
Clinical value of phenylephrine testing in the upper and lower eyelids of patients with aponeurotic and congenital eyelid ptosis
2022-09-14 06:37OzgunMelikeGedarTotukMeltemGuzinAltinelAyseYagmurKanraUmitAykan
关键词:根系
INTRODUCTION
Eyelid ptosis, which is an abnormal function of the levator palpebra superioris muscle or Müller’s tarsal muscle, is one of the common eyelid disorders seen in oculoplastic surgery. The etiology of ptosis can be congenital,myogenic, neurogenic, and aponeurotic
. Ophthalmic plastic surgeons evaluate levator function (LF) and response to topical phenylephrine for the preoperative evaluation and determination of the appropriate surgical method for ptosis repair, but there is an underestimated situation; upper eyelid ptosis can change the lower eyelid position in both congenital and aponeurotic subgroups of ptosis to maintain the horizontal visual axis without inclination of the head in the primary gaze position
. The possible mechanism of this harmony is a compensatory contraction of the superior rectus/levator complex and simultaneous lower eyelid retractor, thereby displacing the globe upward in the orbit and retracting the lower eyelid with a dynamic lower scleral show
. Few previous studies have highlighted this issue and have shown that lower scleral show improves after ptosis surgery
. The need for a detailed evaluation of the lower eyelid for more precise and successful ptosis surgery prompted us to design this study.
The levator palpebra superioris, the major upper eyelid elevator muscle, contains striated muscle fibers and acts together with Müller’s muscle
. Müller’s muscle and the lower eyelid tarsal muscle are sympathetically stimulated smooth muscles that contract and widen the interpalpebral fissure in the presence of a topical adrenergic such as phenylephrine, a direct alpha-1 adrenergic agonist
. The response to topical phenylephrine is predictive of the outcome of a Müller’s ptosis repair
.Although interpalpebral fissure height is dependent on the lower eyelid position, changes in the lower eyelid position with phenylephrine are not usually measured before surgery
.Eyelid position is frequently described using the marginal reflex distance (MRD) alone for the upper eyelids
.
This study aimed to determine the time in which the maximal response of upper and lower eyelids to phenylephrine testing occurred, the correlation between the upper and lower eyelids,and to compare the test results of different groups of ptosis etiology and severity at different time points.
SUBJECTS AND METHODS
This study was approved by the Institutional Ethics Committee of Bahcesehir University (Date 4.9.2019,No. 2019-12/05), and conducted in compliance with the latest version of the Declaration of Helsinki. Informed consent was obtained from all of the patients.
This was a retrospective analysis of 140 eyes of 87 patients with upper eyelid ptosis who were referred to our clinic between September 2018 and May 2019.Our study included eyes with aponeurotic and congenital upper eyelid ptosis with good LF (>8 mm). The exclusion criteria were eyelid pathologies such as lower eyelid laxity, a history of previous eyelid surgery or trauma (traumatic ptosis), tumors causing mechanical ptosis or any other known eyelid disease;neurotoxin application 5mo before the phenylephrine testing;systemic or neurologic diseases that might affect eyelid position(such as Parkinson’s disease, Horner syndrome, stroke, cranial nerve palsy, thyroid eye disease, myasthenia gravis).
Baseline ophthalmologic examinations for ptosis included:measurements of Snellen visual acuity, MRD1 defined as the distance from the light reflex to the upper lid margin and MRD2 as the distance to the lower lid margin, LF, scleral show height, and slit-lamp anterior and posterior segment examinations. Eyes with aponeurotic ptosis were divided into four subgroups: age-related, post-operative, contact lens (CL)-induced, and idiopathic etiology.
MRD1 is the distance between the inferior margin of the upper eyelid and the pupillary light reflex in the primary position of gaze. The normal range of MRD1 is 4-4.5 mm. It is measured using a millimeter ruler held adjacent to the patient’s lateral canthus while the patient is in the sitting position, looking at a light source (a penlight) placed 50 cm away from the margin of the upper eyelid. A finger is placed over the patient’s brow to ensure frontalis relaxation
. Ptosis was defined as mild if the MRD1 was >1.5 mm, moderate if it was 0.5-1.5 mm, and severe if it was <0.5 mm. MRD1 has a negative value if the upper lid margin obstructs the corneal reflex. This value is based on the elevation of the ptotic eyelid until the light reflex appears
.
