
Physical Therapy Modalities of Western Medicine and Traditional Chinese Medicine for Meibomian Gland Dysfunction
2020-12-31 08:13LIJieOUShangKunLIWeiLIUZuGuoPENGQingHua
Digital Chinese Medicine 2020年4期
关键词:银海
LI Jie,OU Shang-Kun,LI Wei,LIU Zu-Guo,e*,PENG Qing-Hua*
a.Hunan Provincial Key Laboratory for Prevention and Treatment of Ophthalmology and Otolaryngology Diseases with Chinese Medicine,Changsha,Hunan 410208,China
b.Department of Ophthalmology,the First Hospital of Hunan University of Chinese Medicine,Changsha,Hunan 410007,China
c.Fujian Provincial Key Laboratory of Ophthalmology and Visual Science,Eye Institute of Xiamen University,School of Medicine,Xiamen University,Xiamen,Fujian 361102,China
d.Xiamen Eye Center of Xiamen University,Xiamen,Fujian 361001,China
e.Department of Ophthalmology,The First Affiliated Hospital of University of South China,Hengyang,Hunan 421001,China
ABSTRACT The meibomian gland is a unique sebaceous gland located in the eyelid.Its main function is to secrete lipids and form the lipid layer of the tear film to delay the evaporation of waterborne tears,increase the surface tension of the tear film,and to lubricate the contact area of the eyelid and eyeball.Abnormal secretion of the meibomian gland is known as meibomian gland dysfunction(MGD),which has become the most important cause of evaporative dry eye disease (DED).The clinical pathophysiological process and underlying molecular mechanisms of MGD are not clear.As serious side effects may occur with the long-term use of hormonotherapy and non-steroidal anti-inflammatory drugs (NSAIDs) for the treatment of MGD,meibomian gland physiotherapy is considered the most effective and safest therapy for MGD.This review summarizes the physical therapy modalities of western medicine (WM) and traditiond Chinese medicine (TCM) for the treatment of MGD to provide optimal treatments for these patients and to further lay a foundation for mechanistic studies of MGD.
Keywords Meibomian gland dysfunction (MGD)Dry eye disease Eyelid hygiene LipiFlow Intense pulse light (IPL)Acupuncture Eye fumigation Moxibustion
1 Introduction
Meibomian gland dysfunction (MGD) is one of the most common diseases in ophthalmic practice.It is a prevalent disorder:the estimated pooled prevalence is 35.8%,with a higher prevalence of 46.2% - 69.3% in Asia and more than 80.0% of patients with dry eye disease (DED) having MGD in the United States and Europe[1,2].MGD occurrence increases with age,sleep disorders,contact lens wear and androgen deficiency[3].In 2011,the International Workshop on MGD defined the condition as a chronic,diffuse abnormality of the meibomian gland,commonly characterized by terminal duct obstruction and/or qualitative or quantitative changes in the glandular secretion.These changes lead to alterations in the tear film lipid layer,with increased tear evaporation and osmolarity,symptoms of eye irritation,visual disturbance,clinically apparent inflammation and ocular surface diseases[4].It is well accepted that MGD is the most common cause of evaporative DED[5].
Traditional Chinese medicine (TCM) ophthalmology has no corresponding disease named for MGD.Some descriptions of the ophthalmological diseases recorded in ancient books of TCM are similar to most of the symptoms and signs of MGD,such as “wind edge rotten eyes” in theEye Collection of Standards of Diagnosis and Treatment,“fetid wind red rot” or“wind string red-eye” inEssentials from the Silver Sea(Yin Hai Jing Wei,《银海精微》),and the relevant records of “white astringency” inA Close Examination of the Precious Classic(Shen Shi Yao Han,《审视瑶函》).Modern Chinese medicine study supports the etiology and pathogenesis of MGD as the “blepharitis marginalis” and “white acerbity” inOphthalmology of Traditional Chinese Medicineedited by Professor PENG Qing-Hua[6].
The meibomian gland is sebaceous gland embedded in the tarsal plate of both the superior and inferior eyelids.The specific meibomian gland comprise meiocytes forming the acini that perform lipogenesis and mebium production[7-9].The glandular secretion with the lipid and protein mixture maintains the osmolarity and stability,and prevents evaporation of the tear film[10,11].In the histopathological stage,because of the abnormal composition of mebium and the increase of viscosity,meibomian gland can undergo functional and structural changes,such as hyperkeratinization of the ductal epithelium in the meibomian gland[12,13],leading to MGD.So,the ultimate goal of MGD management is to restore the function and structure of meibomian gland.
