Analysis of the characteristics of electronic equipment usage distance for common users
2021-09-15 03:24FernandoSoler1AlicianchezGarcAinhoaMolinaMartDoloresdeFezValentaz1DavidPiero
国际眼科杂志 2021年9期
Fernando Soler1,2, Alicia Sánchez-García, Ainhoa Molina-Martín, Dolores de Fez, Valentín Díaz1,2, David P Piero
Abstract
•KEYWORDS:presbyopia; working distance; mobile phone usage distance; electronic device
INTRODUCTION
The analysis of visual requirements or demands is crucial when prescribing any type of optical aid, especially for the correction of presbyopia[1]. Likewise, near visual tasks have been also demonstrated to be a critical factor in the development of myopia[2]. Myopic children have shown to spend more time on average each day on activities at less than 20 cm than non-myopic children[3]. In another study conducted in 6 152 Spanish children aged from 5-7 years, a total of 43.3% of the participants spent more than 3h a day doing near activities, with 48.9% of them spending more than 50% of this time using electronic devices[4]. On the other hand, the extended use of smartphones has shown to have important implications for ocular surface health and binocular function[5]. However, very few studies have tried to characterize the working distance (WD) in the population more susceptible to all these visual and ocular problems as well as the distance of use of the mobile phone usage distance (MPUD), one of the most common daily activities in the general population[1,6-9].
Concerning presbyopia correction, a careful evaluation of visual demands is necessary to select the most adequate design for the optical aid in order to achieve a functional vision[1,10]. Presbyopic contact lens and spectacle corrections as well as the implantation of multifocal or extended depth of focus intraocular lenses (IOLs) have shown to have a significant impact on WD which may be optimized to satisfy the patient’s visual requirements[11-17]. Giletal[18]concluded in a comparative study of four different multifocal IOLs that their characteristics evaluated in terms of optics, profile, and add power may contribute to help surgeons decide on the type of IOL most suitable for each patient, especially those with high visual demands at near and intermediate distances. Therefore, not all presbyopia-correcting optical aids are optimal for covering the visual demands of each specific patient[19-20]. The aim of the current study was to analyze and characterize the pattern of visual WD and MPUD in a large population with significant demands at near using electronic devices, analyzing the differences in these parameters according to different aspects such as job profile.
SUBJECTS AND METHODS
PatientsThis study was a transversal study resulting from a screening campaign evaluating the visual status of professionals working with computers or electronic devices more than 2h per day. This screening campaign was promoted and developed by Dr Soler Foundation (Elche, Alicante, Spain). A total of 100 patients were revised with a mean age of 41.2 years, ranging from 20-62 years. Inclusion criteria were patients with an age between 20-65 years and reporting a daily use of more than 2h of computer or electronic devices. Exclusion criteria included any active ocular disease, previous ocular surgery including laser refractive surgery, limited vision (corrected distance visual acuity of 20/60 or below), neurologic problems, strabismus, and amblyopia. All patients were adequately informed about the study and signed a consent form prior to their inclusion. The study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the University of Alicante (Exp UA-2018-12-16).
ClinicalProcedureA battery of screening tests was performed to all participants in a single session at the working environment of each of them. This means that measurements were performed directly at the institutions where participants were working, not at any clinical setting or clinic. Therefore, this screening study was not conducted in a controlled clinical environment as the aim of the study was to measure how the patient works in its real daily position, not in artificial conditions. All measurements were performed by the same three experienced examiners (AMM, ASG and DPLL).