赖尔,本名周丽,作家,曾获中国“五个一工程奖”贡献奖,因其作品长篇魔幻小说《魔法城》而被意少小读者熟知。生活中的她,时而是纵横游戏世界大杀四方的女汉子,时而是独自行走领略各国风情的游者,时而又是咖啡馆里安静读书的文艺淑女……自由洒脱和沉稳睿智这两种特质在她身上得以完美融合。
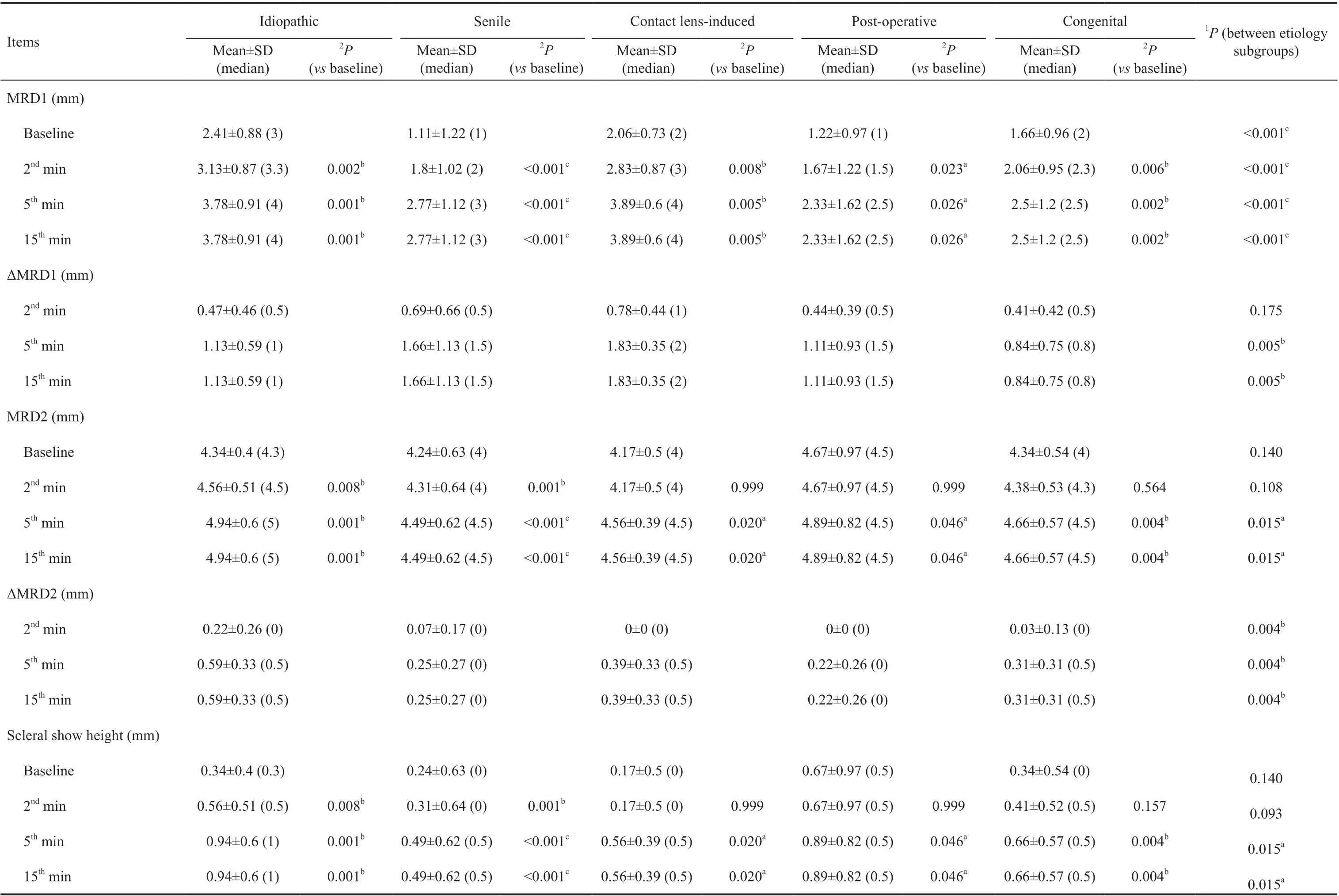
The evaluation of the mean values of MRD1,ΔMRD1, MRD2, ΔMRD2, and scleral show height, with respect to the etiology of ptosis, showed that regardless of the etiology, an increase was observed in all parameters at all measurement times after phenylephrine testing (
<0.05;Table 3). The ΔMRD1 was highest in eyes with CL-induced ptosis and lowest in eyes with congenital ptosis at the 5
and 15
minutes (
<0.005; Table 3). On the other hand, scleral show height was highest in eyes with idiopathic ptosis, and lowest in those with senile ptosis at the 5
and 15
minutes(
=0.015; Table 3).