Many therapeutics have been proposed to treat MGD,including physiotherapy in western medicine(WM) and traditional Chinese medicine (TCM),artificial lubricants,anti-inflammatory agents,tetracycline,immunosuppressors and lubricant ointments.However,except for physiotherapy in WM and TCM,most of those strategies focus on alleviating symptoms or have severe side effects[14].In contrast,physiotherapy focuses on restoring meibomian gland function and structure and has become one of the major forms of therapy (Figure1A).This review summarized and evaluated the current studies on the physical therapy modalities in WM and TCM on MGD (Figure1B).
2 Physical Therapy Modalities for MGD in WM
The physical therapy modality in WM for MGD is a kind of non-pharmaceutical therapy.This includes a broad range of treatments,from low-tech solutions like eyelid hygiene,artificial eyelid warming and massage to high-tech solutions like automated eyelid warming and massage (LipiFlow®System),optimal pulsed light (OPT) therapy,intense pulsed light (IPL)therapy,etc.Each modality has special characteristics (Table1),which are summarized below.
2.1 Eyelid hygiene
Eyelid hygiene plays an important role in decreasing the load of lipolytic bacteria and the amount of potentially toxic lipids on the ocular surface in products to induce tear film spoilage (e.g.,free fatty acids),has become the first choice for the management of MGD and is still highly recommended[34].Tear-free baby shampoos such as Johnson’s®No More Tears,combined with warm compresses,have become the customary treatment for MGD.A variety of lid scrubs are also commercially available and are effective for managing DED.However,an optimal cleaning solution is required as the above solutions contain amidoamine,3-(dimethylamino) propylamine (MAPA),which is highly related to contact and eyelid dermatitis[35].
New products have been developed that contain substances that are anti-inflammatory,bactericidal and moisturizing.Several studies investigated advanced administration of eyelid hygiene,such as eyelid margin cleansing with ofloxacin ointment[36],eyelid hygiene treatment following cataract surgery[15],daily routine use of tap water and/or lid hygiene shampoo to cleanse the eyelid margin[16]in patients with MGD,and reported significantly improved in symptoms and signs.
2.2 Eyelid warming and massage
Eyelid warming and massage remain the mainstay and most effective treatments for MGD nowadays.The application of warmth and massage to the eyelid margin can melt meibum plugging the terminal ducts and gland orifices and facilitate the delivery of meibum from the gland to the tear film[37].Several commercial devices,such as the thermodynamic treatment device,MGDRx EyeBag and wet chamber warming goggles have been developed to retain heat more effectively[38,39].Repeated eyelid warming with a non-wet device can improve TBUT in normal individuals and also has beneficial effects on signs and symptoms of MGD[20,21].
Various automated mechanical devices for eyelid massage have recently been developed based on conventional manual methods.One of them is the LipiFlow System™,which was approved by the Food and Drug Administration (FDA) as an automated alternative for liquefying meibum by thermal compression[22-24].Another similar treatment is vectored thermal pulsation (VTP) therapy,which was designed to simultaneously evacuate the gland contents while heating the glands to therapeutic levels[25-27].VTP can be applied to just the outer eyelids using an inflatable air bladder;while the LipiFlow can apply heat to both the inner and outer eyelid surfaces.Other reported mechanical devices include the fingers or auxiliary instruments such as meibomian gland squeezers,glass rods and local applications of medical apparatuses to evacuate stagnant meibum and improve meibomian gland function[40].
Several studies have indicated that eyelid warming and massage could improve symptoms and signs without serious adverse events in patients with MGD[22-27].Besides,eyelid warming and massage combined with optimal antibacterial honey are effective adjunctive therapies for MGD[40,41].The effectiveness of meibomian gland massage combined with topical levofloxacin against ocular surface flora in patients before penetrating ocular surgery has been reported[42].However,patients often feel discomfort such as mild pain during eyelid massage;with the pain more apparent during the first session compared to the following sessions.Conjunctival congestion and punctate hemorrhages of the lid margin may occur after eyelid massage[40].Therefore,it is important to utilize reliable methods to provide optimal force during the procedure.
