
Diffuse large B-cell lymphoma arising from follicular lymphoma with warthin’s tumor of the parotid gland - immunophenotypic and genetic features:A case report
2019-04-22 06:28ChangSongWangXiaChuDiYangLeiRenNianLongMengXueXiaLvTianYunYanShaCao
World Journal of Clinical Cases 2019年22期
Chang-Song Wang, Xia Chu, Di Yang, Lei Ren, Nian-Long Meng, Xue-Xia Lv, Tian Yun, Yan-Sha Cao
Chang-Song Wang, Nian-Long Meng, Xue-Xia Lv, Tian Yun, Yan-Sha Cao, Department of Pathology, 989th Hospital of PLA, Luoyang 471000, Henan Province, China
Abstract
Key words: Diffuse large B cell lymphoma; Warthin’s tumor; Parotid gland; Follicular lymphoma; Case report; Genetic feature
INTRODUCTION
Warthin’s tumor (WT) is associated with different lymphoproliferative disorders in the salivary glands.It is the second most common benign neoplasm of the salivary gland and occurs almost exclusively in the parotid gland.WT is composed of several cysts that are lined with tall, bilayered oncocytic columnar cells and lymphoid stroma.Within WT, the two composed parts rarely transform into carcinoma or lymphoma,and when it does, the carcinoma is the most common type.On occasion, some lymphomas contain the normal residual lymphoid stroma, and the majority of the stroma of WT is entirely replaced by neoplastic cells.However, the lymphoid stroma of WT comprises systemic lymphoid tissue based on the foundation that most lymphomas arising from WT are disseminated disorders.Approximately 28 cases of lymphomas with WT have been reported in the English literature, and most of them were non-Hodgkin lymphomas; only a few cases were Hodgkin lymphomas (Table 1).Follicular lymphoma (FL) is actually a prevalent subtype.The diffuse large B cell lymphoma (DLBCL) arising from FL also involves the parotid gland and is the first known report.In this paper, we studied a case of B cell non-Hodgkin lymphoma that arose from the stroma of WT and transformed to DLBCL.In addition, the molecular genetic characteristics and immunotypes of these genes were studied.
Table 1 Summary of lymphomas association with Warthin’s tumor
CASE PRESENTATION
Chief complaints
A 67-year-old man was admitted to the hospital with a slowly enlarging right cheek mass for 12 years.At first, the mass was about the size of a peanut without any discomfort; the mass grew slowly and began to change in size over 2 mo before he was admitted to our hospital.Over time, the patient felt mild local pain and right cheek discomfort.
History of present illness
The patient had no history of the present illness.
History of past illness
His medical history included a hepatitis B virus infection for 20 years and 30 years of smoking.
Personal and family history
His family histories and previous clinical and genetic disease histories were unremarkable.
Physical examination upon admission
A solitary, hard mass approximately 10.0 cm × 10.0 cm × 8.0 cm in size at the tail of the right parotid gland was examined, and there were no swollen lymph nodes in the adjacent region.
Laboratory examinations
There were no special laboratory examination results.
Imaging examinations
Contrast-enhanced computed tomography (CT) scans of the neck and parotid gland demonstrated a heterogeneous echo-textured mass in the right parotid gland measuring 10 cm × 10 cm × 8 cm without pathologic cervical adenopathy.The facial nerve function was intact.
Pathological findings
Gross examination of the excised specimen showed a gray-red and gray-white appearance, and a soft-textured, lobulated external surface neoplasm that measured 9 cm × 8 cm × 7 cm was surrounded by relative normal parotid gland tissue.In cross section, the cut surfaces of the neoplasm were multicystic and had a homogeneous scaly appearance, and a small amount of fluid was discovered in the cyst.Microscopically, bilayered oxyphilic, cuboidal or polygonal epithelium cells and lymphoid intraparenchymal components were observed, which are typical WT histological characteristics (Figure 1A).Simultaneously, many medium- to large-sized lymphoid cells were observed diffusely in other parts of the neoplasm, and a few secondary lymphoid follicles were observed at the center or edge of the neoplasm(Figure 1B and 1C).The lymphoid cells had irregular nuclear contours, indistinct nucleoli, and scant cytoplasm with atypia contours and nucleus.At the border of the epithelium, lymphoepithelial lesions were identified (Figure 1D).Necrosis was observed locally, and mitoses were approximately 3-4/10 high-power fields.