当前国内质量控制工具的利用尚不成熟,仍处于学习阶段。而在美国的笔译项目中,术语管理贯穿整个项目,质量控制更是一个动态过程,并紧密结合各类计算机软件技术。
Patients’demographics, side of ptotic eye, etiology of ptosis, and concomitant systemic and ocular diseases were recorded.MRD1, MRD2, and scleral show height were measured at baseline, and the 2
, 5
, and 15
minutes of the phenylephrine testing, and recorded by the same author (Gedar Totuk OM).All measurements are given in units of 0.5 mm.
另外,本文控制了其他影响创新的主要因素[3],包括制度 (INS)、人力资本研究与开发(HKRD)、基础设施 (INFR)、市场成熟度 (MS)和商业成熟度 (BS)5个因素。此外,考虑到时间和空间的影响,本文还控制了年份和地域的影响。
总之,“共享经济”实质上是以盈利为目的的共享,它是人们既担任“消费者”又充当“拥有者”,它把使用权和所有权分离,并实现二者的相互转化,赢得更高的规模效益。它通过对消费者需求的分析进行资源配置和需求匹配,以最高的精度满足客户的需求,同时发挥资源自身的价值。“共享经济”平台的运行是一个取代了传统中介机构,基于自身庞大的供给资源和需求客户实现再中介化的过程,它持续健康发展的成本收益性也是它利润的最主要来源。“共享经济”的运行机制为我国加快转变经济发展方式提供了新的方向和动力。
The mean age of the patients was 52.29±16.45 (range, 16-80)y.Twenty-two (25.3%) of the patients were male and 65 (74.7%)were female. The eyelid ptosis was unilateral in 34 (39.1%)patients and bilateral in 53 (60.9%) patients. The ptosis duration (years) was recorded as 7.19±11.47 (range 0.08-45)y.According to the etiology, 124 eyes (88.6%) had aponeurotic and 16 eyes (11.4%) had congenital ptosis. The most common aponeurotic ptosis subgroup was senile ptosis (72%). The severity of ptosis was mild or moderate in 114 eyes (81.4%;Table 1).
翻译活动要以社会主义核心价值观为导向,加强思想引领,保证意识形态领域的正确价值取向;把握好翻译活动的文化导向,提高翻译人员的思想自觉性和文化自信心;推动翻译领域的供给侧结构性改革,以人民群众喜闻乐见的语言开展翻译活动;坚持翻译为人民服务,为社会主义服务,更好满足人们日益增长的美好生活需求,为两个一百年伟大目标的实现在思想文化领域提供可靠的翻译保证。
某调蓄水池位于壶关县,工程级别为Ⅲ等3级,总容积14万m3,地面高程为970.0~975.0 m,场地地基持力层为低液限粉土,结构较松散,为弱—中等透水层,场地为自重湿陷性,地基湿陷等级为Ⅱ等(中级),湿陷土层下限深度12 m。
In the phenylephrine testing, one drop of phenylephrine 2.5%solution (Mydfrin 2.5%, Alcon Laboratories Inc., Fort Worth,TX, USA) was instilled in the inferior cul-de-sac of the ptotic eye. The examiner’s finger depressed the lower lid while instilling the phenylephrine drop.
MRD2 is the distance between the central portion of the lower eyelid and the pupillary light reflex in the primary position of gaze.