The screening session included the following measurements and tests performed in the following sequential order: 1) Self-developed questionnaire asking about the medical history of patients and determining their eligibility for the study; 2) Measurement of the main WD according to the job or position of patients (from the spectacle plane) and their arm length with a calibrated ruler; 3) Measurement of distance (4 m) LogMAR visual acuity and stereopsis (40 cm) of patients with their actual correction (glasses, contact lenses, no correction) using a calibrated tablet Euvision Tab (Euvision Ltd., Pécs, Hungary)[21]. This tablet has been validated for screening of different visual conditions[21]; 4) Measurement of near (40 cm) visual acuity of patients with their actual correction (glasses, contact lenses, no correction) using LogMAR chart; 5) Evaluation of the ocular alignment by means of the cover test at distance and near with correction; 6) Measurement of the near point of convergence using the push-up technique; 7) Measurement of the MPUD (face-device distance) with the VisionApp (VisionApp Solutions S.L.,guilas, Murcia) while the patient was reading the general menu of the main screen of the mobile phone device. This App identifies the range of distance when using the mobile hand-held device and has been validated for such purpose[22]. This App was installed in one mobile phone that was specifically used for the screening campaign. High accurate MPUD values were measured at 0.1 Hz during a minimum time of 1min[22]. The main outcome measures of this study were WD and MPUD. As described previously, other variables were evaluated that were considered as secondary.
StatisticalAnalysisStatistical analyses were performed with a commercially available software package (SPSS for Mac, Version 20.0; IBM Corporation, Armonk, NY, USA). Kolmogorov-Smirnov test was used to assess the normality of the data distributions analysed. Measured variables were characterized with the following parameters: average, standard deviation, median and range. The correlation of WD and MPUD with the rest of variables evaluated was analysed with the Pearson coefficient for samples normally distributed and the Spearman coefficient for those not normally distributed. The paired Studentt-test was used for the comparison of the different distances measured in each subject of the study,whereas the unpaired Studentt-test was used for the comparison between independent groups (male-female, exo-eso). Finally, a one-way analysis of variance (ANOVA) was performed to assess the statistical significance of differences in WD and MPUD between job groups, using the Bonferroni test for post-hoc analysis. For all statistical tests, aP-value below 0.05 was considered as statistically significant.
在这里(x,y)表示发送节点,(xi,yi)一跳邻居节点.那么节点间的相对位移可以利用以下公式来得到:
RESULTS
A total of 200 eyes of 100 patients with mean age of 41.2 years (SD: 10.48, median: 41.0, range: 20-62 years) were evaluated. The sample was comprised of 55 males (55.0%) and 45 females (45.0%). During the screening, a total of 19 (10.0%) and 52 patients (24.0%) wore contact lenses and glasses, respectively. Table 1 summarizes the main outcomes obtained in the sample screened. As shown, the WD was significantly longer than the MPUD (P<0.001). Likewise, the arm length was significantly higher than the measurement of WD and MPUD (P<0.001).
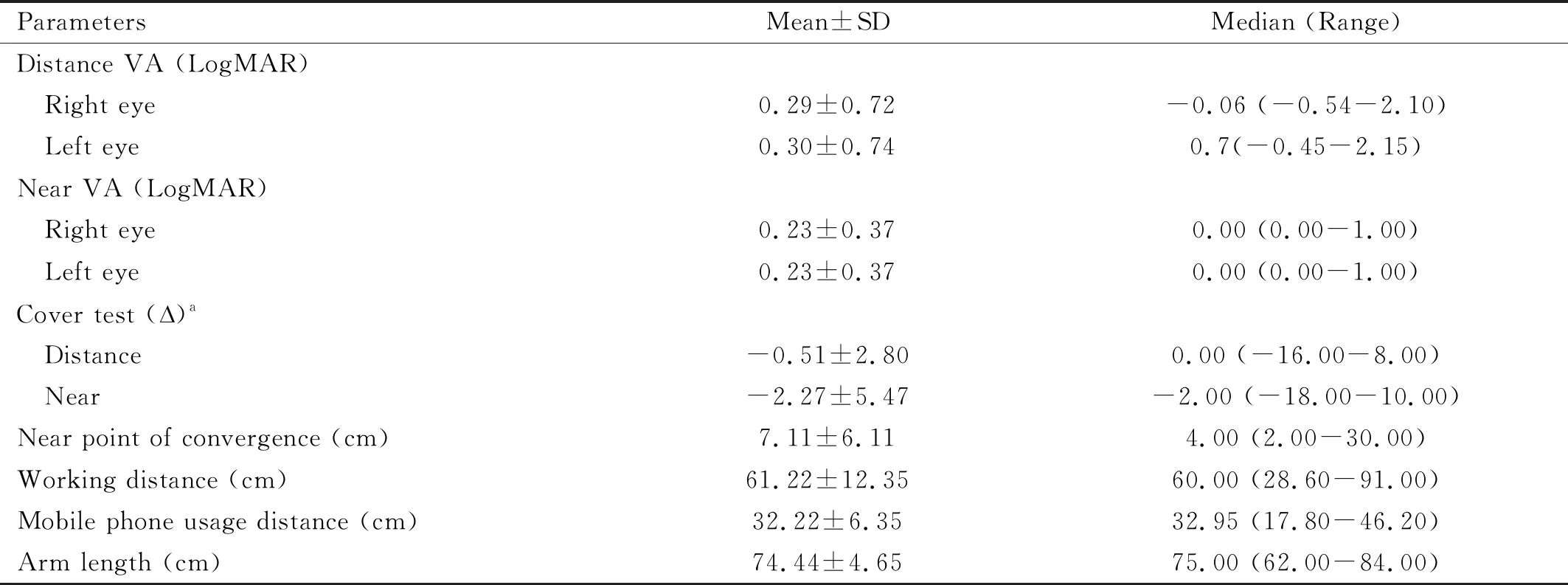
Table 1 Summary of the main outcomes obtained in the sample of patients screened
RelationshipBetweenWorkingandMobilePhoneUsageDistanceFigure 1 shows the distribution of the WD and MPUD measured in the evaluated sample. As shown, a great variability in the relationship between both distances was present. A total of 4% (4) and 91% (91) of patients had a WD and MPUD of 40 cm or below, respectively. Likewise, a total of 68% (68) and 100% (100) of patients had a WD and MPUD of 66 cm or below, respectively. A weak although statistically significant correlation was found between WD and MPUD (r=0.387,P<0.001) (Figure 2). Likewise, a weak but statistically significant correlation of WD with arm length was found (r=0.260,P=0.009). However, no significant correlation was found between arm length and MPUD (r=0.109,P=0.279). Furthermore, no statistically significant correlations of the near point of convergence with WD (r=-0.028,P=0.784) and MPUD (r=0.129,P=0.199) were found.
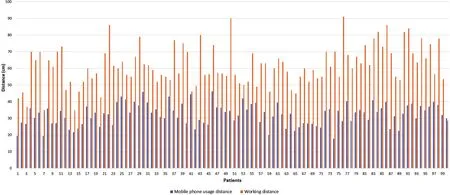
Figure 1 Distribution of the working (orange bars) and mobile phone usage distances (blue bars) measured in the evaluated sample.
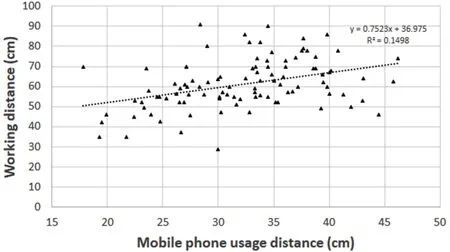
Figure 2 Scatterplot showing the relationship between the distance of the mobile phone usage distance and the working distance in the sample of eyes evaluated. The adjusting line to the data obtained by means of the least-squares fit is shown.
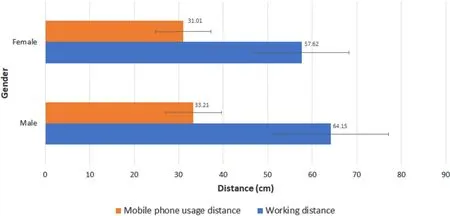
Figure 3 Mean working (orange bars) and mobile phone usage distance (blue bars) according to age in the sample of patients evaluated.
RelationshipofWorkingandMobilePhoneUsageDistancewithClinicalVariablesWeak but statistically significant correlations of distance (right eye:r=0.356,P<0.001; left eye:r=0.344,P<0.001) and near visual acuities (right and left eyes:r=0.386,P<0.001) with WD were found. In contrast, no significant correlations of MPUD with visual acuities were found (0.105≤r≤0.140,P≥0.165). Likewise, poor and no significant correlations of WD and MPUD with stereopsis and distance and near phoria measurements were found (-0.083≤r≤0.145,P≥0.150). Furthermore, age was found to be significantly correlated with both WD (r=0.255,P=0.011) and MPUD (r=0.395,P<0.001).