Immunohistochemical staining and results
At the same time, immunohistochemical staining was performed according to the reported literature.Formalin-fixed paraffin-embedded sample blocks were cut into 3 μm-thick sections and used for immunohistochemical staining.High-pressure heating was performed for antigen retrieval in 10 mmol citrate buffer (pH 6.0).The primary antibodies were added and incubated overnight at 4 °C or 37 °C for 3 h according to the manufacturer’s instructions.The secondary antibodies were added and incubated on the next day and then visualized with DAB.
Immunohistochemical staining showed that the columnar oncocytic cells were positive for AE1/AE3 (Figure 2A) and CK18; neoplastic cells located in coarctate follicles were positive for CD20 (Figure 2B), Pax-5 (Figure 2C), bcl-2 (Figure 2D) and bcl-6, weakly positive for CD3, CD5 and CD45RO, and negative for CD5, CD21, CD10(Figure 2E), CyclinD1, CD15, CD30, CD1a, ALK, CD4, CD123, CD56, S-100, and human melanoma black 45.The adjacent diffusely medium- to large-sized lymphoid cells were positive for Pax-5, bcl-6, CD20 (Figure 2F), MUM-1 (Figure 2G), bcl-2,Foxp1, andCD79a and negative for CD5, CD21, CD10, CyclinD1, CD3, and CD45RO.The Ki-67 proliferation index was estimated at approximately 80% (Figure 2H).
Molecular genetic detection
Fluorescent in situ hybridization (FISH) analysis with the dual-color dual fusion MYC(8q24), bcl-2 break-apart rearrangement (18q21), bcl2/IGH fusion translocation t(14;18), bcl-6 break-apart rearrangement (3q27) and MYC/IGH fusion translocation t(14;18) probes were performed on the tissue mass.The results showed that there were no fusion genes or break-apart rearrangements, except for bcl-6 (3q27) (Figure 3A-D).
FINAL DIAGNOSIS
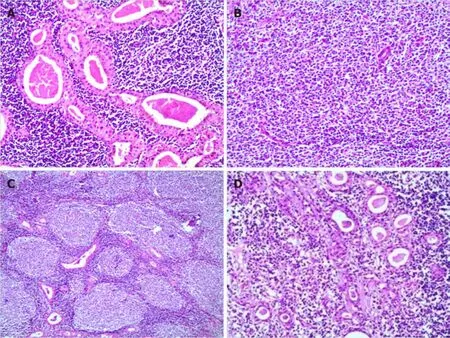
Figure 1 Morphological characteristic of Warthin’s tumor and lymphoma.
Epstein Barr virus (EBV) DNA was also detected using EBV-encoded RNA chromogenic in situ hybridization, and the result was negative in tumor cells.According to the histological features, immunophenotype and FISH results, the patient was diagnosed with “WT with diffuse large B-cell lymphoma (non-germinal center formation germinal center blastocyte type) that was transformed from FL in the parotid gland”.
TREATMENT
The patient underwent a right superficial parotidectomy, and the tissue was sent for pathological examination.No swollen lymph nodes or neoplasms were found along the right carotid arteries and sternocleidomastoid muscle.
OUTCOME AND FOLLOW-UP
Soon after, full-body fluorine-18 fluorodeoxyglucose positron emission tomography/CT were performed to judge the clinical stage and extent of the lesion,and no potential lesions were detected.Bone marrow was not involved, which was detected by biopsy.The patient was classified as stage 3A.The patient did not receive any treatment because his health was too poor to tolerate any medicine.The patient survived 6 mo after diagnosis.
