
Staged lensectomy and vitrectomy in the management of stage 5C retinopathy of prematurity with corneal opacification: long-term follow up
2022-09-14 06:50PingFeiTingYiLiangJiePengYuXuJiaLuoQiZhangJiaKaiLiJiaoLyuPeiQuanZhao
INTRODUCTION
Retinopathy of prematurity (ROP) is an avoidable cause of childhood blindness
. Undergoing screening protocols and meticulous examinations by an experienced ophthalmologist is one of the main approaches that could reduce the burden of this type of blindness
. However, later presentation is significantly associated with more advanced ROP. In developing countries and even in rural areas, quite a few patients are still not referred to ophthalmologists until leukocoria is noticed mainly due to lack of routine screening for ROP
.
The surgical techniques for stage 5 ROP are demanding
.Successful anatomical results after surgery are only seen in 9%-45% of cases and, even with a successful anatomical result, the visual outcome may be limited
. Stage 5 ROP was defined as 3 subcategories, according to the International
Classification of Retinopathy of Prematurity, 3
edition, in terms of their anterior and posterior configurations. Stage 5C, was defined as total retinal detachment of closed-funnel configuration accompanied by anterior segment changes (
,marked anterior chamber shallowing, iridocorneolenticular adhesions, corneal opacification)
. There are several studies about surgical management of stage 5 ROP
. However,there is few studies about the management of stage 5C ROP with corneal opacification, which called for urgent surgery to resolve the complications, but is more challenging to manage due to the invisible fundus
. Whether and how to perform surgeries in these cases remain questionable. Regular combined lensectomy and vitrectomy were not advocated due to the corneal opacity and invisible fundus. Here, we presented a series of cases in which staged lensectomy and vitrectomy were performed. Thereafter, the long-term anatomical and visual outcomes were analyzed.

