依达拉奉在全麻下行胸腔镜下食管癌根治术患者中的应用效果
2020-06-29 07:37唐玉茹帅训军徐堂文李会孙常荣艾登斌
中国当代医药 2020年13期
关键词:依达拉奉
唐玉茹 帅训军 徐堂文 李会 孙常荣 艾登斌

[摘要]目的 探討依达拉奉在全麻胸腔镜下食管癌根治术患者中的应用效果。方法 选取2016年12月~2017年8月于青岛市立医院行全麻胸腔镜下食管癌根治术的60例患者作为研究对象,年龄35~68岁,美国麻醉医师协会(ASA)Ⅰ~Ⅱ级。采用随机数字表法将其分为EI和CG组,每组各30例。EI组患者麻醉诱导后将依达拉奉30 mg加入0.9%氯化钠100 ml中静滴,CG组患者麻醉诱导后给予等量0.9%氯化钠静滴。分别于麻醉后切皮前(T0)、单肺通气60 min(T1)、单肺通气90 min(T2)、单肺通气120 min(T3)、膨肺30 min(T4)及术后60 min(T5)采取静脉血,采用酶联免疫吸附法(ELISA)检测磷脂酰肌醇-3激酶(PI3K)、磷酸化蛋白激酶B(p-AKT)、活化蛋白-1(AP-1)、白介素-8(IL-8)、肿瘤坏死因子-α(TNF-α)和超氧化物歧化酶(SOD)表达水平,并比较两组患者的手术情况。结果 两组患者的手术时间、术中单肺通气时间、麻醉时间、手术径路、麻醉后监测治疗室(PACU)时间比较,差异无统计学意义(P>0.05)。两组患者T1~T5时血浆中的PI3K、p-AKT、AP-1、IL-8及TNF-α表达水平均高于T0,差异有统计学意义(P<0.05);两组患者T1~T5时血浆中的SOD表达水平低于T0时,差异有统计学意义(P<0.05);EI组患者T1~T5时血浆中的PI3K、p-AKT、AP-1、IL-8及TNF-α表达水平均低于CG组,差异有统计学意义(P<0.05);EI组患者T1~T5时血浆中的SOD表达水平高于CG组,差异有统计学意义(P<0.05)。结论 依达拉奉对单肺通气性肺损伤有保护作用,通过减少促炎性细胞因子的释放,减少术后肺炎性反应。
[关键词]依达拉奉;单肺通气;肺损伤
[中图分类号] R614 [文献标识码] A [文章编号] 1674-4721(2020)5(a)-0107-04
Application effect of Edaravone in patients undergoing thoracoscopic esophagectomy under general anesthesia
TANG Yu-ru1 SHUAI Xun-jun2 XU Tang-wen3▲ LI Hui2 SUN Chang-rong2 AI Deng-bin2
1. Qingdao Mental Health Center, Qingdao University, Shandong Province, Qingdao 266034, China; 2. Department of Anesthesiology, Qingdao Municipal Hospital, Shandong Province, Qingdao 266000, China; 3. Department of Anesthesiology, the Affiliated Hospital of Qingdao University, Shandong Province, Qingdao 266000, China
[Abstract] Objective To investigate the application effect of Edaravone in patients undergoing thoracoscopic esophagectomy under general anesthesia. Methods A total of 60 patients undergoing thoracoscopic esophagectomy under general anesthesia in Qingdao Municipal Hospital from December 2016 to August 2017 were selected as the research subjects, aged 35-68 years old, with American Society of Anesthesiologists (ASA) Ⅰ-Ⅱ grades. All patients were divided into EI group and CG group according to the random number table method, 30 cases in each group. Patients in the EI group were given intravenous infusion of Edaravone 30 mg in 0.9% sodium chloride 100 ml after induction of anesthesia, while those in the CG group were given intravenous infusion of equal amounts of sodium chloride after induction of anesthesia. The venous blood samples were obtained at the following time points respectively: before skin incision after anesthesia (T0), one lung ventilation 60 min (T1), one lung ventilation 90 min (T2), one lung ventilation 120 min (T3), dilated lung 30 min (T4) and 60 min after operation (T5), and enzyme-linked immunosorbent assay (ELISA) was used to detect phosphatidyl inositol 3-kinase (PI3K), phosphorylated protein kinase B (p-AKT), activating protein-1 (AP-1), and interleukin-8 (IL-8), tumor necrosis factor-α (TNF-α) and superoxide dismutase (SOD) expression levels. The operation of the two groups of patients was compared. Results There were no significant differences in the operation time, intraoperative one lung ventilation time, anesthesia time, operation path, and post-anesthesia care unit (PACU) time between the two groups (P>0.05). The expression levels of PI3K, p-AKT, AP-1, IL-8 and TNF-α in the plasma of the two groups at T1-T5 were higher than those at T0, and the differences were statistically significant (P<0.05). The expression levels of SOD in the plasma of the two groups at T1-T5 were lower than those at T0, and the differences were statistically significant (P<0.05). The expression levels of PI3K, p-AKT, AP-1, IL-8 and TNF-α in the plasma of patients in EI group at T1-T5 were lower than those in CG group, and the differences were statistically significant (P<0.05). The expression levels of SOD in the plasma of patients in EI group at T1-T5 were higher than those in CG group, and the differences were statistically significant (P<0.05). Conclusion Edaravone has a protective effect on one lung ventilation-induced lung injury, and reduces the postoperative pulmonary inflammatory response by reducing the release of pro-inflammatory cytokines.