DISCUSSION
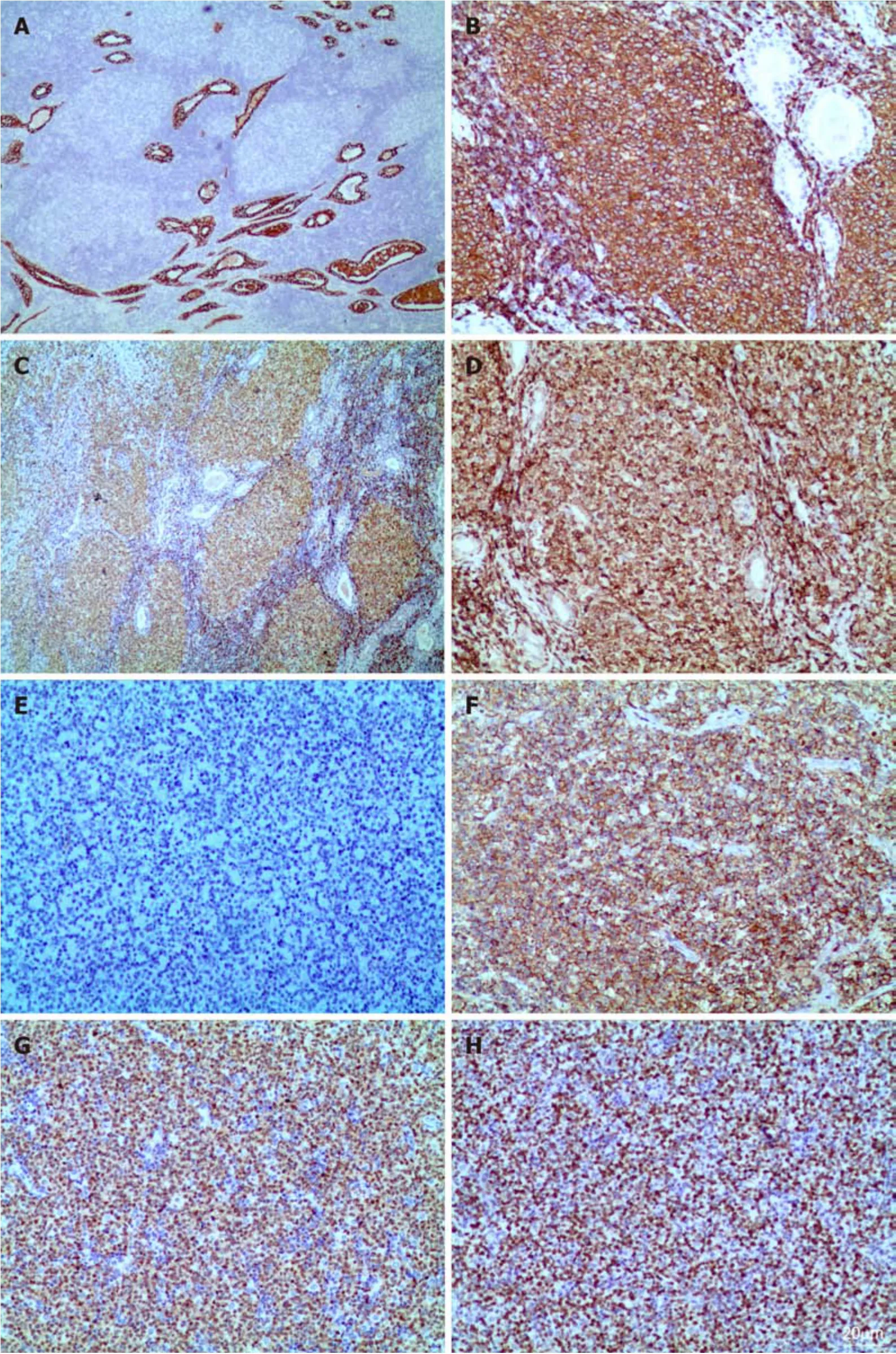
Figure 2 Immunotype of lymphoma with Warthin’s tumor.
Malignant transformation in WT is rare and only occurs in approximately 1% of WT cases.It can affect either the epithelial or lymphoid component.In the majority of cases, this transformation occurs in the epithelium, and few cases involve the lymphoid stroma.Lymphoma originating from the stromal component of the parotid gland is extremely rare, especially in WT.According to the English and Chinese literature, 28 cases of WT with lymphoma have been reported to date.We concluded that the most common subtypes of lymphoma were FLs (10 cases)[1-10], followed by Hodgkin’s lymphoma (4 cases)[11-14]and diffuse large B cell lymphoma (6 cases)[4,15-18].The others were small lymphocytic lymphoma/chronic lymphocytic leukemia (3 cases)[19-21], mantle cell lymphoma (1 case)[22], extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (1 case)[23], Lennert lymphoma (1 case)[24],peripheral T-cell lymphoma (2 cases)[25,26], and T lymphoblastic leukemia/lymphoma(1 case)[27].In these patients, 4 cases of T-cell lymphoma and 25 cases of B-cell lymphoma were observed.The age of reported patients with lymphoma and WT ranged from 49 to 102 years, with an average age of 69 ± 11.3 years.There were 25 males (86.2%) and 4 females (13.8%), and the ratio was 6.3:1, indicating that this kind of disease is most likely involved in middle-age and older males.In these cases, only 1 case involved the bilateral parotid gland, and the others involved a single site.One case involved the upper right cervical lymph node.All of these cases were diagnosed accurately after WT excision.In our case, the patient was an older man and had a 12-year clinical history, which is consistent with the reported literature.He was promptly diagnosed after the excision of the parotid gland mass.
