
The association of benign prostatic hyperplasia with lower urinary tract stones in adult men:A retrospective multicenter study
2018-04-19 05:38HungJungJinsungPrkWonKimHongWookKimHyungJoonKimSungwooHongJoYngHongChung
Asian Journal of Urology 2018年2期
J Hung Jung ,Jinsung Prk ,Won T Kim ,Hong Wook Kim ,Hyung Joon Kim ,Sungwoo Hong ,H Jo Yng ,Hong Chung *
a Department of Urology,Yonsei University,Wonju College of Medicine,Wonju,Korea
b Department of Urology,Eulji University,College of Medicine,Daejeon,Korea
c Department of Urology,Chungbuk National University,College of Medicine,Cheongju,Korea
d Department of Urology,Konyang University,College of Medicine,Daejeon,Korea
e Department of Urology,Dankook University,College of Medicine,Cheonan,Korea
f Department of Urology,Cheonan Hospital,Soonchunhyang University,College of Medicine,Cheonan,Korea
g Department of Urology,Konkuk University,School of Medicine,Chungju,Korea
1.Introduction
Benign prostatic hyperplasia(BPH)is highly prevalent in elderly men and affects approximately 50%of all men between 60 and 70 years old[1].Twenty-five percent to 50%of those with BPH have lower urinary tract symptoms(LUTS),such as flow impedance and sensations ofincomplete emptying,related to bladder outlet obstruction(BOO).Furthermore,BPH is associated with additional complications such as acute urinary retention,hematuria,urinary tract infection,and urinary stones[1,2].
Historically,lower urinary tract stones have been associated with a variety of disorders of the lower urinary tract,such as neurogenic bladder,BPH,and urethral stricture[3].These disorders are known to cause urinary stasis and infection.Bladder and urethral stones are two common types of lower urinary tract stones and account for 5%and 0.3%of all urinary stone diseases,respectively[3,4].Bladder calculi are commonly found in elderly men with lower urinary tract obstruction,such as BPH[5,6].Although urethral calculi primarily arise in association with urethral foreign bodies or anatomical anomalies such as urethral strictures or diverticula,the bladder is considered to be a primary source of urethral calculi in adults[3,4].
Although BPH is assumed to be associated with BOO and urinary stasis,the role of the prostate in the pathogenesis of lower urinary tract stones has not been well explored.In this study,we compared the characteristicsofmen with two types oflower urinary tract stonesto help elucidate the role of BPH in the formation of lower urinary tract stones.
2.Materials and methods
We retrospectively identified men with lower urinary tract stones who presented consecutively to three clinical centers in Korea(Eulji University Daejeon Hospital,Konkuk University Chungju Hospital,and Yonsei University Wonju Severance Christian Hospital)between May 2010 and May 2014.Two hundred and thirty-five patients were identified.We collected data from men over the age of 19 years old to exclude the patients with lower urinary tract stones associated with an anatomic abnormality such as a urethral stricture or diverticulum that were common in childhood.Bladder and urethral calculi were confirmed by computed tomography(CT)or cystoscopy.Urethral calculi were defined as any calculi in urethra from the meatus through to the bladder neck.Two patients were below the age of 19 years and were excluded.The medical records of 12 additional patients were not available for review.We reviewed the medical records of the remaining 221 patients.The Institutional Review Board of the Yonsei University Wonju College of Medicine approved this study(YWMR-15-5-059).
We divided the patients into two groups based on the location of the urinary stones:Group 1(bladder calculi)and Group 2(urethral calculi).The demographic and clinical data collected included patient age,medical history,clinical manifestations,laboratory findings,and radiologic findings.All 221 patients had undergone CT to investigate the presence and location of lower urinary tract stones,congenital abnormalities,and/or associated upper urinary tract pathology.Upper urinary tract pathologies included concurrent renal or upper urinary tract stone and unilateral hydronephrosis.We calculated prostate volume(PV)using a previouslydescribedmethodandellipsoidformula(PV=π/6×[width(cm)×thickness(cm)×length(cm)])[7].We estimated width(right-left)and thickness(anterior-posterior)on axial CT images,and we estimated length(cranial-caudal)on a coronal CT images.
We used the independentt-test,the Fisher exact test,and the chi-square test to compare the baseline characteristics of the two groups of patients.We performed univariate and multivariate analyses with a logistic regression model to examine the relationships between several independent variables and the two types of lower urinary tract stones.We performed all analyses with the IBM SPSS Statistics software,Version 20.0(IBM,Armonk,NY,USA).We considered two-tailedpvalues of less than 0.05 statistically significant.