[Key words] Edaravone; One lung ventilation; Lung injury
单肺通气(one lung ventilation)目前广泛用于心胸外科手术,在减轻术侧肺牵拉损伤同时,可为手术创造清晰视野,保护健侧肺安全。然而,长时间单肺通气能激活严重氧化应激反应,而触发炎性反应,这是术后肺功能紊乱的原因之一[1-2]。依达拉奉,作为一种外源性自由基清除剂,有清除自由基和抑制脂质过氧化作用[3-4]。磷脂酰肌醇-3激酶/蛋白激酶B/活化蛋白-1(phosphatidyl inositol 3-kinase/protein kinase B/activating protein-1,PI3K/AKT/AP-1)信号通路是保护机体应应激反应的重要通路[5],PI3K/AKT/AP-1是否参与到依达拉奉对单肺通气手术的保护机制尚不明确。本研究选取于青岛市立医院行全麻胸腔镜下食管癌根治术的60例患者作为研究对象,旨在分析依达拉奉在全麻下行胸腔镜下食管癌根治术患者中的应用效果,以期为临床提供参考,现报道如下。
1资料与方法
1.1一般资料
选取2016年12月~2017年8月于青岛市立医院行全麻胸腔镜下食管癌根治术的60例患者作为研究对象,采用随机数字表法将其分为EI和CG组,每组各30例。纳入标准:年龄35~68岁,美国麻醉医师协会(American Society of Anesthesiologists,ASA)Ⅰ~Ⅱ级。排除标准:术前已存在肺或其他感染性疾病;术前有化疗、放疗及糖皮质激素使用者。本研究已获得青岛市立医院医学伦理委员会批准,所有患者均签署知情同意书。为保证研究条件的一致性,均由同一位麻醉医师实施麻醉和由同组手术医师实施手术。两组患者的性别、年龄、体重指数(body mass index,BMI)、术前肺功能指标[第1秒用力呼气容积(forced expiratory volume in one second,FEV1)、用力肺活量(forced vital capacity,FVC)、FEV1/FVC]等一般资料比较,差异无统计学意义(P>0.05)(表1),具有可比性。
1.2麻醉方法
患者入室后开放静脉通路,常规监测心电图、脉搏、血氧饱和度、无创血压、呼气末二氧化碳和气道阻力等。麻醉诱导后EI组患者给予依达拉奉(商品名:必存,江苏先声药业有限公司,生产批号:80-130103)30 mg加入0.9%氯化钠100 ml,30 min内静脉滴注完毕;CG组患者给予等量0.9%氯化钠静滴。
