
胰腺癌导致的十二指肠梗阻经肝放置营养管1例
2015-10-28 09:01贾中芝田丰王凯蒋国民
介入放射学杂志 2015年6期
贾中芝,田丰,王凯,蒋国民
·病例报告Case report·
胰腺癌导致的十二指肠梗阻经肝放置营养管1例
贾中芝,田丰,王凯,蒋国民
晚期胰腺癌导致的胆道及十二指肠梗阻患者生存期一般较短,对此类患者应以最小的创伤方法治疗为主。本文报道1例晚期胰腺癌导致的胆道及十二指肠梗阻患者,胆道梗阻给予胆道支架治疗后解除了梗阻性黄疸,由于此患者心脏功能不全不能耐受胃空肠吻合术,并且在DSA下和内窥镜下放置支架及营养管失败,最后采取经肝、胆道支架放置营养管治疗,获得了一定的疗效。
胰腺癌,十二指肠梗阻,营养管
1 INTRODUCTION
Thesurvivalperiodofduodenalobstruction patients due to unresectable pancreatic cancer is only about 12 weeks[1].However,in the setting of bothbiliary and duodenal obstruction,the survival period becomes further shorter[2].Considering the systemic condition and poor prognosis,for such patients it is obligatory to employ minimally-invasive therapeutic scheme as far as possible.In the previous clinical practice,gastrojejunostomy[3]was regarded as the standard minimally-invasive treatment for malignant duodenal obstruction,but for recent years endoscopic duodenal stenting has been increasingly used topalliate duodenal obstruction[4].However,the use of endoscopy is difficult in some cases because of the malignant duodenal obstruction.Therefore,feedingtube placement is an alternative for patient with duodenal obstruction when gastrojejunostomy or endoscopic duodenal stenting is unable to be performed.
This paperdescribes anovel techniquefor feeding tube placement in a patient with duodenal obstruction,in whom all gastrojejunostomy,endoscopic duodenal stenting and routine feeding tube placement failed to success.
2 CASE REPORT
ThisstudyisapprovedbyourInstitutional Review Committee,and the informed consent to publish is obtained from the patient.
The patient was a 61-year-old female,who presented at the first medical visit with jaundice and wasdiagnosedofobstructivejaundicedueto inoperable pancreatic cancer.She was admitted to hospital to receive biliary stent placement,and was uneventfulatthetimeofdischarge.Noother treatmentwasemployed.Onemonthlater,she developednauseaandvomiting,andendoscopic examination revealed duodenal obstruction,and the duodenal papilla was not affected.As her cardiac ejection fraction was only 19%,gastrojejunostomy was definitely not suitable for her.Even worse,both duodenalstentingandfeedingtubeplacement,performed under fluoroscopic or endoscopic guidance, failed to success.
Therefore,a new technique of percutaneous tube placement,which was performed via trans-hepatic and biliary route,was suggested.A commercially available percutaneous transhepatic cholangiodrainage(PTCD)set(Cook Medical,Cook,USA)was used. After puncturing the bile duct,a 0.038 inch guide wire was inserted until its tip entered the jejunum(fig.1).Then,a 5-Fr sheath was introduced over the guide wire and a 5-Fr catheter(H1,Cook Co.Ltd.,Bloomington,USA)was advanced over the 0.038 inch guide wire until its tip was in the jejunum.The 0.038 inch guide wire was replaced by a long guide wire(150 cm in length;Radifocus Guide wire M Standard type,Terumo Co.Ltd.,Japan).Then,the 5-Fr catheter and sheath were removed,and the tunnel was dilated by a dilator;and a 90 cm-long 7-Fr guiding catheter(Vista Brite Tip Guiding Catheter,Johnson&Johnson Co.Ltd.,Miami,FL,USA)was co-axially inserted with the 5-Fr H1 catheter until its tip was in the jejunum(fig.2).Finally,both the guide wire and 5-Fr H1 catheter were removed(fig.3),and the 7-Fr guiding catheter outside of the body was fixed to the skin(fig.4).After the procedure,the patient received routine care,prophylactic antibiotics and odynolysis.Every day a total of 2 000-2 400 ml liquid food was administered through the guiding catheter.The patient died of multiple organ failure 28 days after the procedure with nooccurrenceof hemobilia or infection.