3.Results
Of the 221 patients,194(87.8%)had bladder calculi and 27(12.2%)had urethral calculi.All of urethral calculi were found in prostatic or bulbar urethra.As shown in Table 1,the most common symptoms of bladder calculi were hematuria(37.1%)and voiding dysfunction(32.5%).Five patients(2.6%)with bladder calculi presented acute urinary retention,however it might result from BPH or bladder calculi,itself.Urethral calculi were commonly associated with voiding dysfunction(63.0%)and acute urinary retention(18.5%)secondary to urinary tract obstruction.All of the patients with urethral calculi were symptomatic,whereas 15.5%of patients with bladder calculi were asymptomatic and diagnosed incidentally during routine health examination.
Table 2 summarizes the clinical characteristics of men with lower urinary tract calculi.Both the mean age and the mean PV of Group 1 were significantly higher than those of Group 2(p<0.001).Upper urinary tract pathology was present in 31.4%and 63.0%of patients in Group 1 and Group 2,respectively,which was significantly more common in Group 2 than in Group 1(p=0.005).Although patients with bladder calculi had a higher prevalence of neurologic disease,diabetes mellitus,and bacteriuria than those with urethral calculi,there were no significant differences between the two groups in the prevalence of neurologic disease,diabetesmellitus,urologicalanomalies,or bacteriuria.The creatinine level was similar in two groups.
Univariateanalysis revealedthat thepresenceof bladder calculi was significantly associated with age(odds ratio[OR]=1.072,95%confidenceinterval[CI]:1.040-1.105),PV(OR=1.076,95%CI:1.033-1.120),and upper urinary tract pathology(OR=0.278,95%CI:0.114-0.628)compared to urethral calculi.Multivariate analysis showed that age and PV were statistically significant predictors of bladder calculi(OR=1.075,95%CI:1.023-1.129 andOR=1.069,95%CI:1.017-1.123,respectively)compared to urethral calculi,while upper urinary tract pathology was a statistically significant predictorofurethralcalculi(OR=3.468,95%CI:1.093-10.999)compared to bladder calculi.
4.Discussion
Lower urinary tract stones are relatively rare,with an incidence rate of less than 10%[4].However,their clinical symptoms may be as troublesome as those of upper urinary tract stones.Lower urinary tract stones are traditionally classified as migrant,primary idiopathic,and secondary[4,5].Although numerous studies have suggested that lower urinary tract stones are associated with urinary stasis caused by BPH,the contribution of BPH to the pathogenesis of urethral calculi appear to be different from its contribution to bladder calculi[3-6].Our findings are consistent with this theory,as PV was shown to be associated with bladder calculi and not with urethral calculi.
Crawford et al.[8]demonstrated that patients with a PV of 31 mL or higher had a significantly greater risk of acute urinary retention and need for invasive surgical treatment.Philippou et al.[9]suggested that BOO may be the prime etiologic factor in 75%of cases of bladder calculi and that the presence of bladder calculi is an absolute indication for surgical treatment of prostate.A recent study by Childs et al.[10]found that older age,longer intravesical prostatic protrusion,and lower peak urinary flow were important predictors of bladder calculi in patients with BPH.More speci fically,larger PV,which was associated with longer intravesical prostatic protrusion,was a signi ficant predictor of bladder calculi.This is consistent with our findings,which showed that patients with bladder calculi indeed had larger PV when compared to those with urethral calculi.
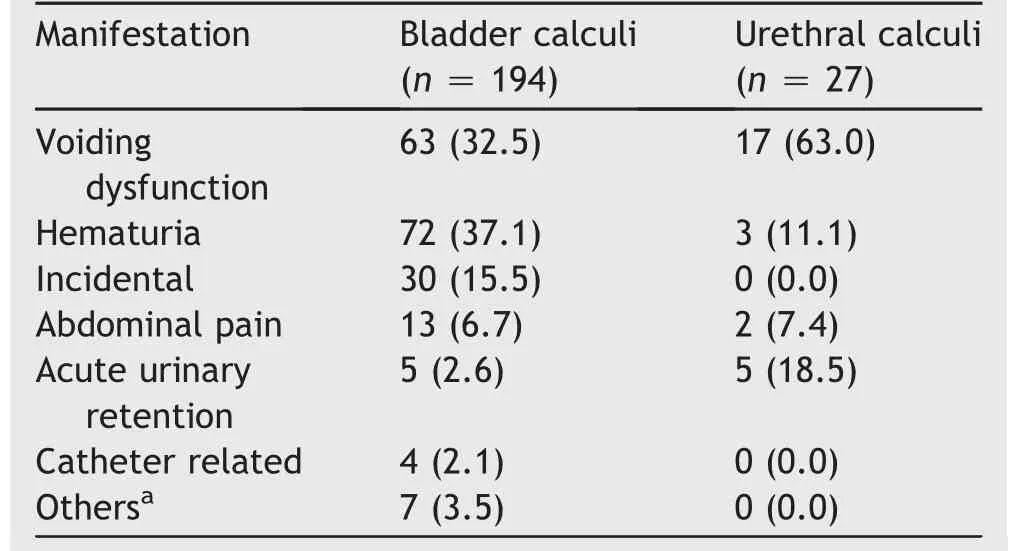
Table 1 Clinical manifestations of lower urinary tract stones(n,%).
