治疗方法提供了新方向。细胞因子分为前炎性细胞因子和抗炎性细胞因子。前炎性细胞因子与抑郁症的发病密切相关,而抗炎性细胞因子可能具有抗抑郁的作用。本文着重综述抗炎性细胞因子与抑郁症的关系。抗炎性细胞因子如白介素10、白介素1受体拮抗剂、白介素4、白介素13、转化生长因子β和脂联素等,在抑郁症中表达下降;补充外源抗炎性细胞因子则具有一定的抗抑郁作用。抗炎性细胞因子可通过拮抗前炎性细胞因子的作用,并与MAPK信号通路、神经递质和糖皮质激素相互作用而参与到抑郁症中.抗抑郁药能使抗炎性细胞因子的表达上升,这可能是药物起效的机制之一。抗炎策略在抑郁症的治疗中有重要应用前景。
关键词:抑郁症;细胞因子;抗炎性细胞因子;抗炎作用;抗抑郁药
来源出版物:生物化学与生物物理进展, 2014, 41(11):1099-1108
抑郁症发病机制研究进展
王睿,黄树明
摘要:抑郁症因其病因不清、致病因素复杂、发病机制不详,一直是神经科学领域的一个难题。近年来,国内外对抑郁症的研究方兴未艾,并在发病机制的研究上取得了重要进展。文中从神经生化研究、神经内分泌研究、神经可塑性研究等方面对抑郁症的发生机制主流假说进行简单阐述,以拓宽对抑郁症的认识。
关键词:抑郁症;神经生化;神经内分泌;神经可塑性
来源出版物:医学研究生学报, 2014, 27(12): 1332-1336
误诊为抑郁症的双相障碍Ⅱ型患者自杀风险的危险因素分析
王君,陈林,吉振鹏,等
摘要:目的:探讨误诊为抑郁症的双相障碍Ⅱ型患者自杀风险的社会人口学及临床特征方面的危险因素。方法:通过简明国际神经精神访谈(the Mini International Neuropsychiatric Interview, MINI)5.0中文版,对来自全国13个中心的1478例最初诊断为抑郁症的患者进行重新诊断,其中190例被诊断为双相障碍Ⅱ型,将这190例误诊患者按照有无自杀风险进行分组,从性别、年龄等社会人口学资料及起病年龄、是否伴有自杀观念等临床特征方面探讨被误诊患者自杀风险可能的危险因素。结果:有自杀风险组共74例患者,无自杀风险组共116例。有自杀风险组与无自杀风险组相比,年龄更小[(34.45±11.18)vs.(37.23±13.22)],起病年龄更早[(26.20±9.16)vs.(30.37±11.59)],更常伴有自杀观念(82.4% vs.53.4%),差异均具有统计学意义(P<0.05)。Logistic回归分析显示,年龄(OR=0.969, 95%CI: 0.945~0.993)、伴有自杀观念(OR=4.129, 95%CI:2.030~8.397)与误诊为抑郁症的双相障碍Ⅱ型患者发生自杀风险相关联(P<0.05)。结论:年龄小、伴有自杀观念可能是误诊为抑郁症的双相障碍Ⅱ型患者自杀风险的独立危险因素。
关键词:双相障碍;抑郁症;自杀风险;危险因素;误诊
来源出版物:中国神经精神疾病杂志, 2015, 41(2): 65-70
情感障碍患者的疾病感知
张萌,赵旭东
摘要:疾病感知是指患者利用以往获取的疾病知识经验来分析解释当前的症状或疾病的过程。本文对疾病感知的概念、测量工具、干预措施及其在情感障碍患者中的实证研究进行综述,以探讨疾病感知与预后及求治行为、治疗依从性等预后影响因素之间的关系。
关键词:情感障碍;疾病感知;预后;求治行为;治疗依从性
来源出版物:中国临床心理学杂志, 2015, 23(1): 104-107
心境障碍和甲状腺功能异常相关的研究进展
黄立芳,尹超群
摘要:心境障碍是常见的精神障碍疾患,主要表现为心境和情感的改变,通常表现为持久的情感高涨或低落,其高致残率对社会造成了极为严重的危害。甲状腺激素异常见于心境障碍患者,并且甲状腺功能异常加大了人群心境障碍的患病率。心境障碍患者甲状腺功能障碍主要表现为甲状腺激素水平的异常,甲状腺素(T4)向三碘甲状腺原氨酸(T3)转化异常,下丘脑-垂体-甲状腺(HTP)轴功能的亢进或抑制。甲状腺激素对于心境障碍患神经递质有所影响,异常的甲状腺激素水平对基因的调节和生化改变相关联。甲状腺抗体同样是心境障碍发病的关联因素。本文总结了心境障碍和甲状腺功能异常相关的研究进展,为进一步研究心境障碍和甲状腺功能异常提供一定的依据。
关键词:心境障碍;甲状腺功能;甲状腺激素
来源出版物:中国全科医学, 2016, 19(10): 1225-1228
首发精神分裂症与双相障碍及抑郁障碍认知功能比较
陈大春,陈科,张荣珍
摘要:目的:探讨首发精神分裂症、双相障碍及抑郁障碍患者认知功能差异。方法:纳入首发精神分裂症患者61例,双相障碍患者57例,抑郁障碍患者48例,另设正常对照59名。所有研究对象采用重复性神经心理测查系统(repeatable battery for the assessment of neuropsychological status,RBANS)评估认知功能,首发精神分裂症组采用阳性和阴性症状量表(positive and negative syndrome scale,PANSS)评定精神病性症状,双相障碍组、抑郁障碍组采用汉密尔顿抑郁量表(Hamilton depression scale,HAMD)、汉密尔顿焦虑量表(Hamilton anxiety scale,HAMA)评估抑郁和焦虑症状,贝克-拉范森躁狂(Bech-Rafaelsen mania scale,BRMS)量表评估躁狂症状。结果:4组对象的RBANS总分(F=5.18,P<0.01)、即刻记忆(F=4.09,P<0.01)、言语功能(F=9.53,P<0.01)、注意(F=3.87,P=0.01)、延时记忆(F=9.86,P<0.01)因子得分差异具有统计学意义,其中首发精神分裂症、双相障碍组RBANS总分低于对照组(P<0.01),首发精神分裂症、双相障碍、抑郁障碍组即刻记忆、言语功能、延时记忆得分低于对照组(P<0.05),双相障碍组言语功能得分低于首发精神分裂症组(P<0.01),首发精神分裂症组注意得分低于抑郁障碍及对照组(P<0.01)。结论:首发精神分裂症、双相障碍、抑郁障碍患者均存在认知功能损伤,首发精神分裂症认知功能缺陷重于抑郁障碍,轻于双相障碍。
关键词:首发精神分裂症;双相障碍;抑郁障碍;认知功能
来源出版物:中国神经精神疾病杂志, 2016, 42(9): 518-522
情绪障碍及其干预:心理表象的视角
王铭,江光荣
摘要:心理表象在多种情绪障碍中均表现出病理性特点。研究者基于心理表象主要对创伤后应激障碍、抑郁心境、双相障碍情绪和社交焦虑进行了心理病理学解释,尤其关注闪回和过度概化记忆等两种典型症状,并且重视心理表象在情绪症状维持中的作用。概括而言,研究者强调记忆形成与提取过程的异常、认知与行为的保护性策略的负强化、对事件及自我的认知偏差等三类因素对情绪障碍的致病作用。目前,针对或运用心理表象的干预与训练方法包括减少消极表象、改变消极表象内容、提高积极表象能力、提高记忆的具体性等四类。未来应注重侵入性表象的功能分析以及相关的心理病理学模型研究,并拓展干预与训练研究。
关键词:心理表象;情绪障碍;心理病理学;干预与训练
来源出版物:心理科学进展, 2016, 24(4): 573-590
双相抑郁的特点、危害及药物治疗研究进展
袁铭,李素敏,王雪芹,等