Shapiro-Wilk test was used to examine the normality of data distribution. The study data are summarized using descriptive statistics including the mean±standard deviation (SD), median for continuous variables, and numbers and percentages for categorical variables. Data were analyzed using the Kruskal-Wallis test, followed by Dunn’s post hoc test to compare pairs.The Mann-Whitney
test was used to compare quantitative variables between two groups. The Wilcoxon signed-rank test was used for comparing quantitative variables in the groups.Analysis of qualitative variables was performed using the Chisquare test and the Fisher-Freeman-Halton test. Spearman’s rho test was used for correlation analysis between parameters.Probability values of less than 0.05 were considered significant.
The response of the lower eyelid tarsal muscle to phenylephrine is quantified using the change in MRD2 (ΔMRD2) and the scleral show height. ΔMRD2 is post-phenylephrine MRD2 value minus the baseline MRD2 value for each time point.ΔMRD2 equals the change of the scleral show height. ΔMRD2 was categorized as follows: 0, 0.5-1 or >1 mm.
Statistical analysis was performed using the IBM SPSS Statistics 22 package (IBM SPSS, Turkey). The
[8][15]李延瑞、梁玉璋:《宁德语音的近期演变及其途径》,《福建师大学报》(哲学社会科学版)1982年第2期。
The response of the Müller’s muscle to phenylephrine is characterized by the change in MRD1 (ΔMRD1). ΔMRD1 is equal to the post-phenylephrine MRD1 value minus the baseline MRD1 value for each time point. ΔMRD1 was categorized as follows: 0, 0.5-1, 1.5-2, and >2 mm.
葡萄种植面积的扩张速度已经超出了我们的预料,也培养了市场的大众化消费。在质量问题上,生产者着实有待改变理念,增强优果意识。现在优果高价市场不是没有,只是种植者缺乏底气,也缺少抱团取暖、开创市场的信心和勇气。有时候觉得一般果和优质果售价差异不大,而优质果管理上要求更高,技术更严,觉得下那功夫不划算。殊不知,一些公司或家庭农场,早已经开始了绿色无公害和有机果品生产,且颇受高端消费者青睐。单家独户的种植者也应该转变理念,积极尝试。
RESULTS
The scleral show is an anatomic condition in which the scleral area is abundantly visible. Its height is the distance between the central portion of the lower eyelid and the central portion of the inferior corneal limbus. Baseline scleral show height is classified as 0, 0.5-1, and >1 mm.
Thirty-three (37.9%) of 87 patients had an accompanying systemic disease, the most common was hypertension(16%), followed by thyroid diseases (11.4%). Sixty-one(43.6%) of 140 eyes had previous ophthalmic disease or surgery. The most common previous ophthalmic surgery was phacoemulsification+intraocular lens implantation (12.8%).The most common accompanying ophthalmic disease or condition was dry eye syndrome (5%), and CL use (6.4%).
The mean MRD1,MRD2, and scleral show heights before phenylephrine testing(baseline) were 1.39±1.20, 4.29±0.62, and 0.29±0.62 mm,respectively. These values increased within 5min after testing but remained largely stable between the 5
-15
minutes(Figure 1). The ΔMRD1 and ΔMRD2 were 0.62±0.60 and 0.07±0.18 at the 2
minute of the test, and 1.48±1.03 and 0.59±0.63 at the 5
minute, respectively. The values of the ΔMRD1 and ΔMRD2 at the 15
minute remained the same as the 5
minute. The ΔMRD1 and ΔMRD2 values showed a significant but weak correlation at all measurement times(Table 2).
At baseline, the scleral show height was 0 and 0.5-1 mm in 67.1%and 27.1% of eyes, respectively (Figure 2). The percentage of eyes with scleral show height of 0.5-1 mm or >1 mm was significantly higher in patients aged over 60y compared with those aged under 60y (39.4%
27%,
=0.044). TheΔMRD1 was 0.5-1 mm in 62.9% of eyes in the 2
minute of phenylephrine testing, and >1.5 mm in 52.8% of eyes at the 5
and 15
minute (Figure 2). Similarly, the percentage of eyes with a ΔMRD2 of 0.5-1 mm increased from 14.3% in the 2
minute to 54.3% at both the 5
and 15
minutes (Figure 2).