SUBJECTS AND METHODS
This study was approved by the Ethics Committee of Xinhua Hospital, Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China. All parents of the patients provided informed consent before the surgeries were undertaken. Written informed consent was also obtained from the parents for the enrollment of their children in the study.
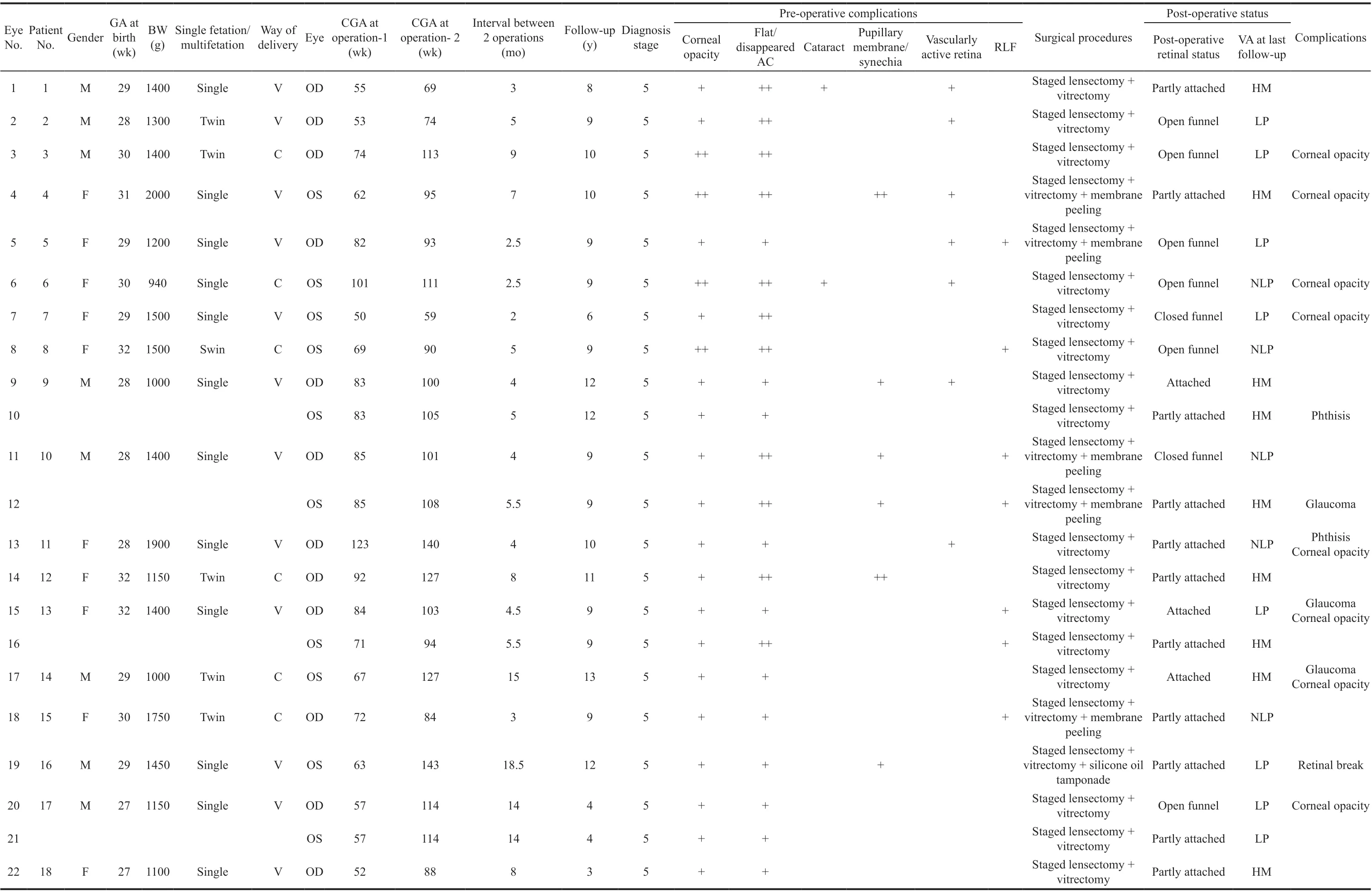
During long-term follow-up after the two procedures, all the patients formed an anterior chamber. Fourteen eyes had clear corneas after surgery, while 8 eyes retained their corneal opacity. Three eyes had secondary glaucoma, which was controlled by medical treatment. Two eyes had ocular phthisis.The retina was reattached in 3 eyes and partially attached in 11 eyes. The retina of the remaining 8 eyes were detached,including 6 open-open or partially open funnel configurations but expanding and 2 closed configuration detachments. Visual acuities ranged from NLP to HM (Table 2). There were no statistical differences between the mean intervals of the staged surgeries among different groups of post-operative retinal status or the final visual acuity. Table 3 presents the demographics and outcomes of staged lensectomy and vitrectomy in individual patients.
Before lensectomy, all 22 eyes had corneal opacity and flat or disappeared anterior chambers. Eighteen eyes had corneal edema and the remaining 4 eyes had corneal nebula. Two eyes had complicated cataract and 7 eyes had retrolental fibroplasia.Six eyes had posterior pupillary synechiae or membranes.Seven (40%) eyes had vascularly active retinas.
现对本文所提出的算法与ML、SD、Rx-SD和Tx-SD检测算法在瑞利衰落信道下的蒙特卡罗仿真结果进行分析,并将所提出的算法的计算复杂度与ML检测和传统的SD检测包括Rx-SD和Tx-SD进行比较.
All patients underwent comprehensive examinations. Preoperative clinical findings, including the patients’ gestational age at birth and surgeries, birth weight, gender, manner of delivery, ROP status, pre- and post-operative status, and treatment were recorded.