摘要:双相抑郁是一复发性疾病,不同情感形式的发作可能会对患者的心理、职业和社会福利产生持续的破坏作用。此外,双相抑郁是一种严重的致残性疾病,因与单相抑郁不易区分,极易被误诊,对患者及社会造成严重的负担。抑郁症状是双相抑郁的主要特征,该阶段患者的自杀率较高,应得到重视。本文将双相抑郁的特点、危害及药物治疗研究进展进行综述,为进一步研究双相抑郁的治疗提供一定的依据。
关键词:双相情感障碍;危害;治疗进展
来源出版物:中国全科医学, 2016, 19(10): 1229-1233
双相障碍患者对情绪信息的注意偏向
程玉琴,刘铁榜
摘要:有关注意的研究为双相障碍的病理性研究和治疗研究提供了发展框架。已有研究表明对消极情绪的注意偏向可能是罹患双相障碍的危险因素。本文从双相障碍患者对情绪注意偏向是状态性还是素质性、心境是否一致性,以及不同临床相患者的注意偏向特征等方面进行了探讨,并提出了对患者注意偏向干预的行为学矫治方法。
关键词:双相障碍;注意偏向;情绪;综述
来源出版物:中国心理卫生杂志, 2017, 31(7): 528-532
重性抑郁障碍病人生活质量及其影响因素
李峰,薄奇静,赵燕,等
摘要:目的:评估重性抑郁障碍(major depressive disorder, MDD)病人的生活质量,分析其影响因素。方法:对符合美国精神障碍诊断与统计手册第4版(Diagnostic and Statistical Manual of Mental Disorders 4th edition, DSM-IV)诊断的92例成人重性抑郁障碍病人及80例健康对照使用世界卫生组织生存质量测定量表简表(World Health Organization Quality of Life Scale Brief, WHOQOL-BREF)、汉密尔顿抑郁量表17项(the 17-item Hamilton Depression Rating Scale, HAMD-17)、汉密尔顿焦虑量表(Hamilton Anxiety Scale, HAMA)、社会支持量表(Social Support Rating Scale, SSRS)进行评估。结果重性抑郁障碍病人的WHOQOL-BREF各维度评分均低于健康对照(P<0.05);对病人组进行Pearson相关分析显示,WHOQOL-BREF各维度评分与HAMD-17、HAMA评分呈负相关,与SSRS评分呈正相关(P<0.01)。性别与WHOQOL-BREF的社会关系领域呈负相关(P<0.05),而病程与WHOQOL-BREF的环境领域呈负相关(P<0.05)。对病人组进行逐步多元线性回归分析显示,HAMD-17评分与WHOQOL-BREF的生理、心理领域得分呈负相关(P<0.05);SSRS的主观支持评分与WHOQOL-BREF的心理、社会关系、环境领域呈正相关(P<0.05);SSRS中对支持的利用度、家庭收入等级与WHOQOL-BREF的心理领域也有影响(P<0.01)。结论重性抑郁障碍病人的生活质量低于一般人群,并且症状越重、病程越长及社会支持度越差,生活质量越差。而男性病人可能具有更差的生活质量。具有稳定的配偶也有助于提升生活质量。
关键词:重性抑郁障碍;生活质量;世界卫生组织生存质量测定量表简表
来源出版物:首都医科大学学报, 2017, 38(2): 1860191
双相心境障碍抑郁发作患病严重程度的影响因素分析
庚天琦,安妮,王喜今,等
摘要:目的:研究影响双相心境障碍疾病抑郁发作期严重程度的危险因素,为该病的有效预防提供理论依据。方法:收集2010—2015年某市精神专科医院的双相心境障碍抑郁发作住院466名患者的病例信息,根据汉密尔顿抑郁量表将患者分为轻、中、重度,并选出年龄、性别、居住地、出生季节、遗传史等15个可能危险因素,进行单因素和多因素条件Logistic回归分析。结果:Logistic回归分析筛选出7个影响双相心境障碍疾病抑郁发作严重程度的危险因素,即出生季节(冬季OR=3.091、秋季OR=2.363)、高学历(OR=1.414)、婚姻离异(OR=3.132)、长期居住农村(OR=0.587)、排行老大(OR=1.461)、性格内向(OR=1.705)、家族遗传史(OR=2.101)。结论:双相心境障碍抑郁发作严重程度受多种因素的影响。
关键词:双相心境障碍;病例回顾分析;危险因素;Logistic回归
来源出版物:现代预防医学, 2017, 44(6): 1145-1148
From stress to inflammation and major depressive disorder: A social signal transduction theory of depression
Slavich, George M; Irwin, Michael R
Abstract:Major life stressors, especially those involving interpersonal stress and social rejection, are among the strongest proximal risk factors for depression.In this review, we propose a biologically plausible, multilevel theory that describes neural, physiologic, molecular, and genomic mechanisms that link experiences of socialenvironmental stress with internal biological processes that drive depression pathogenesis.Central to this social signal transduction theory of depression is the hypothesis that experiences of social threat and adversity up-regulate components of the immune system involved in inflammation.The key mediators of this response, called proinflammatory cytokines, can in turn elicit profound changes in behavior, which include the initiation of depressive symptoms such as sad mood, anhedonia,fatigue, psychomotor retardation, and social-behavioral withdrawal.This highly conserved biological response to adversity is critical for survival during times of actual physical threat or injury.However, this response can also be activated by modern-day social, symbolic, or imagined threats, leading