For the assessment of LF, the patient’s frontalis muscle was stabilized with a finger placed above the brow while the patient looked from far downgaze to far upgaze. The distance from the upper palpebral margin position in the down-gaze and the upper palpebral margin position in upgaze is the LF.This measurement was performed before the test only. LF was evaluated as excellent (13-15 mm), good (8-12 mm), fair(5-7 mm), and poor (4 mm)
.


Considering the percentage of eyes in the classifications of MRD1, ΔMRD1, MRD2, and ΔMRD2, a higher percentage of eyes with senile or CL-induced ptosis showed >1.5 mm ΔMRD1; other etiology groups showed less change in MRD1 at the 5
and 15
minutes (
=0.005; Table 4). When the ΔMRD2 was taken into consideration, it was observed that the percentage of eyes with the greatest change (0.5-1 mm)was highest in the eyes with idiopathic ptosis, and CL-induced ptosis at the 5
and 15
minutes (87.5%
66.7%, respectively;
=0.038, Table 4).
The percentage of older patients (aged over 60y) was highest in eyes with senile ptosis and post-operative ptosis (
<0.001;Table 4). Severe ptosis was also more common in eyes with senile ptosis and post-operative ptosis than in the other etiology groups (
=0.015; Table 4). The baseline scleral show height increased with increasing severity of ptosis (
=0.047;Table 4). The percentage of eyes with higher ΔMRD1 also increased with increasing severity of ptosis at the 2
, 5
, and 15
minutes of the phenylephrine test (
=0.003,
<0.001, and
<0.001, respectively; Table 4).
DISCUSSION
The use of topical phenylephrine in ptotic eyes was popularised by Putterman and Fett
, and has been used to predict the surgical outcomes of ptosis correction. In this study,we aimed to evaluate the changes in the upper and lower eyelid positions with phenylephrine testing, and to determine the appropriate timing of phenylephrine tests according to the responses at the 2
, 5
, and 15
minutes. We also assessed the effect of the etiology and severity of ptosis on eyelid positions after phenylephrine testing. Studies vary in the time after phenylephrine instillation at which MDR1 measurements are acquired to evaluate the patient’s reaction to the drug
.Most oculoplastic surgeons use the phenylephrine test in preoperative planning, waiting at least 5min before measuring MRD1
. In our study, the measurements of the 5
and 15
minutes MRD1, MRD2, scleral show height, ΔMRD1, and ΔMRD2 were better than the measurements of the 2
minute.In accordance with previous reports, in our study, the values did not change after the 5
minute and remained stable up to the 15
minute. The results of this study indicated that maximal responses with phenylephrine occurred in 5min after administration in all groups. Therefore, patients do not have to wait for long after drop placement in a busy clinic setting.

In our study, we used one drop of 2.5% phenylephrine instead of 10%. In a report, eyelids receiving 10% phenylephrine were an average of 0.2 mm higher than the same eyelids tested with 2.5% phenylephrine
. Given that this is a small and clinically insignificant magnitude of difference, and there is a higher risk of adverse systemic adverse effects of high-dose phenylephrine such as subarachnoid hemorrhage, ventricular arrhythmia, and severe hypertension, 2.5% phenylephrine should be chosen instead of 10%
. In our study, the most common concomitant systemic disease was hypertension (16%), one patient had coronary artery disease, and another had cerebrovascular disease. Using 10% phenylephrine could be a potential risk for these patients, thus 2.5% phenylephrine was preferred. We detected no adverse effects during or after the test.
We observed a non-response (ΔMRD1: 0) or low response(ΔMRD1: 0.5-1 mm) to phenylephrine testing was seen more in the congenital ptosis groups. In previous phenylephrine test studies, this group was generally excluded and not studied,accordingly, it was not possible to make direct comparisons.The exact mechanism of ptosis in congenital ptosis is different from aponeurotic ptosis, so the differences in the responses may be due to the insufficient myogenic structure in congenital ptosis
. Heisel
reported that orbital septa in patients with congenital ptosis demonstrate consistent histologic disorganization and fibrosis.