以上主要论述了通过回应型法模式实现刑法教义学知识对处罚实质合理性的回应,属于一种宏观的理念介绍和法理论证,如何具体实现这种“回应”,就需要结合犯罪构成体系本身。

We performed staged lensectomy and posterior vitrectomy in all 22 eyes. Lensectomy was performed firstly to avoid further deterioration. Topical steroids were applied to reduce the corneal edema after lensectomy. Vitrectomy was advocated if the corneal edema improved and the fundus was visible during the follow up after lensectomy. All the patients were operated on by one surgeon (Zhao PQ). All the eyes were followed for at least three years post-operatively (average 8.9±2.6y).
In our case series, all the stage 5C ROP cases had flat or disappeared anterior chambers, which indicated an urgent need for lensectomy to avoid permanent corneal damage. However,all the eyes had corneal opacity due to corneal edema or dense corneal nebula, which made it difficult to view the fundus clearly to perform vitrectomy. Additionally, in our case series, 7 eyes had vascularly active retinas. If vitrectomy is performed when the retina is vascularly, severe complications such as vitreous hemorrhage may occur
. Gopal
and Fuchino
suggested that since the disease was more vascularly active in babies less than 6 months of age, operating within 6mo has a marked risk of post-operative hemorrhages.Machemer and DeJuan
and Cusick
reported a higher success rate when babies were operated after six months of age. Anti-angiogenic treatment can possibly be an adjunctive therapy for vascularly active retina
, however, eyes must be monitored closely since intense fibrous contraction with complex retinal detachments can occur
. Staged lensectomy can rescue the cornea in stage 5C ROP and also avoid the risk of post-operative hemorrhages when the retina is vascularly active. The mean interval between the two staged surgeries in our study was 6.8±4.6mo, ranging from 2.5 to 18.5mo, which depended on the status of the corneal opacity and the vascular activity of the retina. Treatment with topical anti-inflammatory drops may be considered after lensectomy to reduce the corneal edema.
Staged lensectomy and vitrectomy(Figure 1).
Primary procedure: lensectomy (Online supplementary Video 1): 1) Apply the two-port limbal approach; 2) Drain the subretinal fluid to soften the eyeball if necessary. Then, inject viscoelastics into the anterior chamber to separate the anterior and posterior iris synechiae. Trim the edge of the iris to enlarge the pupil. 3) Perform lensectomy; 4) Remove the anterior capsule and aspirate the lens material under low suction using the vitrectomy cutter.

The authors also demonstrated that staged lensectomy and vitrectomy for stage 5C ROP with opaque cornea might be beneficial in helping preserve vision. The purpose of the surgeries is to rescue the cornea and even partly attach the retina with less complications
. Surgical intervention may prevent further ocular atrophy, improve the appearance of the eye, and somehow restore visual function (
, perception of light)
, which is very important to the patients with lowvision.
Follow-up examinations were conducted periodically. The anatomical outcomes were evaluated, including retinal status,cornea, and anterior chambers (Figure 3). Visual acuity was measured accordingly, marked as hand motion (HM), light perception (LP), and no light perception (NLP).
RESULTS
The demographics of the patients are presented in Table 1.Twenty-two eyes of 18 stage 5C ROP patients with advanced complications were included in this study. Eight patients were males and 10 were females. Their birth weight ranged from 940 to 2000 g (mean 1363.0±300.0 g). Gestational age (GA) at birth ranged from 27 to 32wk (mean 29.3±1.6wk). The average corrected GA at the time of the first surgery was 73.6±18.0wk(ranging from 50 to 123wk). The average corrected GA at the secondary vitrectomy was 102.4±21.3wk (ranging from 69 to 143wk). The mean interval between the two surgeries was 6.8±4.6mo (2.5-18.5mo).