DifferencesAccordingtoGenderConcerning gender differences, significantly longer WD were found in males compared to females (P=0.008) (Figure 3), confirming that no significant differences were found between subgroups in age and refractive error (P≥0.121). A similar trend was observed for MPUD, but the differences between males and females did not reach statistical significance (P=0.085) (Figure 3). Similarly, a significantly longer arm length (71.59±4.19vs76.79±3.59 cm;P<0.001) was found in females as well as a closer near point of convergence (5.56±4.11vs8.35±7.16 cm;P=0.024).
DifferencesAccordingtotheTypeofPhoriaA total of 13 (13%), 56 (56%), and 31 (31%) patients presented orthophoria, exophoria and esophoria, respectively. No statistically significant differences were found in WD, age, refractive error and gender between patients with exophoria and esophoria (P≥0.071) (Figure 4). Likewise, differences between exophoric and esophoric patients in terms of MPUD did not reach statistical significance (P=0.472) (Figure 4). Furthermore, no significant differences were detected between patients with exophoria and esophoria in near point of convergence (P=0.339) and arm length (P=0.932).
DifferencesAccordingtotheTypeofJobThe distribution of professional jobs of patients enrolled in this study was as follows: 27 administrative staff (27%), 11 executive (11%), 13 militaries (13%), 15 sellers (15%), 11 university researchers or lecturers (11%), 12 health professionals (12%), and 11 other professionals (11%) (Figure 5). Statistically significant differences were detected among job groups in WD (P=0.021), but not in gender, age or refractive error (P≥0.101). Specifically, the WD for the military group was significantly longer than that measured in the group of university researchers and lecturers (P=0.025) (Figure 5). Although the WD was found to be also longer for militaries compared to health professionals (P=0.074) and other professionals (P=0.069), differences did not reach statistical significance (Figure 5). Concerning the MPUD, differences between job groups were in the limit of statistical significance (P=0.047), with a trend to measure shorter distances for health professionals compared to executives (P=0.192). Furthermore, no statistically significant differences between job groups in the measurement of the near point of convergence (P=0.630) and near phoria (P=0.722).