a
Age is also a well-known etiologic factor associated with BPH.The incidence of BPH increases rapidly with age and reaches nearly 100%in the ninth decade[1].A large-scale Korean cohort study confirmed this finding and showed that PV was associated with advancing age[11].In our current study the mean age of patients with urethral calculi was about 10 years younger than those with bladder calculi.These findings reinforce the theory that PV is an independent risk factor for bladder calculi,as confirmed by our multivariate analysis.
Urethral calculi are commonly reported in endemic areas,such as Asia and the Middle East,where there is a high incidence of bladder calculi[4,12].This suggests that urethral calculi may result from bladder migration or may develop concurrently due to an anatomical anomaly.Anatomical changes of the urethra have been found in almost half of patients with urethral calculi[13,14].However,it is reasonable to assume that migratory stones account for a large proportion of the urethral calculi found in healthy,and it has been suggested that not all urethral calculi originate in the bladder[4].Moreover,the incidence of concurrent urinary stones in patients with urethral calculi is 32%-91%[14,15].If urethral calculi stem from migration,then the bladder and upper urinary tract are strong candidates for the primary source of such stones,and in the past the bladder has indeed been believed to be the primary source[14].However,in our study 63.0%(17/27)of patients with urethral calculi had a concurrent upper urinary stone.This indicates that urethral calculi,while migratory,may actually form in the upper urinary tract rather than in the bladder.Furthermore,PV was inversely correlated with urethral calculi compared to bladder calculi.This finding suggests that urethral calculi,as opposed to bladder calculi,are not a consequence of BPH progression.
This study has several limitations.First,urinary tract stone disease may be associated with metabolic disorders,which we did not report on.Childs et al.[10]reported that patients with bladder calculi had metabolic abnormalities on 24 h urine supersaturation studies.Additional information about family history and further metabolic evaluation may have helped uncover potential primary causes of urinary tract stone disease.Second,our data did not include the compositional analysis of the lower urinary tract stones.Although few published studies have reported the composition of lower urinary tract stones,the composition can imply the origin of the stones.Struvite and uric acid stones are regarded as migratory stones from the bladder.In contrast,calcium oxalate and cysteine stones are thought to originate from the upper urinary tract[3,4,6,12].Finally,our study does not address whether or not concurrent upper urinary tract pathologies,such as upper urinary stones or unilateral hydronephrosis,represent evidence of stone migration from the kidneys.A key strength of our study is that all of the patient records included CT images,which allowed us to estimate PV and to determine the actual presence and location of stone disease.
Despite these potential limitations,this study provides further insight into the formation of lower urinary tract stones.Specifically,PV,which increases with age,is an independent risk factor only for the development of bladder calculi.Secondarily,urethral calculi,while migratory,may actually form in the upper urinary tract rather than in the bladder.This new information has significant implications for the diagnostic workup and treatment of men who present with BPH and/or with symptoms of lower urinary tract stones.
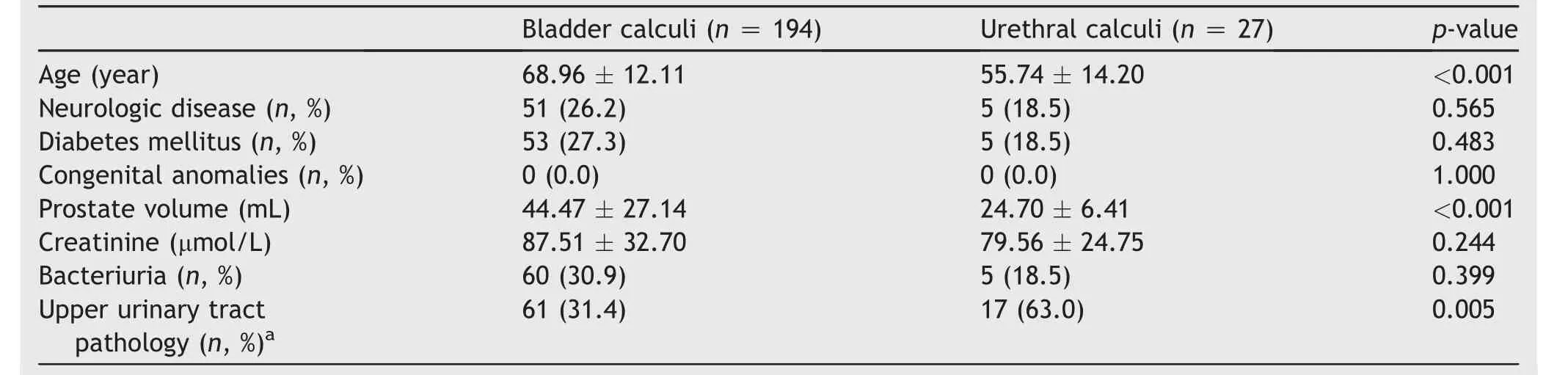
Table 2 Baseline characteristics of men with lower urinary tract stones.