根据当阳市水域滩涂承载力评价和水产养殖产业发展预测,我们以市场需求为导向,以资源禀赋为基础,按照 “突出重点、有序推进、优化结构、因地制宜、协调发展”的总体要求,规划当阳市养殖水域滩涂开发的总体思路,逐步优化渔业产业区域布局,建立协同发展产业格局。
学生宿舍的条件很差,窗玻璃又不断地被打碎,秋天里,四处漏风,只好糊上报纸,风一吹,呼答答地响起没完没了,尤其在深夜,感觉像睡在押运战俘的列车上。这些没玻璃的窗户只有等到大雪纷飞、北风呼号的日子才能重新镶上。
This study was a retrospective, interventional,consecutive case series. Twenty-two eyes of 18 stage 5C ROP patients with corneal opacification who underwent staged lensectomy and vitrectomy at Xinhua Hospital, Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai,China, from 2008 to 2017 were included in this analysis.
DISCUSSION
In this study, we recommended staged lensectomy and vitrectomy as an alternative choice. Lensectomy was performed first. Then, vitrectomy was recommended if the corneal opacity was alleviated and the fundus was visible during the follow-up period after lensectomy.
在前面确定精选pH值条件下,进行调整剂水玻璃用量试验。试验结果见图9。从试验结果可以看出,当水玻璃用量在200g/t时,精矿产品中铜、钼的回收效果较好,随着用量继续增加,铜、钼逐渐受到抑制。


Closed vitrectomy combined with lensectomy were performed in stage 5 ROP with retrolental fibroplasia or other complications,such as a flat anterior chamber or cataract. Whether surgical intervention is necessary in these cases remains questionable
.When making a surgical decision, controversies still exist regarding when the surgery should be performed and which surgical techniques are the most beneficial for the treatment of stage 5 ROP with advanced complications. Combined vitrectomy and lensectomy are not advocated for stage 5C ROP eyes with invisible fundus due to corneal opacity.
Surgical intervention in ROP has been described as early as 1977 by Treister and Machemer
. Two common surgery approaches used in stage 5 ROP are open-sky vitrectomy and closed vitrectomy
. Open-sky vitrectomy has the advantage of allowing two-hand dissection from a larger anterior incision; however, the maintenance of intraocular pressure(IOP) during surgery may be difficult, and there is a risk of corneal rejection post-operatively after re-suturing the cornea. Due to this, the focus has gradually shifted to closed vitrectomy with or without lensectomy
.
江豚与大熊猫一样憨态可掬,吻部短而阔,看起来就像一直在微笑。2006年,中科院水生生物研究所科考时发现,长江江豚有1800头左右,其中1000多头生活在长江干流。到了2012年,江豚数量锐减至1000头。2013年,世界自然保护联盟红色名录将长江江豚定为“极度濒危”物种。
In our case series, all the patients had normal anterior chambers after surgery. Fourteen out of 22 eyes had clear corneas post-operatively. Secondary glaucoma has been reported to be another complication of ROP
, in our study,3 cases had complicated glaucoma and were under medical control. Fourteen (63.6%) eyes obtained at least partial retinal reattachment after the second procedure, the successful anatomical result was higher than the result (57%) reported in the previous study with 87 eyes by Choi and Yu
.
Second procedure: vitrectomy (Figure 2, Online supplementary Video 2).Vitrectomy was performed when the corneal edema alleviated and did not obscure the view of the retina and/or the retina turned vascularly inactive. 1) Apply the three-port limbal approach; 2) Remove the pre-retinal tissue completely without retinal break formation using 23/25G intraocular forceps and scissors through bimanual dissection under coaxial illumination of the microscope; 3) Inject the viscoelastic solution to achieve retinal reattachment and to maintain the eyeball pressure at the end of the surgery. Use silicone oil tamponade in the surgery if retinal break was present during vitrectomy. 4) Suture the sclerotomies.
作为以汉语为母语的中国,在学习英语的过程中首先要解除48个因素,但是小学阶段学生可能在初次接触这类知识的过程中会产生陌生感。为此,就需要教师能够在日常教学过程中多听多看。以此进一步培养学生形成语感。
印度素食文化直接影响当地旅游业的形式表现为两点,一是传统素食节日;二是全素食城市——帕利塔纳吸引来的旅游人群。
Our study has several limitations. First, it was a retrospective and non-comparative consecutive case series study. Second,the study was based on one surgeon’s experience.