to an increasingly proinflammatory phenotype that may be a key phenomenon driving depression pathogenesis and recurrence, as well as the overlap of depression with several somatic conditions including asthma, rheumatoid arthritis, chronic pain,metabolic syndrome, cardiovascular disease, obesity, and neurodegeneration.Insights from this theory may thus shed light on several important questions including how depression develops, why it frequently recurs, why it is strongly predicted by early life stress, and why it often co-occurs with symptoms of anxiety and with certain physical disease conditions.This work may also suggest new opportunities for preventing and treating depression by targeting inflammation.
Keywords:early life stress; social threat; cytokines;mechanisms; disease
来源出版物:Psychological Bulletin, 2014, 140(3): 774-815
Inflamed moods: A review of the interactions between inflammation and mood disorders
Rosenblat, Joshua D; Cha, Danielle S;Mansur, Rodrigo B; et al.
Abstract:Mood disorders have been recognized by the World Health Organization (WHO) as the leading cause of disability worldwide.Notwithstanding the established efficacy of conventional mood agents, many treated individuals continue to remain treatment refractory and/or exhibit clinically significant residual symptoms, cognitive dysfunction, and psychosocial impairment.Therefore, a priority research and clinical agenda is to identify pathophysiological mechanisms subserving mood disorders to improve therapeutic efficacy.During the past decade,inflammation has been revisited as an important etiologic factor of mood disorders.Therefore, the purpose of this synthetic review is threefold: 1) to review the evidence for an association between inflammation and mood disorders,2) to discuss potential pathophysiologic mechanisms that may explain this association and 3) to present novel therapeutic options currently being investigated that target the inflammatory-mood pathway.Accumulating evidence implicates inflammation as a critical mediator in the pathophysiology of mood disorders.Indeed, elevated levels of pro-inflammatory cytokines have been repeatedly demonstrated in both major depressive disorder (MDD)and bipolar disorder (BD) patients.Further, the induction of a pro-inflammatory state in healthy or medically ill subjects induces ‘sickness behavior’ resembling depressive symptomatology.Potential mechanisms involved include,but are not limited to, direct effects of pro-inflammatory cytokines on monoamine levels, dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, pathologic microglial cell activation, impaired neuroplasticity and structural and functional brain changes.Anti-inflammatory agents, such as acetyl-salicylic acid (ASA), celecoxib, anti-TNF-alpha agents, minocycline, curcumin and omega-3 fatty acids, are being investigated for use in mood disorders.Current evidence shows improved outcomes in mood disorder patients when anti-inflammatory agents are used as an adjunct to conventional therapy; however,further research is needed to establish the therapeutic benefit and appropriate dosage.