2.3 IPL and optimal pulse technology
IPL is a broad-spectrum,non-coherent and polychromatic light source with a wavelength spectrum of 500 -1 200 nm produced by a high-output xenon lamp that can be filtered to allow the emission of a specific range of wavelengths[43].IPL was optimized to allow a single light source (blue light) or blue light + IPL,termed optimal pulse technology (OPT),without increased adverse events.A growing number of physicians worldwide use IPL/OPT for the treatment of MGD and have reported improvements insymptoms,lipid layer grade,and meibomian gland secretion quality and productivity on the day after IPL therapy compared to those at baseline[44-46].ALBIETZ et al.[44]reported that a combination of IPL and meibomian gland expression significantly improved dry eye symptoms and meibomian gland function.YIN et al.[47]compared the results of IPL therapy and eyelid hygiene,reported that both were equally effective in improving symptoms and meibomian gland function.Other studies indicated that IPL therapy was a safe therapy for long-term and regular use for MGD[29].
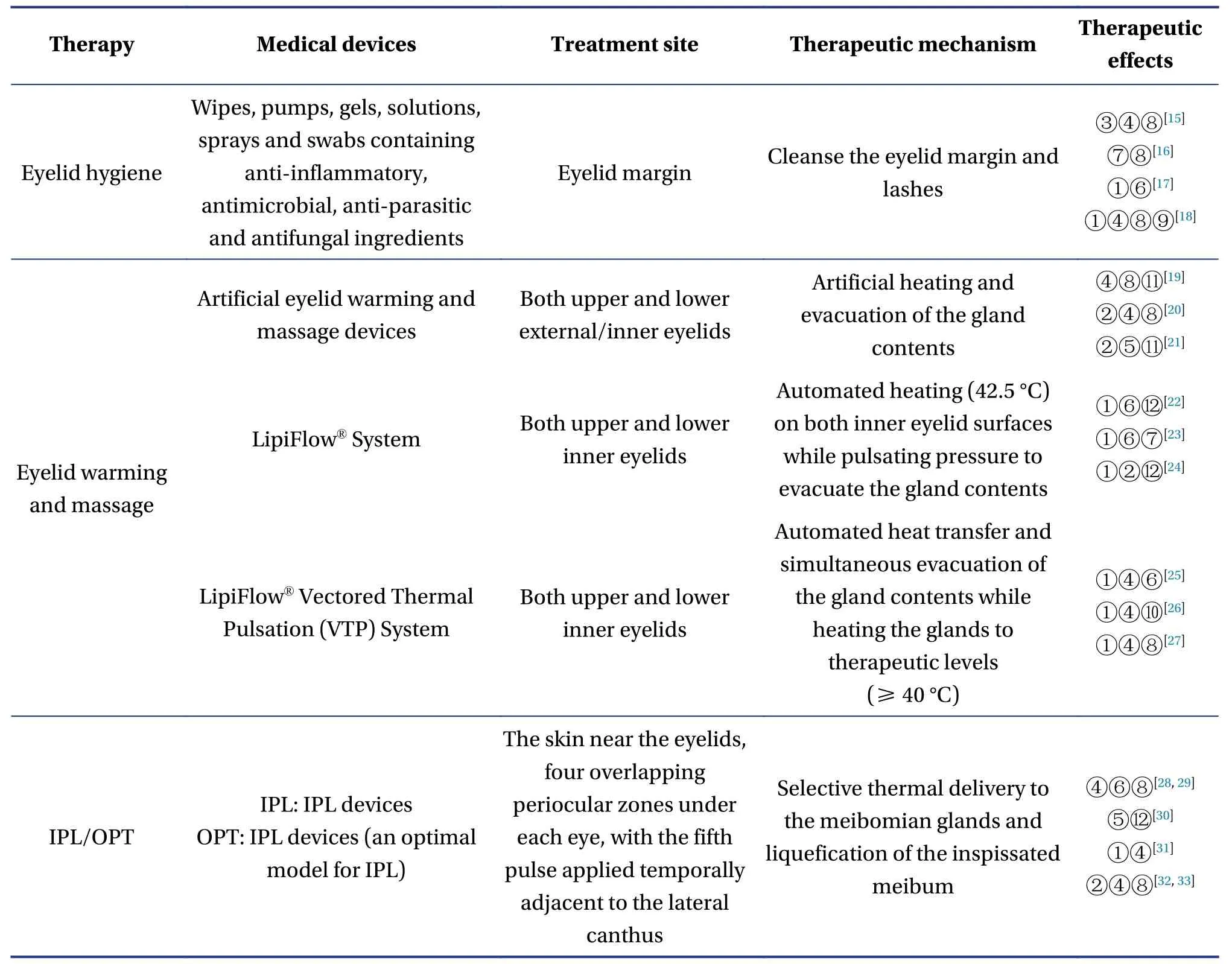
Table1 Characteristics of physical therapy modalities in WM for MGD
The mechanism by which IPL/OPT provides therapeutic effects to improve signs and symptoms on MGD remains vague.The proposed mechanisms include heat transfer,thrombosis of the vasculature around the meibomian gland,and decreased levels of inflammatory cytokines in the tears[48].First some hypotheses propose that the heat produced by IPL/OPT could melt pathologically dysfunctional secretions and improve the obstructive orifices of the meibomian gland.Second,IPL/OPT significantly reduces levels of inflammatory cytokines such as interleukin (IL)-17A,IL-6 and prostaglandin E2 (PGE2),which are highly related to the clinical symptoms of DED induced by MGD.Third,IPL/OPT treatment can immediately reduce bacteria and mite load on the eyelid margin and their associated inflammation[49,50].However,the mechanism requires to be elucidated in future studies.