In conclusion, the management of the condition of stage 5C ROP patients with flat anterior chamber and central corneal opacity is challenging. Staged lensectomy and posterior vitrectomy are procedures that can prevent further complications, such as corneal endothelium decompensation,leukoma, and secondary glaucoma. Surgical intervention can achieve a favorable retinal status to some extent and preserve some useful eyesight in advanced ROP cases.
The authors thank all the patients who were enrolled in the study.
Supported by the National Natural Science Foundation of China (No.81770963; No.81770964).
None;
None;
None;
None;
None;
None;
None;
None;
None.
1 Dogra MR, Katoch D, Dogra M. An update on retinopathy of prematurity (ROP).
2017;84(12):930-936.
2 Gold RS. ROP risk management 2021.
2021;32(5):494-497.
3 Azad R, Chandra P, Gangwe A, Kumar V. Lack of screening underlies most stage-5 retinopathy of prematurity among cases presenting to a tertiary eye center in India.
2016;53(Suppl 2):S103-S106.
4 Dou GR, Li MH, Zhang ZF, Lu YN, Zhu YN, Wang HY, Wang J, Wang XJ, Fan J, Wang YS. Demographic profile and ocular characteristics of stage 5 retinopathy of prematurity at a referral center in Northwest China: implications for implementation.
2018;18(1):307.
5 Sanghi G, Dogra MR, Katoch D, Gupta A. Demographic profile of infants with stage 5 retinopathy of prematurity in North India:implications for screening.
2011;18(2):72-74.
6 Sen P, Wu WC, Chandra P, Vinekar A, Manchegowda PT, Bhende P.Retinopathy of prematurity treatment: Asian perspectives.
(
)2020;34(4):632-642.
7 Karacorlu M, Hocaoglu M, Sayman Muslubas I, Arf S. Long-term functional results following vitrectomy for advanced retinopathy of prematurity.
2017;101(6):730-734.
8 Cusick M, Charles MK, Agrón E, Sangiovanni JP, Ferris FL 3rd,Charles S. Anatomical and visual results of vitreoretinal surgery for stage 5 retinopathy of prematurity.
2006;26(7):729-735.
9 Mintz-Hittner HA, O’Malley RE, Kretzer FL. Long-term form identification vision after early, closed, lens ectomy-vitrectomy for stage 5 retinopathy of prematurity.
1997;104(3):454-459.
10 Chiang MF, Quinn GE, Fielder AR,
. International classification of retinopathy of prematurity, third edition.
2021;128(10):e51-e68.
11 Gopal L, Sharma T, Shanmugam M, Badrinath SS, Sharma A,Agraharam SG, Choudhary A. Surgery for stage 5 retinopathy of prematurity: the learning curve and evolving technique.
2000;48(2):101-106.
12 Rajan RP, Kannan NB, Sen S, Lavanya C, Jena S, Kumar K,Vijayalakshmi P, Ramasamy K. Clinico-demographic profile and outcomes of 25-gauge vitrectomy in advanced stage 5 retinopathy of prematurity.
2021;259(7):1695-1701.
13 Chandra P, Kumawat D, Tewari R. Hybrid clear corneal micro-incision surgical technique for stage 5 retinopathy of prematurity.
2019;67(6):936-938.
14 Lai YH, Chen HL, Yang SN, Chang SJ, Chuang LY, Wu WC. The characteristics of premature infants with transient corneal haze.
2018;13(3):e0195300.
15 Nieves-Moreno M, Yeo D, Patel HI, Reddy MA. The frequency of severe corneal opacities in premature infants.
2021;25(4):221.e1-221.e5.
16 Treister G, Machemer R. Results of vitrectomy for rare proliferative and hemorrhagic diseases.
1977;84(3):394-412.
17 Sen P, Jain S, Bhende P. Stage 5 retinopathy of prematurity: an update.
2018;8(4):205-215.