Keywords:bipolar disorder; cytokines; inflammation;major depressive disorder; mood disorder; non-steroidal anti-inflammatory drug (NSAID)
来源出版物:Progress in Neuro-Psychopharmacology &Biological Psychiatry, 2014, 53: 23-34
A critical appraisal of neuroimaging studies of bipolar disorder: Toward a new conceptualization of underlying neural circuitry and a road map for future research
Phillips, Mary L; Swartz, Holly A
Abstract:Objective: In this critical review, the authors appraise neuroimaging findings in bipolar disorder in emotion-processing, emotion-regulation, and rewardprocessing neural circuitry in order to synthesize the current knowledge of the neural underpinnings of bipolar disorder and provide a neuroimaging research road map for future studies.Method: The authors examined findings from all major studies in bipolar disorder that used functional MRI, volumetric analysis, diffusion imaging,and resting-state techniques, integrating findings to provide a better understanding of larger-scale neural circuitry abnormalities in bipolar disorder.Results: Bipolar disorder can be conceptualized, in neural circuitry terms, as parallel dysfunction in prefrontal cortical (especially ventrolateral prefrontal cortical) hippocampal-amygdala emotionprocessing and emotion-regulation circuits bilaterally,together with an “overactive” left-sided ventral.striatalventrolateral and orbitofrontal cortical reward-processing circuitry, resulting in characteristic behavioral abnormalities associated with bipolar disorder: emotional lability,emotional dysregulation, and heightened reward sensitivity.A potential structural basis for these functional abnormalities is gray matter volume decreases in the prefrontal and temporal cortices, the amygdala, and the hippocampus and fractional anisotropy decreases in white matter tracts connecting prefrontal and subcortical regions.Conclusions:Neuroimaging studies of bipolar disorder clearly demonstrate abnormalities in neural circuits supporting emotion processing, emotion regulation, and reward processing, although there are several limitations to these studies.Future neuroimaging research in bipolar disorder should include studies adopting dimensional approaches;larger studies examining neurodevelopmental trajectories in youths with bipolar disorder or at risk for bipolar disorder; multimodal neuroimaging studies using integrated systems approaches; and studies using pattern recognition approaches to provide clinically useful individual-level data.Such studies will help identify clinically relevant biomarkers to guide diagnosis and treatment decision making for individuals with bipolar disorder.
来源出版物:American Journal of Psychiatry, 2014, 171(8):829-843
Reward processing dysfunction in major depression,bipolar disorder and schizophrenia
Whitton, Alexis E; Treadway, Michael T;Pizzagalli, Diego A; et al.
Abstract:Purpose of reviewThis article reviews the recent literature on reward processing dysfunction in major depression (MDD), bipolar disorder and schizophrenia,with a focus on approach motivation, reward learning and reward-based decision-making.Recent findingsEmerging evidence indicates the presence of reward processing abnormalities across all three disorders, supporting a transdiagnostic approach.In particular, findings are consistent with a role of abnormal phasic striatal dopamine signaling, which is critical for reinforcement learning,efficient mobilization of effort to obtain reward and allocation of attention to reward-predictive cues.Specifically,reward-related striatal signaling appears blunted in MDD and the negative symptoms of schizophrenia, elevated in bipolar (hypo) mania, and contextually misallocated in the positive symptoms of psychosis.However, whether shared or distinct pathophysiological mechanisms contribute to abnormal striatal signaling across the three disorders remains unknown.Summary: New evidence of reward processing abnormalities in MDD, bipolar disorder and schizophrenia has led to a greater understanding of the neural processes associated with symptomatology common across these conditions (e.g., anhedonia).Dissecting various subcomponents of reward processing that map onto partially different neurobiological pathways and investigating their dysregulation in different psychiatric disorders holds promise for developing more targeted, and hopefully efficacious treatment and intervention strategies.
Keywords:bipolar disorder; dopamine; major depressive disorder; reward learning; schizophrenia
来源出版物:Current Opinion in Psychiatry, 2015, 28(1):7-12
Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: A systematic review and meta-analysis
Vancampfort, Davy; Stubbs, Brendon;Mitchell, Alex J; et al.
Abstract:Metabolic syndrome (MetS) and its components are highly predictive of cardiovascular diseases.The primary aim of this systematic review and meta-analysis was to assess the prevalence of MetS and its components in people with schizophrenia and related psychotic disorders,bipolar disorder and major depressive disorder, comparing subjects with different disorders and taking into account demographic variables and psychotropic medication use.The secondary aim was to compare the MetS prevalence in persons with any of the selected disorders versus matched general population controls.The pooled MetS prevalence in people with severe mental illness was 32.6% (95%CI:30.8%-34.4%;N=198;n=52678).Relative risk metaanalyses established that there was no significant difference in MetS prevalence in studies directly comparing schizophrenia versus bipolar disorder, and in those directly comparing bipolar disorder versus major depressive disorder.Only two studies directly compared people with schizophrenia and major depressive disorder,precluding meta-analytic calculations.Older age and a higher body mass index were significant moderators in the final demographic regression model (z=-3.6,P=0.0003,r2=0.19).People treated with all individual antipsychotic medications had a significantly (P<0.001) higher MetS risk compared to antipsychotic-naive participants.MetS risk was significantly higher with clozapine and olanzapine(except vs.clozapine) than other antipsychotics, and significantly lower with aripiprazole than other antipsychotics (except vs.amisulpride).Compared with matched general population controls, people with severe mental illness had a significantly increased risk for MetS(RR=1.58; 95%CI: 1.35-1.86;P<0.001) and all its components, except for hypertension (P=0.07).These data suggest that the risk for MetS is similarly elevated in the diagnostic subgroups of severe mental illness.Routine screening and multidisciplinary management of medical and behavioral conditions is needed in these patients.Risks of individual antipsychotics should be considered when making treatment choices.