2.4 Other physicotherapeutics of WM for MGD
Other physical treatments in WM also have been reported for the treatment of MGD.Meibomian gland probing was proven to be a safe and effective method to relieve meibomian gland obstruction with symptom relief and tear film stabilization in patients with MGD[51,52].Wearing moisture chamber spectacles is a safe and promising alternative management for DED and MGD by improving ocular discomfort and tear film stability[53].Three-dimensional (3D) printed personalized moisture chamber spectacles were an effective method to provide sufficiently high periocular humidity in a low-humidity environment in patients with MGD[54].
3 Physical Therapy Modalities in TCM for MGD
Physical therapy in TCM for MGD is based on the TCM syndrome differentiation,including the windheat attack of the exterior,damp-heat of the spleen and stomach,spleen and kidney yin deficiency,phlegm-damp obstruction of the eyelids,and Qi deficiencies of the spleen and stomach.Physical therapy is also called external therapy in TCM.The external treatment for MGD mainly includes acupuncture,eye fumigation and moxibustion MB.Different TCM syndrome differentiation in MGD use different external treatments according to its characteristics (Table2).

Table2 Characteristics of the physical therapy modalities in TCM for MGD
3.1 Acupuncture
Acupuncture therapy is a promising strategy that promotes meridian circulation and regulates Qi and blood in patients with MGD patients.Acupuncture has been applied to select acupuncture sites for different syndromes in patients with MGD[60,61].The acupuncture points usually selected included Jing Ming (BL1),Cuan Zhu (BL2),Yang Bai (GB14),Si Zhu Kong (TE23),Tai Yang (EX-HN5),Si Bai (ST2),He Gu(LI4),Tai Chong (LR3),Guang Ming (GB37),San Yin Jiao (SP6),Feng Chi (GB20) and others.The reported course of treatment was three times a week for four weeks[55,62-64].
Acupuncture shows effects by alleviating symptoms,increasing tear production,and improving TBUT and lipid deficiency in MGD patients.Several studies have observed the clinical effectiveness of acupuncture in the treatment of MGD,in which acupuncture applied at the periocular points was better at improving the palpebral margin score and increasing tear secretion,indicating a better therapeutic efficacy compared to WM[65,66].
The potential molecular mechanisms of acupuncture may include the inhibition of the pro-inflammatory activities of interleukin-6 (IL-6),tumor necrosis factor (TNF)-α,and transfer growth factor (TGF)-β1 as well as increased lactoferrin level in tears to provide a bacteriostatic effect,thereby inhibiting inflammation of the ocular surface[67].Additionally,acupuncture promotes the synthesis and secretion of mucins by goblet cells and the meibomian gland,increases the mucin content in tears,and restores tear film stability to restore the normal structure and function of the ocular surface[68,69].
3.2 Eye fumigation
Eye fumigation therapy is believed to show effects by spreading the external evil,nourishing Yin and glory,dredging the meridians and collaterals,and improving unobstructed Qi and blood[70].eye fumigation uses a medicine decoction to fumigate the eyes with its hot air transpiration.It has the dual effect of physical wet and hot compress and drug treatment.Reported studies applied eye fumigation for approximately 15 min each session,1 - 3 times daily[71,72].
In practice,eye fumigation usually uses fumigation or a fumigation combined with a washing.Clinically,a medicine tank with liquid is removed from the stove and the jar is then immediately covered with a thick sheet of paper or a thick paper cover with holes so that the hot air can fumigate the eyes.The temperature should be hot enough to endure without scalding as too low a temperature cannot achieve the purpose of eye fumigation.The liquid can be reheated.Studies in MGD patients have also reportedly used a heated steam kettle or an ultrasonic atomization inhaler for eye fumigation[70].