基于设计的大豆根系L系统,在VC++6.0开发平台下,借助OpenGL强大的三维图形和模型库进行构建,系统充分考虑根系间夹角、侧根弯曲度和根系生长量的变化,并采用随机函数实现各量值的随机变化,从而使生成的图形具有更好的视觉效果,随机生成的大豆根系拓扑模型如图2所示。
Eighty-eight percent of eyelids with CL-related ptosis had a high ΔMRD1 response to phenylephrine in the 5
and 15
minutes of the test. Lee
reported that all eyelids with CL-related ptosis had a high response to phenylephrine. In our study, in the senile ptosis group, 22.2% of the eyelids responded >2 mm, and 52.8% responded >1.5 mm in the 5
and 15
minutes. These findings in phenylephrine response may help surgeons decide which eyelids should undergo Müller’s muscle resection surgery.
Eyelids with mild ptosis are known to benefit most from Müller’s muscle resection surgery because this technique can raise the lid by up to 2 mm
. In our study, non-response(ΔMRD1: 0) was seen slightly more in the moderate and severe ptosis groups than in the mild ptosis group. However,in the mild ptosis group, the rate of eyelids that had a ΔMRD1 response of ≥1.5 mm, was 38.8% at the 5
and 15
minutes, 9%did not respond, and the responses were insufficient in 52.2%.Lee
reported that the response rate of eyes to phenylephrine was 88% in mild ptosis. In our study, the rates of mild responder eyelids were less than those reported previously.On the contrary, eyelids with severe ptosis responded better,38.5% responded extremely well (ΔMRD1>2 mm), and 65.4% responded well (ΔMRD1≥1.5 mm) to phenylephrine testing. Sometimes in severe ptosis, baseline MRD1 values can be very low, therefore even an excellent response may be insufficient for treating ptosis completely. Nevertheless,based on these findings, phenylephrine testing has clinical value for eyes with severe ptosis in the decision for Müller’s muscle conjunctival resection (MMCR). In the literature, there were other studies that found results consistent with our study.Nacaroglu
compared the outcome of MMCR for mild/moderate versus severe involutional aponeurotic ptosis, and they found that higher surgical success rates were obtained in cases with mild-moderate ptosis and clinically acceptable success rates were obtained in cases with severe ptosis.Sweeney
compared outcomes between MMCR ptosis repair and external levator resection (ELR) in patients with severe involutional blepharoptosis, and found that MMCR ptosis repair is an effective approach in treating patients with severe ptosis, and it may offer superior outcomes to ELR. Patel
demonstrated that MMCR with or without tarsectomy does provide another alternative to the surgeon for the management of severe involutional blepharoptosis.
Most studies only reported changes in MRD1 values;however, MRD2 measurements are usually disregarded
.We reported both lower and upper eyelid responses with measurements of MRD1, MRD2, and scleral show height,and their changes with time. The baseline scleral show degrees were correlated with ptosis severity. The MRD2 measurements indicated that the responses were better at the 5
and 15
minutes than at the 2
minute, and the results of the 5
and 15
minutes were the same. For the 2
, 5
, and 15
minutes ΔMRD2 classifications, there was no significant difference between the ptosis severity groups (
>0.05).However, the lower eyelid response of the mild ptosis group was better than that of the moderate and severe ptosis groups,and the responses of the moderate group were better than the severe ptosis group at the 2
, 5
, and 15
minutes. Also, the idiopathic etiology group’s lower eyelid responses were faster and better than the other groups. It should be noted that the eyelids in the idiopathic etiology group mostly had mild ptosis,which may account for the good MRD2 response in this group.The ΔMRD2 was related with baseline scleral show degree.The mild ptosis group had lower scleral show measurements and higher ΔMRD2 values. The ΔMRD1 and ΔMRD2 values were poorly correlated in all measurement times. In accordance with our results, Kaskouli
reported that more severe myogenic ptosis was significantly associated with more severe preoperative scleral show. Preoperative MRD2 was the only factor predicting postoperative improvement of scleral show in myogenic ptosis
.
The main limitation of the present study is its retrospective design. The other limitation was that the eyelid measurements were obtained through a simple technique used in daily clinical examinations. Although this technique was shown to produce repeatable results in MRD measurements with deviations of less than 0.5 mm, the accuracy of the measurements could be further improved by using sophisticated techniques such as head position stabilization and digital imaging.