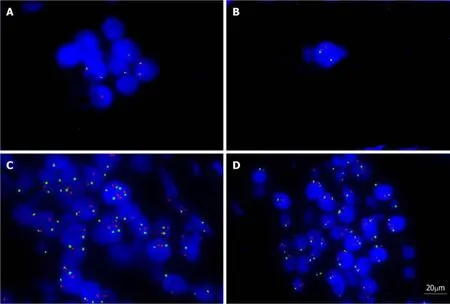
Figure 3 Fluorescent in situ hybridization studies using dual-color dual fusion bcl-2 break apart rearrangement (18q21), bcl-6 break apart rearrangement(3q27), MYC (8q24), and MYC/IGH fusion translocation t (14;18) probes.
Due to the low incidence, the previously reported cases spanned a long time period, and the evidence of diagnosis was different.Molecular detection, FISH analysis, gene rearrangement and flow cytometry (FCM) analysis were not performed in most of these cases.Only a few cases were reported for FCM detection[19],immunoglobulin monoclonal gene rearrangement[1,21], PCR detection[23]or detection of bcl-2 mcr/JH fusion DNA sequences[1].Our case was detected by the FISH method,and the result showed that only bcl-6 break-apart rearrangement (3q27) was observed in tumor cells of DLBCL.We reviewed the published paper and found that the CD10 was detected in 1 case and the result was negative[17], the others were not mentioned for detection.Bcl-2 rearranged were detected in 2 cases and the results revealed that the bcl-2 gene was rearranged, consistent with the presence of the t (14; 18) (q32; q21)translocation[1,2].Our case showed that no bcl-2 break-apart rearrangement (18q21)and bcl2/IGH fusion translocation t(14; 18).CD10 staining positive andbcl2gene rearrange were typically seen in FL which was developed in the lymph nodes.And CD10 expression and bcl-2 status were reported in few cases, especially in malignant lymphomas which were occurred in WT.
The mechanism of malignant transformation in WT is not fully understood.Smoking was presumed to be a first-hand factor with WT because smokers have an estimated risk 8 times that of nonsmokers.However, we reviewed the literature, and the results showed that only 5 patients had a history of smoking[12,16,17,19], and the smoking history of 2 patients exceeded 50 years[12,17]; the others did not mention smoking history.Therefore, smoking may not be the key cause of lymphoma with WT.Another etiological factor may be radiation exposure, as lymphomas arising within a WT occur after receiving previous radiation[28].In our case, the patient had a 30-year history of smoking and no history of previous radiation exposure, so other unknown factors may cause the lymphoma involving WT.
The relationship between EBV infection and lymphoma with the parotid gland is unknown; based on a previous report, only 1 case of EBV-positive DLBCL of an elderly patient with WT was reported, and its clinical course was aggressive[17]; the others were negative for EBV infection, including our case.The mechanism of EBV infection in malignant lymphomas occurred in WT was unclear for the low incidence.
The prognosis of lymphomas with WT is discrepant because the incidence is too low.The reported literature showed that the valuable prognosis index had a high mitotic rate and a high Ki-67 index or a large number of positive cells.Although the Ki-67 index was up to 80% in our case, the patient remained alive 6 months after the operation.
As we have known that the lymphoid component of WT is part of the systemic lymphoid tissue, many lymphocytes will be found in the excised parotid gland, so lymphomas with WT arise from lymphoid cell transformation or chronic inflammation.The extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue may be the most common subtype neoplasm in WT; however, only 1 case of extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue has been reported, and the majority of lymphomas with WT are FCL.Second, another query or debate is whether the lymphoma is coincidental or arises from the lymphoid stroma of WT; few patients with lymphoma in WT were reported to have systemic lymphoma by systemic fluorine-18 fluorodeoxyglucose positron emission tomography/CT span.
CONCLUSION
In conclusion, this case is the first reported case of DLBCL that was transformed from FL in a WT excision specimen.This is a very rare lesion with an extremely low incidence and unclear biological behavior.Therefore, we should carefully examine the tumor stroma during the pathological examination because the neoplastic cells can be confused with the normal reactive lymphoid component in WT.Requisite molecular detections are performed when the diagnosis of lymphoma with WT is dubious.
 World Journal of Clinical Cases2019年22期
World Journal of Clinical Cases2019年22期
- World Journal of Clinical Cases的其它文章
- Colorectal cancer:The epigenetic role of microbiome
- Human podocyte injury in the early course of hypertensive renal injury
- Relationship between acute hypercarbia and hyperkalaemia during surgery
- Surgical treatment ofpatients with severe non-flail chest rib fractures
- Super-selective arterial embolization in the control of acute lower gastrointestinal hemorrhage
- End-stage liver disease score and future liver remnant volume predict post-hepatectomy liver failure in hepatocellular carcinoma