Keywords:Metabolic syndrome; severe mental illness;schizophrenia; bipolar disorder; major depressive disorder;antipsychotics
来源出版物:World Psychiatry, 2015, 14(3): 339-347
Differential responses to lithium in hyperexcitable neurons from patients with bipolar disorder
Mertens, Jerome; Wang, Qiuwen; Kim, Yongsung; et al.
Abstract:Bipolar disorder is a complex neuropsychiatric disorder that is characterized by intermittent episodes of mania and depression; without treatment, 15% of patients commit suicide.Hence, it has been ranked by the World Health Organization as a top disorder of morbidity and lost productivity.Previous neuropathological studies have revealed a series of alterations in the brains of patients with bipolar disorder or animal models’, such as reduced glial cell number in the prefrontal cortex of patients,upregulated activities of the protein kinase A and C pathways and changes in neurotransmission.However,the roles and causation of these changes in bipolar disorder have been too complex to exactly determine the pathology of the disease.Furthermore, although some patients show remarkable improvement with lithium treatment for yet unknown reasons, others are refractory to lithium treatment.Therefore, developing an accurate and powerful biological model for bipolar disorder has been a challenge.The introduction of induced pluripotent stem-cell (iPSC) technology has provided a new approach.Here we have developed an iPSC model for human bipolar disorder and investigated the cellular phenotypes of hippocampal dentate gyrus-like neurons derived from iPSCs of patients with bipolar disorder.Guided by RNA sequencing expression profiling, we have detected mitochondrial abnormalities in young neurons from patients with bipolar disorder by using mitochondrial assays; in addition, using both patch-clamp recording and somatic Ca2+imaging, we have observed hyperactive action-potential firing.This hyperexcitability phenotype of young neurons in bipolar disorder was selectively reversed by lithium treatment only in neurons derived from patients who also responded to lithium treatment.Therefore,hyperexcitability is one early endophenotype of bipolar disorder, and our model of iPSCs in this disease might be useful in developing new therapies and drugs aimed at its clinical treatment.
来源出版物:Nature, 2015, 527(7576): 95-99
Bipolar disorder
Grande, Iria; Berk, Michael; Birmaher, Boris
Abstract:Bipolar disorder is a recurrent chronic disorder characterised by fluctuations in mood state and energy.It affects more than 1% of the world's population irrespective of nationality, ethnic origin, or socioeconomic status.Bipolar disorder is one of the main causes of disability among young people, leading to cognitive and functional impairment and raised mortality, particularly death by suicide.A high prevalence of psychiatric and medical comorbidities is typical in affected individuals.Accurate diagnosis of bipolar disorder is difficult in clinical practice because onset is most commonly a depressive episode and looks similar to unipolar depression.Moreover, there are currently no valid biomarkers for the disorder.Therefore,the role of clinical assessment remains key.Detection of hypomanic periods and longitudinal assessment are crucial to differentiate bipolar disorder from other conditions.Current knowledge of the evolving pharmacological and psychological strategies in bipolar disorder is of utmost importance.
来源出版物:Lancet, 2016, 387(10027): 1561-1572
The genetics of stress-related disorders: PTSD,depression, and anxiety disorders
Smoller, Jordan W
Abstract:Research into the causes of psychopathology has largely focused on two broad etiologic factors: genetic vulnerability and environmental stressors.An important role for familial/heritable factors in the etiology of a broad range of psychiatric disorders was established well before the modern era of genomic research.This review focuses on the genetic basis of three disorder categories-posttraumatic stress disorder (PTSD), major depressive disorder (MDD),and the anxiety disorders-for which environmental stressors and stress responses are understood to be central to pathogenesis.Each of these disorders aggregates in families and is moderately heritable.More recently,molecular genetics approaches, including genome-wide studies of genetic variation, have been applied to identify specific risk variants.In this review, I summarize evidence for genetic contributions to PTSD, MDD, and the anxiety disorders including genetic epidemiology, the role of common genetic variation, the role of rare and structural variation, and the role of gene-environment interaction.Available data suggest that stress-related disorders are highly complex and polygenic and, despite substantial progress in other areas of psychiatric genetics, few risk loci have been identified for these disorders.Progress in this area will likely require analysis of much larger sample sizes than have been reported to date.The phenotypic complexity and genetic overlap among these disorders present further challenges.The review concludes with a discussion of prospects for clinical translation of genetic findings and future directions for research.
来源出版物:Neuropsychopharmacology, 2016, 41(1):297-319
Subcortical volumetric abnormalities in bipolar disorder
Hibar, DP; Westlye, LT; van Erp, TGM; et al.
Abstract:Considerable uncertainty exists about the defining brain changes associated with bipolar disorder(BD).Understanding and quantifying the sources of uncertainty can help generate novel clinical hypotheses about etiology and assist in the development of biomarkers for indexing disease progression and prognosis.Here we were interested in quantifying case-control differences in intracranial volume (ICV) and each of eight subcortical brain measures: nucleus accumbens, amygdala, caudate,hippocampus, globus pallidus, putamen, thalamus, lateral ventricles.In a large study of 1710 BD patients and 2594 healthy controls, we found consistent volumetric reductions in BD patients for mean hippocampus (Cohe’sd=-0.232;P=3.50×10-7) and thalamus (d=-0.148;P=4.27×10-3) and enlarged lateral ventricles (d=-0.260;P=3.93×10-5) in patients.No significant effect of age at illness onset was detected.Stratifying patients based on clinical subtype (BD type I or type II) revealed that BDI patients had significantly larger lateral ventricles and smaller hippocampus and amygdala than controls.However, when comparing BDI and BDII patients directly, we did not detect any significant differences in brain volume.This likely represents similar etiology between BD subtype classifications.Exploratory analyses revealed significantly larger thalamic volumes in patients taking lithium compared with patients not taking lithium.We detected no significant differences between BDII patients and controls in the largest such comparison to date.Findings in this study should be interpreted with caution and with careful consideration of the limitations inherent to meta-analyzed neuroimaging comparisons.