企业社会责任从内容的争论到企业社会责任报告的发布,经历了从理论到实践的飞跃。一旦一种理论成为实践的指导就获得了理论证实的合法地位。“我们知道,科学界利用规范的一个收获是,只要接受了这种规范,就有了一个标准来选择那些可以肯定有解的问题。”〔1〕30“有了一种规范,有了规范所容许的那种更深奥的研究,这是任何一个科学部门达到成熟的标志。”〔1〕9企业社会责任的提出、内容的界定以及最终形成共识被确定为评判企业非经济层面行为的规则和标准,实现了企业伦理从宽泛的而又抽象的甚至有点空洞的企业文化研究转变到务实的社会责任研究上,渡过了企业伦理研究对象模糊不清的阶段,这是它成熟的一种标志。
In conclusion, we found that the results of the phenylephrine testing at the 5
and 15
minutes were both the same, and higher than the 2
minute. Accordingly, it is sufficient to perform the test for 5min. It is possible to obtain more than 2 mm response in eyes with severe ptosis, which may guide the decision to perform Müller’s muscle resection. The upper and lower eyelid responses in phenylephrine testing were poorly correlated. However, the ΔMRD2 was related with baseline scleral show degree. It has been proposed in previous studies that the evaluation of preoperative scleral show may also be a postoperative predictive factor
. Although ptosis and its surgery have been evaluated for many years, studies on the lower and upper lid relationship and its effects on surgical results have been subjects of interest in recent years yet there are very few studies in the literature. In this sense, we think that our study draws attention to this issue, which should be evaluated in greater detail in further studies.
The conception and design of the study: Gedar Totuk OM, Altinel MG, Kanra AY, Aykan U;Study procedures and the measurements: Gedar Totuk OM;Analysis and interpretation of data: Gedar Totuk OM, Altinel MG, Kanra AY, Aykan U; Drafting the article or revising it critically for important intellectual content: Gedar Totuk OM,Altinel MG, Kanra AY, Aykan U; Final approval of the version to be submitted: Gedar Totuk OM, Altinel MG, Kanra AY,Aykan U.
None;
None;
None;
None.
1 Matsuo K, Kondoh S, Kitazawa T, Ishigaki Y, Kikuchi N. Pathogenesis and surgical correction of dynamic lower scleral show as a sign of disinsertion of the levator aponeurosis from the tarsus.
2005;58(5):668-675.
2 Sultana R, Matsuo K, Yuzuriha S, Kushima H. Disinsertion of the levator aponeurosis from the tarsus in growing children.
2000;106(3):563-570.
3 Kim CY, Zhao SY, Wu CZ, Yoon JS, Lee SY. Positional change of lower eyelid after surgical correction of congenital ptosis in the Korean population.
2013;131(4):540-542.
4 Teo L, Lee SY, Kim CY. Effect of upgaze on lower eyelid position in Korean patients with congenital ptosis.
2017;70(3):380-384.
5 Small RG, Sabates NR, Burrows D. The measurement and definition of ptosis.
1989;5(3):171-175.
6 Barsegian A, Botwinick A, Reddy HS. The phenylephrine test revisited.
2018;34(2):151-154.
7 Rootman DB, Sinha KR, Goldberg RA. Change in eyelid position following Müller’s muscle conjunctival resection with a standard versus variable resection length.
2018;34(4):355-360.
8 Carter KD, Frueh BR, Hessburg TP, Musch DC. Long-term efficacy of orbital decompression for compressive optic neuropathy of Graves’ eye disease.
1991;98(9):1435-1442.
9 Liu HP, Shao Y, Zhang D. Surgical correction of blepharoptosis using a modified levator aponeurosis-Müller muscle complex reinsertion technique.
2014;25(1):226-230.
10 Ahmad SM, Della Rocca RC. Blepharoptosis: evaluation, techniques,and complications.
2007;23(3):203-215.
11 Boboridis K, Assi A, Indar A, Bunce C, Tyers AG. Repeatability and reproducibility of upper eyelid measurements.
2001;85(1):99-101.
12 Putterman AM, Fett DR. Müller’s muscle in the treatment of upper eyelid ptosis: a ten-year study.
1986;17(6):354-360.
13 Shin MK, Kim NY, Ahn HB. Time-dependent response of eyelid height with a single drop of 2.5% phenylephrine in Korean ptotic patients.
2020;34(4):311-315.
14 Ayala E, Gálvez C, González-Candial M, Medel R. Predictability of conjunctival-Müellerectomy for blepharoptosis repair.