麻醉诱导:静脉注射咪唑安定(恩华有限责任公司,生产批号:H10980025)0.03 mg/kg、芬太尼(宜昌人福公司,生产批号:81D120)3 μg/kg、顺式阿曲库胺(江苏恒瑞医药有限公司,生产批号:190307BL)0.15 mg/kg,高流量吸入8%七氟醚(江苏恒瑞医药有限公司,生产批号:H20070172),意识消失后将气流量降至2 L/min,七氟醚呼气末浓度降至2%。肌肉完全松弛后,行双腔支气管导管插管。
麻醉维持:两组患者均间断静脉注射维库溴铵0.04~0.08 mg/kg、芬太尼0.05~0.10 mg,七氟醚呼气末浓度维持在1.7%~2.8%。手术开始前10 min行单肺通气。术中通过调节麻醉药调整麻醉深度,维持呼气末二氧化碳在35~40 mmHg之间,平均动脉压(mean arterial pressure,MAP)、心率(heart rate,HR)的波动范围不超过基础值20%。其中,术中出现体温<35.5℃或>37.5℃,心肺复苏等抢救情况以及术中出血>500 ml或异体输血者排除于本实验。
1.3观察指标
记录两组患者的手术情况,包括手术径路(左/右进胸)、术中单肺通气时间、麻醉时间、手术时间、麻醉后监测治疗室(post-anesthesia care unit,PACU)时间以及麻醉后切皮前(T0)、单肺通气60 min(T1)、单肺通气90 min(T2)、单肺通气120 min(T3)、膨肺30 min(T4)及术后60 min(T5)各个时间点的中心静脉压(central venous pressure,CVP)、MAP、HR。分别在以上时间点通过中心静脉采取静脉血5 ml,留取血样后离心,取上清液置于-80℃冰箱下保存,采用酶联免疫吸附法(enzyme-linked immunosorbent assay,ELISA)测定血浆中PI3K、磷酸化AKT(p-AKT)、AP-1、白介素-8(interleukin-8,IL-8)、肿瘤坏死因子-α(tumor necrosis factor-α,TNF-α)和超氧化物歧化酶(superoxide dismutase,SOD)的表达水平。PI3K、p-AKT、AP-1、IL-8、TNF-α及SOD定量ELISA试剂盒,均由北京环亚泰克生物医学技术有限公司提供,严格按照说明书进行操作。
1.4统计学方法
采用SPSS 18.0统计学软件进行数据分析,计量资料用均数±标准差(x±s)表示,多组间比较用单因素方差分析,两组间比较采用t检验;计数资料采用率表示,组间比较采用χ2检验,以P<0.05为差异有统计学意义。
2结果
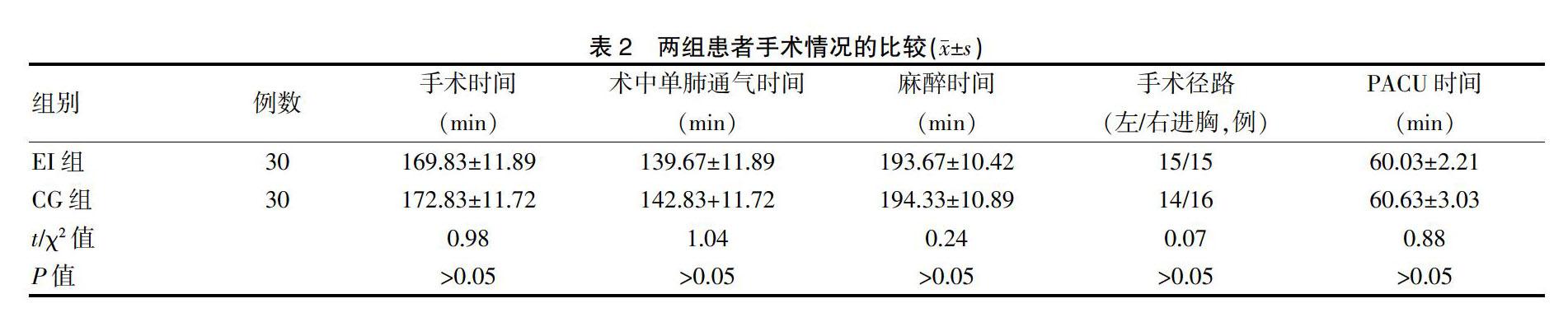
2.1两组患者手术情况的比较
兩组患者的手术时间、术中单肺通气时间、麻醉时间、手术径路、PACU时间比较,差异无统计学意义(P>0.05)(表2)。
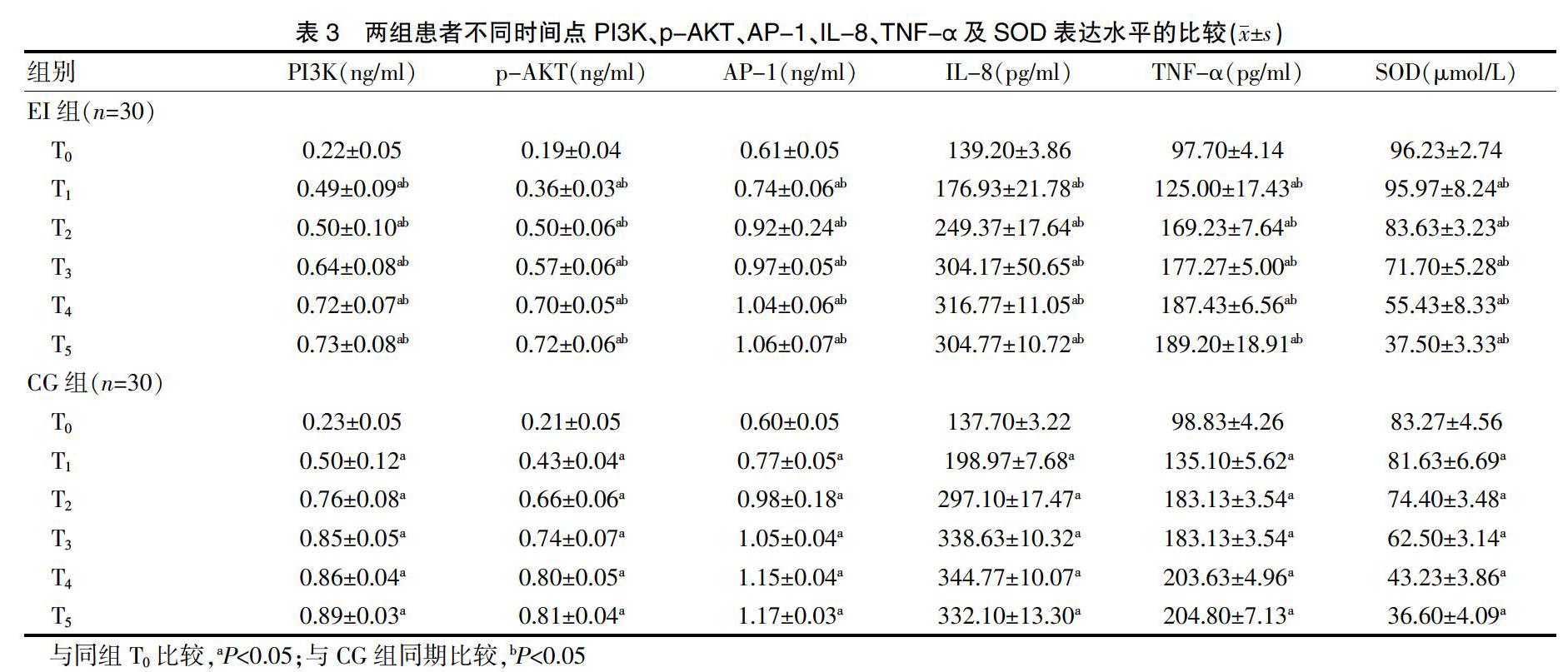