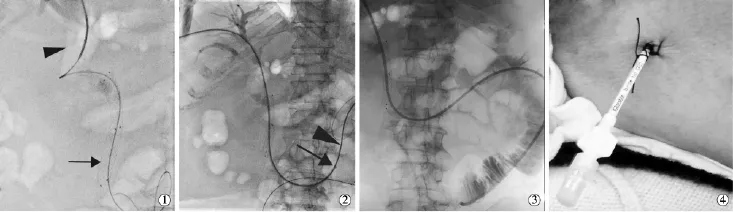
图1
3 DISCUSSION
During its progression,the inoperable malignant pancreatictumornotonlycancausebiliary obstruction,but also can cause duodenal obstruction. Both biliary and duodenal obstruction will cause a series of obvious clinical symptoms,such as jaundice,nausea,vomiting,anorexia,weight loss,etc.,and the quality of life will be markedly impaired.As the patient is usually in a very poor condition and only a very short survival time can be expected,it must be kept in mind that for the treatment of such patient the minimally-invasive and effective palliation technique should be adopted as the first choice.Traditionally,bypass surgery or duodenal stenting is employed to relieve the clinical symptoms.Nevertheless,what can we do for these patients who cannot tolerate the bypasssurgeryandbothduodenalstentingand feeding tube placement,performed under fluoroscopic or endoscopic guidance,are unsuccessful in them. This is a question that has baffled the clinicians.The authorshaveextensivelyreviewedtherelevant medical literatures published in PubMed,and have designed a novel technique for feeding tube placement.
In this paper,the authors reported a novel technique for feeding tube placement in a duodenal obstruction patient.A 7-Fr guiding catheter is used as a feeding tube because its lumen is larger than the usual feeding tube.The 7-Fr guiding catheter is not veryflexible,buttheincidenceofitslumen obstruction is rare.The 7-Fr guiding catheter is placed into the upper jejunum in order to avoid the biliary tract infection due to food reflux.Through this 7-Fr guiding catheter 2 000-2 400 ml liquid food daily was successfully delivered into the patient's intestine for 28 days until the patient died of multiple organ failure,while no hemobilia or infection occurred.The results indicate that this technique of feeding tube placementforduodenalobstructionisclinically feasible.
In conclusion,although percutaneous placement of feeding tube via transhepatic route for duodenal obstructionduetopancreaticcancerisnota commonly used technique,the use of this technique should be seriously considered when the patient can not tolerate a bypass surgery,or when both duodenal stenting and feeding tube placement failed to success.
[1]Dormann A,Meisner S,Verin N,et al.Self-expanding metal stents for gastroduodenal malignancies:systematic review of their clinical effectiveness[J].Endoscopy,2004,36:543-555.
[2]Mutignani M,Tringali A,Shah SG,et al.Combined endoscopic stent insertion in malignant biliary and duodenal obstruction[J]. Endoscopy,2007,39:440-447.
[3]Piesman M,Kozarek RA,Brandabur JJ,et al.Improved oral intake after palliative duodenal stenting for malignant obstruction:a prospective multicenter clinical trial[J].Am J Gastroenterol,2009,104:2404-2411.
[4]Tonozuka R,Itoi T,Sofuni A,et al.Endoscopic double stenting for the treatment of malignant biliary and duodenal obstruction due to pancreatic cancer[J].Dig Endosc,2013,25 Suppl 2:100-108.
Successful placement of nutrition tube via transhepatic route for duodenal obstruction due to pancreatic cancer:report of one case
JIA Zhong-zhi,TIAN Feng,WANG Kai,JIANG Guo-min.Department of Interventional Radiography,Second People's Hospital of Changzhou,Nanjing Medical University,Changzhou,Jiangsu Province 213003,China
JIANG Guo-min,E-mail:jgm916@163.com
Usually the survival period of patients with duodenal obstruction caused by inoperable advanced pancreatic cancer is rather short.For such patients,minimally invasive treatment should be employed as the first choice.This paper reported a case with advanced pancreatic cancer complicated by biliary and duodenal obstruction.After implantation of biliary stent,the obstructive jaundice was relieved. Because of the insufficient cardiac function,the patient was not able to tolerate gastrojejuostomy;besides,as both DSA-guided stent implantation and endoscopic nutrition tube placement failed to success,implantation of nutrition tube via the trans-hepatic and biliary route,as a novel tube placement technique,had to be carried out,and the result in this case was satisfactory.(J Intervent Radiol,2015,24:553-555)
pancreatic cancer;duodenal obstruction;nutrition tube
R735.8
D
1008-794X(2015)-06-0553-03
2014-09-13)
(本文编辑:顾伟中)
10.3969/j.issn.1008-794X.2015.06.022
江苏常州南京医科大学附属常州市第二人民医院介入血管科
蒋国民E-mail:jgm916@163.com
猜你喜欢
科学与财富(2020年29期)2020-12-21
科学与财富(2020年29期)2020-12-21
湖北理工学院学报(人文社会科学版)(2020年4期)2020-07-24
中华建设(2019年6期)2019-07-19
华人时刊(2017年17期)2017-11-09
天津护理(2016年3期)2016-12-01
金色年华(2016年2期)2016-02-28
肝胆胰外科杂志(2015年5期)2015-02-27
中华介入放射学电子杂志(2014年1期)2014-02-02