2007;26(4):217-221.
15 Glatt HJ, Fett DR, Putterman AM. Comparison of 2.5% and 10% phenylephrine in the elevation of upper eyelids with ptosis.
1990;21(3):173-176.
16 Jubbal KT, Kania K, Braun TL, Katowitz WR, Marx DP. Pediatric blepharoptosis.
2017;31(1):58-64.
17 Marenco M, Macchi I, Macchi I, Galassi E, Massaro-Giordano M,Lambiase A. Clinical presentation and management of congenital ptosis.
2017;11:453-463.
18 Gazzola R, Piozzi E, Vaienti L, Wilhelm Baruffaldi Preis F.Therapeutic algorithm for congenital ptosis repair with levator resection and frontalis suspension: results and literature review.
2018;33(4):454-460.
19 Díaz-Manera J, Luna S, Roig C. Ocular ptosis: differential diagnosis and treatment.
2018;31(5):618-627.
20 Heisel CJ, Heider A, Stewart KJ, Andrews CA, Kahana A. Orbital septum fibrosis in congenital ptosis correlates with eyelid function:a clinicopathologic study.
2019;35(5):469-473.
21 Lee GN. Response to phenylephrine testing in upper eyelids with ptosis.
2015;21(3):1-12.
22 Putterman AM, Urist MJ. Müller muscle-conjunctiva resection. Technique for treatment of blepharoptosis.
1975;93(8):619-623.
23 Putterman AM. Müller’s muscle-conjunctival resection ptosis procedure.
1978;9:27-32.
24 Thomas GN, Chan J, Sundar G, Amrith S. Outcomes of levator advancement and Müller muscle-conjunctiva resection for the repair of upper eyelid ptosis.
2017;36(1):39-42.
25 Dan J, Sinha KR, Rootman DB. Predictors of success following müller’s muscle-conjunctival resection.
2018;34(5):483-486.
26 Nacaroglu SA, Karabulut GO, Fazil K, Serefoglu Cabuk K, Kandemir Besek N, Taskapili M. Comparing the outcome of Müller’s muscle conjunctival resection for mild/moderate versus severe involutional aponeurotic ptosis.
2021;31(6):3436-3441.
27 Sweeney AR, Dermarkarian CR, Williams KJ, Allen RC, Yen MT.Outcomes after Müller muscle conjunctival resection versus external levator advancement in severe involutional blepharoptosis.
2020;217:182-188.
28 Patel RM, Aakalu VK, Setabutr P, Putterman AM. Efficacy of Müller’s muscle and conjunctiva resection with or without tarsectomy for the treatment of severe involutional blepharoptosis.
2017;33(4):273-278.
29 Kashkouli MB, Abdolalizadeh P, Hadi Y, Amirsardari A, Jafari S,Karimi N. Change in lower eyelid position after ptosis repair in patients with unilateral myogenic versus aponeurotic blepharoptosis.
2019;35(4):383-386.
猜你喜欢
伴侣(2022年5期)2022-06-20
伴侣(2022年5期)2022-06-16
今日农业(2021年24期)2021-09-02
三农资讯半月报(2020年23期)2020-12-18
湖北农业科学(2019年22期)2019-12-23
农家致富顾问·下半月(2019年7期)2019-09-28
人民长江(2019年7期)2019-09-10
家教世界·创新阅读(2019年4期)2019-05-04
情感读本·道德篇(2018年4期)2018-06-22
家教世界·创新阅读(2017年11期)2017-11-27
 International Journal of Ophthalmology2022年9期
International Journal of Ophthalmology2022年9期
- International Journal of Ophthalmology的其它文章
- Clinical analysis of bilateral acute depigmentation of the iris: first reported case in China
- Interferon-gamma release assays in tuberculous uveitis:a comprehensive review
- Ocular stem cells: a narrative review of current clinical trials
- Different compression sutures combined with intracameral air injection for acute corneal hydrops
- Comparison of intravitreal aflibercept and dexamethasone implant in the treatment of macular edema associated with diabetic retinopathy or retinal vein occlusion: a Meta-analysis and systematic review
- Reproducibility of macular perfusion parameters in nonproliferative diabetic retinopathy patients by two different OCTA sweep modes