2.2两组患者不同时间点PI3K、p-AKT、AP-1、IL-8、TNF-α及SOD表达水平的比较
两组患者T0时的PI3K、p-AKT、AP-1、IL-8、TNF-α及SOD表达水平比较,差异无统计学意义(P>0.05);两组患者T1~T5时血浆中的PI3K、p-AKT、AP-1、IL-8及TNF-α表达水平均高于T0,差异有统计学意义(P<0.05);两组患者T1~T5时血浆中的SOD表达水平低于T0时,差异有统计学意义(P<0.05);EI组患者T1~T5时血浆中的PI3K、p-AKT、AP-1、IL-8及TNF-α表达水平均低于CG组,差异有统计学意义(P<0.05);EI组患者T1~T5时血浆中的SOD表达水平高于CG组,差异有统计学意义(P<0.05)(表3)。
3讨论
食管癌根治术中,长时间单肺通气可激发体内氧化应激反应,引起促炎及抗炎因子的失衡,影响手术预后[1-2,6]。TNF-α是临床检测炎性反应的主要指标之一[7-9]。已有研究表明IL-8和TNF-α在肺损伤中表达上调,参与急性肺损伤过程[9-10]。SOD是衡量机体氧化应激损伤程度的指标[11-12]。在本研究中随着手术操作及单肺通气实施,患者的IL-8、TNF-α升高及SOD降低(P<0.05),提示炎性反应、氧化应激反应与单肺通气性肺损伤存在着直接关系。
研究表明,依达拉奉能明显抑制细胞内脂质过氧化反应[4]。本研究结果显示,与CG组相比,依达拉奉的使用减少了患者IL-8、TNF-α以及SOD的变化幅度(P<0.05),推测依达拉奉可以降低单肺通气时机体炎性反应,有助于改善手术预后。
P13K/AKT信号通路是生物信号引起核反应的重要通路,对氧化应激及炎性反应的过程起重要调控作用[5,13-14]。AP-1是P13K/AKT信号通路的主要下游因子,对炎细胞的增殖与分化意义重大[15]。本研究结果显示,随着单肺通气的实施,患者PI3K及p-AKT、AP-1的表达水平增加,而经过依达拉奉处理后,PI3K与p-AKT的表达水平的升高幅度均较CG组显著降低,同时AP-1的表达水平的升高幅度均较CG组显著降低(P<0.05)。提示依达拉奉可能是通过调节PI3K/p-AKT从而抑制了AP-1的表达来,进而减少过多氧自由基及促炎性细胞因子的产生,从而抑制过度氧化应激及炎性反应,减轻了单肺通气性肺损伤。
综上所诉,依达拉奉可能通过活化PI3K/p-AKT/AP-1信号转导通路,直接抑制氧自由基、抑制炎症级联反应,减轻了单肺通气引起的肺损伤。
[参考文献]
[1]沈启英,陶洪霞,宗志军,等.长时间单肺通气患者非通气侧肺损伤时巨噬细胞状态的变化[J].中华麻醉学杂志,2017, 37(1):39-42.