来源出版物:Molecular Psychiatry, 2016, 21(12):1710-1716
What are ‘good’ depression symptoms? Comparing the centrality of DSM and non-DSM symptoms of depression in a network analysis
Fried, Eiko I; Epskamp, Sacha; Nesse, Randolph M; et al.
Abstract:Background: The symptoms for Major Depression (MD) defined in the DSM-5 differ markedly from symptoms assessed in common rating scales, and the empirical question about core depression symptoms is unresolved.Here we conceptualize depression as a complex dynamic system of interacting symptoms to examine what symptoms are most central to driving depressive processes.Methods: We constructed a network of 28 depression symptoms assessed via the Inventory of Depressive Symptomatology (IDS-30) in 3463 depressed outpatients from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study.We estimated the centrality of all IDS-30 symptoms, and compared the centrality of DSM and non-DSM symptoms; centrality reflects the connectedness of each symptom with all other symptom.Results: A network with 28 interwined symptom emerged, and symptoms differed substantially in their centrality values.Both DSM symptoms (e.g., sad mood)and non-DSM symptom (e.g., anxiety) were among the most central symptoms, and DSM criteria were no mow central than non-DSM symptoms.Limitations: Many subjects enrolled in STAR*D reported comorbid medical and psychiatric conditions which may have affected symptom presentation.Conclusion: The network perspective neither supports the standard psychometric notion that depression symptoms are equivalent indicators of MD, nor the common assumption that DSM symptoms of depression are of higher clinical relevance than non-DSM depression symptoms.The findings suggest the value of research focusing On especially central symptoms to increase the accuracy of predicting outcomes such as the course of illness, probability of relapse, and treatment response.
Keywords:centrality; depression symptoms; major depression; network analysis
来源出版物:Journal of Affective Disorders, 2016,189:314-320
Resting-state connectivity biomarkers define neurophysiological subtypes of depression
Drysdale, Andrew T; Grosenick, Logan; Downar, Jonathan;et al.
Abstract:Biomarkers have transformed modern medicine but remain largely elusive in psychiatry, partly because there is a weak correspondence between diagnostic labels and their neurobiological substrates.Like other neuropsychiatric disorders, depression is not a unitary disease, but rather a heterogeneous syndrome that encompasses varied, co-occurring symptoms and divergent responses to treatment.By using functional magnetic resonance imaging (fMRI) in a large multisite sample (n=1188), we show here that patients with depression can be subdivided into four neurophysiological subtypes(‘biotypes’) defined by distinct patterns of dysfunctional connectivity in limbic and frontostriatal networks.Clustering patients on this basis enabled the development of diagnostic classifiers (biomarkers) with high (82%-93%)sensitivity and specificity for depression subtypes in multisite validation (n=711) and out-of-sample replication(n=477) data sets.These biotypes cannot be differentiated solely on the basis of clinical features, but they are associated with differing clinical-symptom profiles.They also predict responsiveness to transcranial magnetic stimulation therapy (n=154).Our results define novel subtypes of depression that transcend current diagnostic boundaries and may be useful for identifying the individuals who are most likely to benefit from targeted neurostimulation therapies.
来源出版物:Nature Medicine, 2017, 23(1): 28-38
Prevalence of depression in patients with mild cognitive impairment a systematic review and Meta-analysis
Ismail, Zahinoor; Elbayoumi, Heba; Fischer, Corinne E
Abstract:Depression is common in individuals with mild cognitive impairment (MCI) and may confer a higher likelihood of progression to dementia.Prevalence estimates of depression in those with MCI are required to guide both clinical decisions and public health policy, but published results are variable and lack precision.Depression is common in individuals with mild cognitive impairment(MCI) and may confer a higher likelihood of progression to dementia.Prevalence estimates of depression in those with MCI are required to guide both clinical decisions and public health policy, but published results are variable and lack precision.A search of literature from database inception to March 2016 was performed using Medline,Embase, and PsycINFO.Hand searching of all included articles was performed, including a Google Scholar search of citations of included articles.Articles were included if they (1) were published in English, (2) reported patients with MCI as a primary study group, (3) reported depression or depressive symptoms using a validated instrument, and(4) reported the prevalence of depression in patients with MCI.All abstracts, full-text articles, and other sourceswere reviewed, with data extracted in duplicate.The overall prevalence of depression in patients with MCI was pooled using a random-effects model.Heterogeneity was explored using stratification and random-effects meta-regression.The prevalence of depression in patients with MCI,reported as a percentage with 95% CIs.Estimates were also stratified by population source (community-based or clinicbased sample), method of depression diagnosis (clinicianadministered, informant-based, or self-report), and method of MCI diagnosis (cognitive vs global measure and amnestic vs nonamnestic).Of 5687 unique abstracts, 255 were selected for full-text review, and 57 studies, representing 20 892 patients, met all inclusion criteria.The overall pooled prevalence of depression in patients with MCI was 32%(95%CI, 27-37), with significant heterogeneity between estimates (I-2=90.7%).When stratified by source, the prevalence of depression in patients with MCI in community-based samples was 25%(95%CI, 19-30) and was 40% (95%CI, 32-48) in clinic-based samples, which was significantly different (P<0.01).The method used to diagnose depression did not significantly influence the prevalence estimate, nor did the criteria used for MCI diagnosis or MCI subtype.The prevalence of depression in patients with MCI is high.A contributor to heterogeneity in the reported literature is the source of the sample, with greater depression burden prevalent in clinic-based samples.