a
5.Conclusion
Our results suggest that most urethral calculi in men originatefromupper urinary stones unless thereis an anatomical disorder also present.In contrast,bladder calculi are mainly correlated with bladder outlet obstruction such as BPH.Therefore,these two types of lower urinary stones are unlikely to share similar pathophysiology regarding their origin.More research on this topic will increase our understanding of the origin of urethral calculi.
Con flicts ofinterest
The authors declare no conflict ofinterest.
[1]Yoo TK,Cho HJ.Benign prostatic hyperplasia:from bench to clinic.Korean J Urol 2012;53:139-48.
[2]Oelke M,Bachmann A,Descazeaud A,Emberton M,Gravas S,Michel MC,et al.EAU guidelines on the treatment and followup of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction.Eur Urol 2013;64:118-40.
[3]Takasaki E,Suzuki T,Honda M,Imai T,Maeda S,Hosoya Y.Chemical compositions of 300 lower urinary tract calculi and associated disorders in the urinary tract.Urol Int 1995;54:89-94.
[4]Kamal BA,Anikwe RM,Darawani H,Hashish M,Taha SA.Urethral calculi:presentation and management.BJU Int 2004;93:549-52.
[5]Hammad FT,Kaya M,Kazim E.Bladder calculi:did the clinical picture change?Urology 2006;67:1154-8.
[6]Douenias R,Rich M,Badlani G,Mazor D,Smith A.Predisposing factors in bladder calculi.Review of 100 cases.Urology 1991;37:240-3.
[7]Kang TW,Song JM,Kim KJ,Byun HK,Kim YJ,Chung HC,et al.Clinical application of computed tomography on prostate volume estimation in patients with lower urinary tract symptoms.Urol J 2014;11:1980-3.
[8]Crawford ED,Wilson SS,McConnell JD,Slawin KM,Lieber MC,Smith JA,et al.Baseline factors as predictors of clinical progression of benign prostatic hyperplasia in men treated with placebo.J Urol 2006;175:1422-7.
[9]Philippou P,Moraitis K,Masood J,Junaid I,Buchholz N.The management of bladder lithiasis in the modern era of endourology.Urology 2012;79:980-6.
[10]Childs MA,Mynderse LA,Rangel LJ,Wilson TM,Lingeman JE,Krambeck AE.Pathogenesis of bladder calculi in the presence of urinary stasis.J Urol 2013;189:1347-51.
[11]Park DS,Hong JY,Hong YK,Lee SR,Hwang JH,Kang MH,et al.Correlation between serum prostate specific antigen level and prostate volume in a community-based cohort:large-scale screening of 35,223 Korean men.Urology 2013;82:1394-9.
[12]Verit A,Savas M,Ciftci H,Unal D,Yeni E,Kaya M.Outcomes of urethral calculi patients in an endemic region and an undiagnosed primary fossa navicularis calculus.Urol Res 2006;34:37-40.
[13]Selli C,Barbagli G,Carini M,Lenzi R,Masini G.Treatment of male urethral calculi.J Urol 1984;132:37-9.
[14]SharfiAR.Presentation and management of urethral calculi.Br J Urol 1991;68:271-2.
[15]Koga S,Arakaki Y,Matsuoka M,Ohyama C.Urethral calculi.Br J Urol 1990;65:288-9.
 Asian Journal of Urology2018年2期
Asian Journal of Urology2018年2期
- Asian Journal of Urology的其它文章
- Tissue engineering for urinary tract reconstruction and repair:Progress and prospect in China
- Overcoming scarring in the urethra:Challenges for tissue engineering
- Emergency treatment of male blunt urethral trauma in China:Outcome of differentmethods in comparison with other countries
- Prevention strategies for ureteral stricture following ureteroscopic lithotripsy
- Management of complex and redo cases of pelvic fracture urethral injuries
- The effect of adjunct caudal block on postoperative analgesia in robot-assisted laparoscopic radical prostatectomy:A prospective randomized controlled,single blinded pilot study in a tertiary centre