[2]García-de-la-Asunción J,García-Del-Olmo E,Galan G,et al.Glutathione oxidation correlates with one-lung ventilation time and PO2/FiO2 ratio during pulmonary lobectomy[J].Redox Rep,2016,21(5):219-226.
[3]Biswas S,Hwang JW,Kirkham PA,et al.Pharmacological and dietary antioxidant therapies for chronic obstructive pulmonary disease[J].Curr Med Chem,2013,20(12):1496-1530.
[4]张自豪,裴凌.依达拉奉对脓毒症大鼠血脑屏障通透性的影响[J].中华麻醉学杂志,2013,33(8):986-988.
[5]Zhang W,Zhang JQ,Meng FM,et al.Dexmedetomidine protects against lung ischemia-reperfusion injury by the PI3K/Akt/HIF-1α signaling pathway[J].J Anesth,2016,30(5):826-833.
[6]Li C,Xu M,Wu Y,et al.Limb remote ischemic preconditioning attenuates lung injury after pulmonary resection under propofol-remifentanil anesthesia:a randomized controlled study[J].Anesthesiology,2014,121(2):249-259.
[7]邓娟,李亚春,朱涛.右美托咪定对脂多糖诱导的脓毒症大鼠全身炎症反应和肺损伤的影响[J].临床麻醉学杂志,2017,33(9):899-903.
[8]帅训军,艾登斌,张海荣,等.依达拉奉对肺叶切除术肺癌患者围术期炎性细胞因子和自由基的影响[J].山东医药,2009,49(43):56-57.
[9]Casanova J,Garutti I,Simon C,et al.The effects of anesthetic preconditioning with sevoflurane in an experimental lung autotransplant model in pigs[J].Anesth Analg,2011,113(4):742-748.
[10]Casanova J,Simon C,Vara E,et al.Sevoflurane anesthetic preconditioning protects the lung endothelial glycocalyx from ischemia reperfusion injury in an experimental lung autotransplant model[J].J Anesth,2016,30(5):755-762.
[11]Erturk E,Topaloglu S,Dohman D,et al.The comparison of the effects of sevoflurane inhalation anesthesia and intravenous propofol anesthesia on oxidative stress in one lung ventilation[J].Biomed Res Int,2014,2014:360 936.
[12]Nair U,Bartsch H,Nair J.Lipid peroxidation-induced DNA damage in cancer-prone inflammatory diseases:a review of published adduct types and levels in humans[J].Free Radic Biol Med,2007,43(8):1109-1120.
[13]Wang D,Zhang X,Li D,et al.Kaempferide protects against myocardial ischemia/reperfusion injury through activation of the PI3K/Akt/GSK-3β pathway[J].Mediators Inflamm,2017, 2017:5 278 218.
[14]Zhang Y,Li D,Luo J,et al.Pharmacological postconditioning with sevoflurane activates PI3K/AKT signaling and attenuates cardiopulmonary bypass-induced lung injury in dog[J].Life Sci,2017,173:68-72.
[15]Lee CY,Huang CY,Chen MY,et al.IL-8 increases integrin expression and cell motility in human chondrosarcoma cells[J].J Cell Biochem,2011,112(9):2549-2557.
(收稿日期:2019-08-09 本文編辑:任秀兰)
猜你喜欢
中国当代医药(2016年29期)2017-01-03
中国实用医药(2016年23期)2016-12-26
中国实用医药(2016年29期)2016-12-26
中国实用医药(2016年27期)2016-11-30
中国实用医药(2016年26期)2016-11-07
中国实用医药(2016年25期)2016-11-03
中国实用医药(2016年21期)2016-08-19
中国实用医药(2016年21期)2016-08-19
中国实用医药(2016年21期)2016-08-19
中国实用医药(2016年22期)2016-08-19