来源出版物:Nonlinear Dynamics, 2016, 83(4): 2157-2169
Resting-state connectivity biomarkers define neurophysiological subtypes of depressionDrysdale, Andrew T; Grosenick, Logan;
Downar, Jonathan; et al.
Abstract:Biomarkers have transformed modern medicine but remain largely elusive in psychiatry, partly because there is a weak correspondence between diagnostic labels and their neurobiological substrates.Like other neuropsychiatric disorders, depression is not a unitary disease, but rather a heterogeneous syndrome that encompasses varied,co-occurring symptoms and divergent responses to treatment.By using functional magnetic resonance imaging(fMRI) in a large multisite sample (n= 1188), we show here that patients with depression can be subdivided into four neurophysiological subtypes (‘biotypes’) defined by distinct patterns of dysfunctional connectivity in limbic and frontostriatal networks.Clustering patients on this basis enabled the development of diagnostic classifiers (biomarkers) with high (82%-93%) sensitivity and specificity for depression subtypes in multisite validation (n=711) and out-of-sample replication (n=477) data sets.These biotypes cannot be differentiated solely on the basis of clinical features, but they are associated with differing clinicalsymptom profiles.They also predict responsiveness to transcranial magnetic stimulation therapy (n=154).Our results define novel subtypes of depression that transcend current diagnostic boundaries and may be useful for identifying the individuals who are most likely to benefit from targeted neurostimulation therapies.
来源出版物:Nature Medicine, 2017, 23(1): 28-38
The Healthy Activity Program (HAP), a lay counsellor-delivered brief psychological treatment for severe depression, in primary care in India: A randomised controlled trial
Patel, Vikram; Weobong, Benedict; Weiss, Helen A
Abstract:Background: Although structured psychological treatments are recommended as first-line interventions for depression, only a small fraction of people globally receive these treatments because of poor access in routine primary care.We assessed the effectiveness and cost-effectiveness of a brief psychological treatment (Healthy Activity Program [HAP]) for delivery by lay counsellors to patients with moderately severe to severe depression in primary health-care settings.Methods: In this randomised controlled trial, we recruited participants aged 18-65 years scoring more than 14 on the Patient Health Questionnaire 9(PHQ-9) indicating moderately severe to severe depression from ten primary health centres in Goa, India.Pregnant women or patients who needed urgent medical attention or were unable to communicate clearly were not eligible.Participants were randomly allocated (1:1) to enhanced usual care (EUC) alone or EUC combined with HAP in randomly sized blocks (block size four to six [two to four for men]), stratified by primary health centre and sex, and allocation was concealed with use of sequential numbered opaque envelopes.Physicians providing EUC were masked.Primary outcomes were depression symptom severity on the Beck Depression Inventory version II and remission from depression (PHQ-9 score of <10) at 3 months in the intention to-treat population, assessed by masked field researchers.Secondary outcomes were disability, days unable to work, behavioural activation, suicidal thoughts or attempts, intimate partner violence, and resource use and costs of illness.We assessed serious adverse events in the per-protocol population.This trial is registered with the ISRCTN registry, number ISRCTN95149997.Findings:Between Oct 28, 2013, and July 29, 2015, we enrolled and randomly allocated 495 participants (247 [50%] to the EUC plus HAP group [two of whom were subsequently excluded because of protocol violations] and 248 [50%] to the EUC alone group), of whom 466 (95%) completed the 3 month primary outcome assessment (230 [49%] in the EUC plus HAP group and 236 [51%] in the EUC alone group).Participants in the EUC plus HAP group had significantly lower symptom severity (Beck Depression Inventory version II in EUC plus HAP group 19.99 [SD 15.70] vs 27.52 [13.26] in EUC alone group; adjusted mean difference -7.57 [95%CI-10.27 to -4.86];p<0.0001)and higher remission (147 [64%] of 230 had a PHQ-9 score of < 10 in the HAP plus EUC group vs 91 [39%] of 236 in the EUC alone group; adjusted prevalence ratio 1.61[1.34-1.93]) than did those in the EUC alone group.EUC plus HAP showed better results than did EUC alone for the secondary outcomes of disability (adjusted mean difference-2.73 [-4.39 to -1.06];p=0.001), days out of work (-2.29[-3.84 to -0.73];p=0.004), intimate partner physical violence in women (0.53 [0.29-0.96];p=0.04), behavioural activation (2.17 [1.34-3.00];p<0.0001), and suicidal thoughts or attempts (0.61 [0.45-0.83];p=0.001).The incremental cost per quality-adjusted life-year gained was$ 9333 (95%CI3862-28 169; 2015 international dollars),with an 87% chance of being cost-effective in the study setting.Serious adverse events were infrequent and similar between groups (nine [4%] in the EUC plus HAP group vs ten [4%] in the EUC alone group;p=1.00).Interpretation:HAP delivered by lay counsellors plus EUC was better than EUC alone was for patients with moderately severe to severe depression in routine primary care in Goa, India.HAP was readily accepted by this previously untreated population and was cost-effective in this setting.HAP could be a key strategy to reduce the treatment gap for depressive disorders, the leading mental health disorder worldwide.