Several studies have reported the effectiveness of the combination of massage and eye fumigation on MGD.They believed that the clinical symptoms and signs in MGD patients were related to their cervical spondylosis,which caused increased pressure on the blood vessels and nerves,which affected tear circulation and quality to induce MGD.Thus,the combination of massage and eye fumigation could improve eye nutrition,promote tear secretion,and have a cleaning effect by clearing heat and providing detoxification[70,73-75].
3.3 Moxibustion
Moxibustion therapy dredges the meridian,harmonizes the Qi and blood,activates blood circulation and removes blood stasis,and eliminates inflammation and analgesia.Each course of treatment requires a daily Moxibustion session lasting approximately 30 min for 15 d for a total of two courses.After Moxibustion treatment,the symptoms,corneal fluorescence staining and TBUT are reportedly significantly improved;moreover,the operation was simple and easily accepted by children[76,77].
Thunder-fire moxibustion has also shown a remarkable curative effect on MGD[78].The combination of thunder-fire moxibustion with TCM improved meibomian gland function by nourishing the Yin on MGD patients[74,79].QIAN et al.[80]also reported that thunder-fire moxibustion with tobramycin dexamethasone eye drops was effective in treating MGD.
3.4 Other physicotherapeutics of TCM for MGD
Other physical treatments of TCM,such as prick and bleeding and cupping,TCM hot package,and acupoint massage,could improve subjective symptoms,eyelid margin score and TBUT on MGD patients.The combination of TCM and acupoint massage reportedly eliminated eye fatigue,with a total effective rate of 93.3%[81].Moreover,the combination of TCM ultrasonic cooling fog and moxibustion was also effective,with a total effective rate of 95.33%[82].
4 Conclusions and Perspective
Physical therapy modalities are recommended and effective treatments for MGD.Physicotherapeutics of WM has been widely used in practice in the past three years,and many high-end clinical products have been developed.Therefore,it is well promoted in clinical practice.Physicotherapeutics of TCM has its advantages,but it is still relatively traditional,with few commercial benefits,and has not been widely promoted.
To enable MGD patients to receive appropriate physical treatment,standardization of MGD diagnosis and treatment is necessary.First,more studies are needed to assess tear film lipid layer thickness and alterations in the morphology and bacterial flora of the meibomian gland and the ocular surface,as well as tear osmolarity after physical treatments.Second,the mechanisms by which these physical strategies affect MGD requires clarification.Third,some modalities are expensive and not available in all clinics and the issue of cost may be a limitation for MGD patients.Last,the physiotherapy of TCM is based on clinical observations and lacks large samples and multi-center tests;therefore,it is necessary to continue to expand the research and strengthen future studies on these mechanisms.
Acknowledgements
We thank for the funding support from the Research and Innovation Project of Graduate Students in Hunan Province (No.CX20190538),the First-class Open Fund for Integrated Chinese and Western Medicine (No.2018ZXYJH05),the Traditional Chinese Medicine First-Class Discipline Open Fund(No.2018ZYX57),and the Construction Project of Hunan Engineering Technology Research Center for the Prevention and Treatment of Otorhinolaryngologic Diseases and Protection of Visual Function with Chinese Medicine (No.2018YGC02).
Competing Interests
The authors declare no conflict of interest.
猜你喜欢
Chinese Physics B(2022年10期)2022-10-26
小天使·四年级语数英综合(2022年4期)2022-04-28
中华魂(2022年3期)2022-03-18
西部(2021年3期)2021-07-11
西部(2021年3期)2021-07-11
滇池(2020年4期)2020-05-18
东坡赤壁诗词(2019年1期)2019-04-30
商周刊(2018年25期)2019-01-08
中外文摘(2016年24期)2016-11-23
中华手工(2014年3期)2014-06-11
 Digital Chinese Medicine2020年4期
Digital Chinese Medicine2020年4期
- Digital Chinese Medicine的其它文章
- Acupuncture and Related Therapies for Hyperlipidemia:A Network Meta-Analysis
- Identification of Potential Flavonoid Inhibitors of the SARS-CoV-2 Main Protease 6YNQ:A Molecular Docking Study
- Network Biological Modeling:A Novel Approach to Interpret the Traditional Chinese Medicine Theory of Exterior-Interior Correlation Between the Lung and Large Intestine
- Fabrication of A Folic Acid-Modified Arsenic Trioxide Prodrug Liposome and Assessment of its Anti-Hepatocellular Carcinoma Activity
- Silkworm Extract Ameliorates Type 2 Diabetes Mellitus and Protects Pancreatic β-cell Functions in Rats
- Inflammatory Mechanism of Total Flavonoids of Chrysanthemum and Medicated Serum on Castrated Dry Eye Animal and Cell Models