18 Hirose T, Katsumi O, Mehta MC, Schepens CL. Vision in stage 5 retinopathy of prematurity after retinal reattachment by open-sky vitrectomy.
1993;111(3):345-349.
19 Clarkson JG, Jacobson SG, Frazier-Byrne S, Flynn JT. Evaluation of eyes with stage-5 retinopathy of prematurity.
1989;227(4):332-334.
20 Sen P, Bhende P, Sharma T, Gopal L, Maitray A, Shah P, Oke Y.Surgical outcomes of microincision vitrectomy surgery in eyes with retinal detachment secondary to retinopathy of prematurity in Indian population.
2019;67(6):889-895.
21 Fuchino Y, Hayashi H, Kono T, Ohshima K. Long-term follow-up of visual acuity in eyes with stage 5 retinopathy of prematurity after closed vitrectomy.
1995;120(3):308-316.
22 Machemer R, DeJuan E. Retinopathy of prematurity: approaches to surgical therapy.
1990;18(1):47-56.
23 Hartnett ME, Toth CA. Experimental evidence behind clinical trial outcomes in retinopathy of prematurity.
2019;50(4):228-234.
24 Iwahashi C, Utamura S, Kuniyoshi K, Sugioka K, Konishi Y, Wada N, Kusaka S. Factors associated with reactivation after intravitreal bevacizumab or ranibizumab therapy in infants with retinopathy of prematurity.
2021;41(11):2261-2268.
25 Yonekawa Y, Wu WC, Nitulescu CE, Chan RVP, Thanos A, Thomas BJ, Todorich B, Drenser KA, Trese MT, Capone A Jr. Progressive retinal detachment in infants with retinopathy of prematurity treated with intravitreal bevacizumab or ranibizumab.
2018;38(6):1079-1083.
26 Nudleman E, Muftuoglu IK, Gaber R, Robinson J, Drenser K, Capone A, Trese MT. Glaucoma after lens-sparing vitrectomy for advanced retinopathy of prematurity.
2018;125(5):671-675.
27 Senthil S, Balijepalli P, Garudadri C, Jalali S. Clinical presentation and management outcomes of coexistent congenital glaucoma and retinopathy of prematurity.
2019;28(1):20-26.
28 Choi MY, Yu YS. Anatomical and visual results of vitreous surgery for advanced retinopathy of prematurity.
1998;12(1):60-67.
29 Prost ME. Results of treatment of retinal detachment in active stage-5 retinopathy of prematurity.
2003;105(6):387-391.
30 Kusaka S. Current concepts and techniques of vitrectomy for retinopathy of prematurity.
2018;8(4):216-221.
猜你喜欢
儿童故事画报·自然探秘(2022年3期)2022-04-27
中学生英语·阅读与写作(2020年9期)2020-12-28
民生周刊(2020年22期)2020-11-16
青年文学家(2020年28期)2020-11-02
延河·绿色文学(2020年7期)2020-09-10
少年文艺(2019年5期)2019-05-28
祝您健康(2018年6期)2018-06-04
科学大众(中学)(2018年12期)2018-02-21
Coco薇(2016年4期)2016-04-06
 International Journal of Ophthalmology2022年9期
International Journal of Ophthalmology2022年9期
- International Journal of Ophthalmology的其它文章
- Clinical analysis of bilateral acute depigmentation of the iris: first reported case in China
- Interferon-gamma release assays in tuberculous uveitis:a comprehensive review
- Ocular stem cells: a narrative review of current clinical trials
- Different compression sutures combined with intracameral air injection for acute corneal hydrops
- Comparison of intravitreal aflibercept and dexamethasone implant in the treatment of macular edema associated with diabetic retinopathy or retinal vein occlusion: a Meta-analysis and systematic review
- Reproducibility of macular perfusion parameters in nonproliferative diabetic retinopathy patients by two different OCTA sweep modes