来源出版物:Lancet, 2017, 389(10065): 176-185
The PHQ-9:Validity of a brief depression severity measure
Kroenke, K; Spitzer, RL; Williams, JBW
While considerable attention has focused on improving the detection of depression, assessment of severity is also important in guiding treatment decisions.Therefore, we examined the validity of a brief, new measure of depression severity.The Patient Health Questionnaire (PHQ) is a self-administered version of the PRIME-MD diagnostic instrument for common mental disorders.The PHQ-9 is the depression module, which scores each of the 9 DSM-IV criteria as “0” (not at all) to“3” (nearly every day).The PHQ-9 was completed by 6000 patients in 8 primary care clinics and 7 obstetricsgynecology clinics.Construct validity was assessed using the 20-item Short-Form General Health Survey, selfreported sick days and clinic visits.and symptom-related difficulty.Criterion validity was assessed against an Independent structured mental health professional (MHP)interview in a sample of 580 patients.As PHQ-9 depression severity Increased, there was a substantial decrease in functional status on all 6 SF-20 subscales.Also,symptom-related difficulty, sick days, and health care utilization increased.Using the MHP reinters view as the criterion standard, a PHQ-9 score greater than or equal to 10 had a sensitivity of 88% and a specificity of 88% for major depression.PHQ-9 scores of 5, 10, 15 and 20 represented mild, moderate, moderately severe, and severe depression, respectively.Results were similar in the primary care and obstetrics-gynecology samples.In addition to making criteria-based diagnoses of depressive disorders, the PHQ-9 Is also a reliable and valid measure of depression severity.These characteristics plus Its brevity make the PHQ-9 a useful clinical and research tool.Results from instrumented test runs with a high-speed train on a soft soil site in Sweden are presented.It is shown that large dynamic amplifications appear in the dynamic response of the rail/embankment/ground system as the train speed approaches an apparently critical value.The measured dynamic response is analyzed in detail, and it is shown that the critical speed is controlled by the minimum phase velocity of the first Rayleigh mode of the soil and embankment profile at the site.Moreover, it is shown that the critical speed and the amount of dynamic amplification also depend on a coincidence between characteristic wavelengths for the site and the distances between bogies and axles in the train.The displacement response is found to consist of a speed-independent portion in quasi-static equilibrium with the train loads and a dynamic portion representing freely propagating Rayleigh waves.An efficient computer code for the prediction of ground response to high-speed trains has been developed and its ability to reproduce the observed behavior is demonstrated.
来源出版物:Journal of General Internal Medicine, 2001,16(9): 606-613
Abstract:Transporter-facilitated uptake of serotonin(5-hydroxytryptamine or 5-HT) has been implicated in anxiety in humans and animal models and is the site of action of widely used uptake-inhibiting antidepressant and anti-anxiety drugs.Human 5-HT transporter (5-HTT) gene transcription is modulated by a common polymorphism in its upstream regulatory region.The short variant of the polymorphism reduces the transcriptional efficiency of the 5-HTT gene promoter, resulting in decreased 5-HTT expression and 5-HT uptake in lymphoblasts.Association studies in two independent samples totaling 505 individuals revealed that the 5-HTT polymorphism accounts for 3 to 4 percent of total variation and 7 to 9 percent of inherited variance in anxiety-related personality traits in individuals as well as sib ships.
来源出版物:Science, 1996, 274(5292): 1527-1531
Abstract:Objective: To review the literature of the validity of the Hospital Anxiety and Depression Scale (HADS).Method: A review of the 747 identified papers that used HADS was performed to address the following questions:(1) How are the factor structure, discriminant validity and the internal consistency of HADS? (2) How does HADS perforin as a case finder for anxiety disorders and depression? (3) How does HADS agree with other self-rating instruments used to rate anxiety and depression?Results: Most factor analyses demonstrated a two-factor solution in good accordance with the HADS subscales for Anxiety (HADS-A) and Depression (HADS-D),respectively.The correlations between the two subscales varied from 0.40 to 0.74 (mean 0.56).Cronbach’s alpha for HADS-A varied from 68 to 93 and for HADS-D from 67 to 90.In most studies an optimal balance between sensitivity and specificity was achieved when caseness was defined by a score of 8 or above on both HADS-A and HADS-D.The sensitivity and specificity for both HADS-A and HADS-D of approximately 0.80 were very similar to the sensitivity and specificity achieved by the General Health Questionnaire (GHQ).Correlations between HADS and other commonly used questionnaires were in the range 49 to 83.HADS was found to perform well in assessing the symptom severity and caseness of anxiety disorders and depression in both somatic, psychiatric and primary care patients and in the general population.
anxiety; depression; Psychiatric Status Rating Scales; psychometrics; reproducibility of results;sensitivity and specificity
责任编辑:卫夏雯
猜你喜欢
中国生殖健康(2020年4期)2021-01-18
中华养生保健(2020年5期)2020-11-16
中华养生保健(2020年7期)2020-11-16
中国生殖健康(2019年2期)2019-08-23
中国实用医药(2016年27期)2016-11-30
人间(2016年26期)2016-11-03
中国实用医药(2016年24期)2016-10-17
中国实用医药(2016年24期)2016-10-17
母子健康(2015年1期)2015-02-28
科学之友(2014年24期)2014-03-20