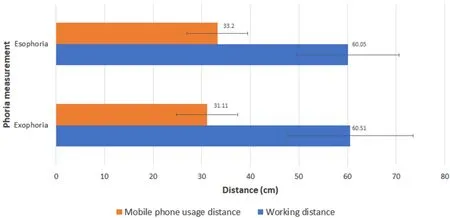
Figure 4 Mean working (orange bars) and mobile phone usage distance (blue bars) according to the type of phoria in the sample of patients evaluated.
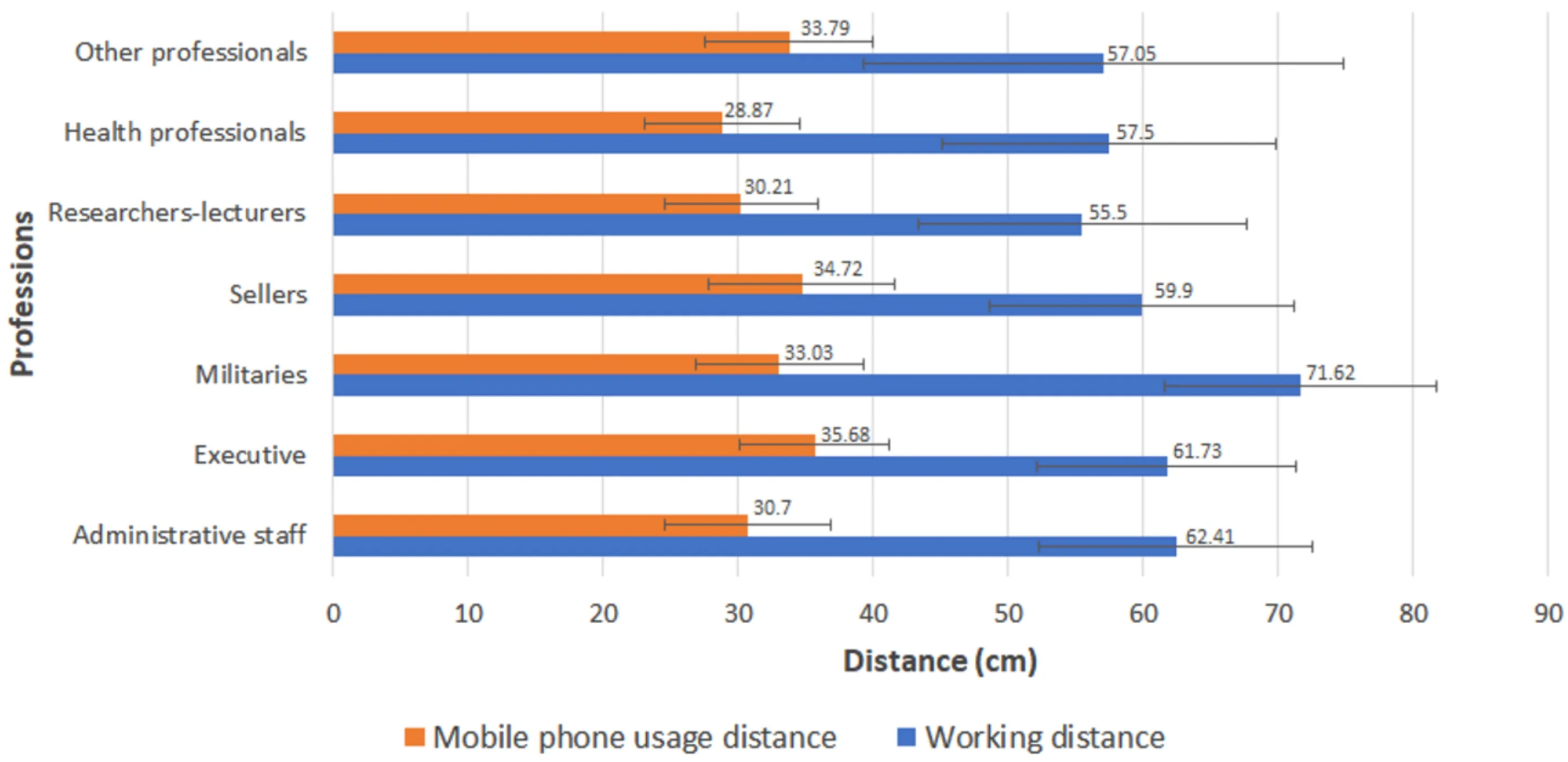
Figure 5 Mean working (orange bars) and mobile phone usage distance (blue bars) according to the type of professions of the patients evaluated.
DISCUSSION
Patient selection is a crucial issue when recommending a specific type of correction, especially in presbyopic subjects[1]. The optical performance of each specific optical aid according to its design should be known and considered by the practitioner before any type of recommendation as the range of tolerable visual quality and foci may vary significantly between different optical corrections[19-20]. Likewise, the visual demands and requirements of the patients should be considered in the attempt of finding the most adequate prescription providing the range of focal distances matching better with the specific range of distances commonly used by patients for performing their daily life activities. Considering that a great part of our lifetime is dedicated to working activities[23]and the use of mobile phones for different purposes[7], and that the visual demands required when performing activities with electronic devices and computers are high[23-25], the aim of the current study was to analyse and characterize the pattern of WD and MPUD in those subjects using electronic devices and computers more than 2h per day.
In our sample, mean WD was 61.22±12.35 cm, ranging from 28.60-91.00 cm. This confirms a great potential variability among individuals in terms of WD despite evaluating people using more than 2h/d computers and electronic devices. A total of 4% (4) and 68% (68) of patients had a WD of 40 and 66 cm or below, respectively. Therefore, the visual acuity in this range of distances should be evaluated when analyzing the effect of any type of optical correction, especially for presbyopia. As recently suggested by a group of experts, the concept of functional vision range should be considered and compared with the range of patient’s visual demands in order to determine the level of matching between both and consequently the adequacy of a presbyopia-correcting intraocular implant[26].
Concerning MPUD, the mean value obtained in the sample evaluated was 32.22±6.35 cm, ranging from 17.80-46.20 cm. A total of 91% (91) and 100% (100) of patients had a MPUD of 40 and 66 cm or below, respectively. This distance was found to be significantly shorter than the WD and this should be also considered when planning a visual rehabilitation with any type of optical correction, especially for presbyopia and hyperopia. Indeed, the visual acuity at around 33 cm should be also evaluated when analyzing the outcomes achieved with any type of presbyopic correction due to the relevance in the presbyopic population of the use of mobile phones. A study conducted in a Spanish population with ages ranging from 16-65 years old found that the mean number of hours of daily use of the mobile phone was 2.8±2.31h, being considered at all age ranges the use of the application WhatsApp (to send and receive text messages and pictures) as irreplaceable (88.5%)[27].
In the current sample, a great variability was observed in the relationship between WD and MPUD among individuals. This means that this relationship cannot be predicted with accuracy. Indeed, a weak although statistically significant positive correlation was found between WD and MPUD. Likewise, the arm length was also found to be a poor predictor of WD, with only a weak although statistically significant correlation between these two parameters. Concerning MPUD, it was not correlated with the arm length. Therefore, the specific measurement of WD and MPUD should be performed in the preoperative exam for defining the prescription of any type of optical aid to detect the real patient’s visual demands and to find the optical correction providing the foci covering such demands. In the field of cataract surgery, the development of a multifocal IOL based on an optic design providing a continuous range of vision between approximately 25 and 90 cm as well as a distance focus seems to be an optimal approach, as it would cover the demands in terms of WD and MPUD of common users of computers and electronic devices. Future studies should investigate this further in order to optimize the selection of presbyopia-correcting IOLs in cataract and clear lens surgery.
The level of correlation of WD and MPUD with different clinical variables evaluated was analyzed to investigate the potential of prediction of such distances by other clinical factors. No significant correlations of WD and MPUD with near point of convergence, stereopsis or magnitude of phoria were found. It should be considered that none of patients had relevant binocular anomalies as it was an exclusion criterion for the screening. In contrast, a weak but statistically significant correlation was found between distance and near visual acuities and WD, with longer distances for those individuals with worse visual acuity. This may be explained by several factors, being one of them the patient’s attempt to diminish the accommodative demand when they are presbyopes or undercorrected hyperopes and then having a poorer near visual acuity. It is curious that this correlation was not found with MPUD, which may be in relation with the possibility of using the zoom modality in these devices facilitating the visualization of the text shown in the display, which is something performed by some users[28]. Indeed, age was found to be significantly correlated with both WD and MPUD, with people in the presbyopic age range showing longer WD and MPUD.
Finally, differences in WD and MPUD have been also found according to gender and the type of job. Specifically, the WD was significantly longer for militaries compared to university researchers and lecturers. Other previous studies have reported quite different WD for distinct professional profiles[1,29-31]. Likewise, significantly longer WD were found in males compared to females. As WD has a certain correlation with arm length[1], this finding seems to be mainly related to the significantly longer arm length found in males, which is something that has been previously demonstrated in anthropometric studies[32-34]. Therefore, gender and the patient’s job should be considered when planning most of optical corrections as the visual demands vary significantly with these two factors. In any case, the range of variability of WD and MPUD as a function of age and profession was always within 25 and 90 cm, a range of distances for which most of presbyopic and non-presbyopic corrections should provide an almost constant level of optimized focusing.
In conclusion, working and MPUD vary significantly among common users of computers and digital devices, with no predictable relationship between them. However, MPUD tended to be shorter than WD for most of patients and therefore this parameter should be considered when selecting the most adequate optical prescription for any type of patient, especially for presbyopia.
猜你喜欢
机械工业标准化与质量(2022年6期)2022-08-12
中等数学(2022年2期)2022-06-05
新高考·高二数学(2022年3期)2022-04-29
新高考·高二数学(2022年3期)2022-04-29
中学生数理化(高中版.高二数学)(2020年11期)2020-12-14
装备制造技术(2020年2期)2020-12-14
小学生学习指导(低年级)(2020年6期)2020-07-25
河南科技学院学报(自然科学版)(2020年2期)2020-05-22
小学生学习指导(低年级)(2018年9期)2018-09-26
疯狂英语·新读写(2018年2期)2018-09-07