
Robotic assisted radical prostatectomy accelerates postoperative stress recovery: Final results of a contemporary prospective study assessing pathophysiology of cortisol peri-operative kinetics in prostate cancer surgery
2016-04-27 06:33AntonioPorroNiolodeLuykPoloCorsiMroSeenAlessndroTfuriDvideInverrdiDvideDeMrhiIreneTmniniMtteoBrunelliMriAngelCerrutoGinLuSlvgnoGinCesreGuidiWlterArtini
Asian Journal of Urology 2016年2期
Antonio B.Porro*,Niolo`de LuykPolo Corsi Mro SeenAlessndro TfuriDvide Inverrdi Dvide De MrhiIrene TmniniMtteo Brunelli, Mri Angel CerrutoGin Lu Slvgno, Gin Cesre Guidi,Wlter Artini
aUrologic Clinic,University Hospital,Ospedale Policlinico,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
bDepartment of Pathology,University Hospital,Ospedale Policlinico,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
cDepartment of Laboratory Medicine,University Hospital,Ospedale Policlinico,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
Robotic assisted radical prostatectomy accelerates postoperative stress recovery: Final results of a contemporary prospective study assessing pathophysiology of cortisol peri-operative kinetics in prostate cancer surgery
Antonio B.Porcaroa,*,Nicolo`de Luyka,Paolo Corsia, Marco Sebbena,Alessandro Tafuria,Davide Inverardia, Davide De Marchia,Irene Tamaninia,Matteo Brunellib, Maria Angela Cerrutoa,Gian Luca Salvagnoc, Gian Cesare Guidic,Walter Artibania
aUrologic Clinic,University Hospital,Ospedale Policlinico,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
bDepartment of Pathology,University Hospital,Ospedale Policlinico,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
cDepartment of Laboratory Medicine,University Hospital,Ospedale Policlinico,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
Prostate cancer;
Robot assisted radical
prostatectomy;
Retropubic radical
prostatectomy;
Stress system
Objective:To investigate the effects of prostate cancer(PCa)surgery on the stress system and to identify potential independent factors associating with stress recovery.
Methods:The design of the study was prospective and PCa surgery included robot assisted radical prostatectomy(RARP)or retropubic radical prostatectomy(RRP).Between February 2013 to December 2014,315 consecutive patients were evaluated.The effects of PCa surgery on the stress system were measured by cortisol serum levels before and after surgery on postoperative day(POD)0,1,3,5 and 45.Cortisol variations in the population and subpopulation(RARP vs.RRP)of patients were investigated by statistical methods.Factors associating with stress recovery were assessed by simple linear regression(SLR)and multiple linear regression (MLR)analysis.
Results:RARP was performed in 75.9%of cases.In the patient population,there were wide serum cortisol perioperative variations.PCa surgery triggered the stress system which immediately (POD 0)responded by cortisol overproduction which induced the negative feedback mechanism that started on POD 1,continued on POD 3,was still ongoing on POD 5 and completely settled on POD 45(stress recovery).In the subpopulation of patients,significantly lower cortisol serum levelswere detected on POD 3-5 in RARP casesin whom cortisollevelswere close to preoperative levels(stress recovery)on POD 5.Independent predictive factors of serum cortisol on POD 5 (stress recovery)were preoperative cortisol(p=0.02),cortisol levels on POD 3(p<0.0001) and RARP(p=0.03)in which the association was negative(stress recovery faster than RRP). Conclusion:Our study shows that PCa surgery immediately(POD 0)triggers the stress system which respond by overproduction of cortisol which induces the negative feedback mechanism thatstarts on POD 1,isstillongoing on POD 5,butiscompletely settled on POD 45.Moreover,after surgical trauma,our study gives evidence that the RARP procedure associates with stress recovery faster than RRP.Further confirmatory studies are required.
ⓒ2016 Editorial Office of Asian Journalof Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Hypothalamus
-pituitary-adrenal
axis;
Cortisol hormone
1.Introduction
Prostate cancer(PCa)is the second most frequent solid tumor after lung cancer in adult males[1]and associates with a mortality rate of 1.2%[2].Radical prostatectomy (RP)is the most performed procedure for treating clinically localized PCa in men who have life expectancy more than 10 years,associates with extended lymph node dissection (LND)in high risk patients[3],and aims to eradicate cancer disease,to preserve urinary continence,and potency as well[3,4].RP may be performed by the open retropubic approach(RRP)or by minimally invasive laparoscopic techniques which include the laparoscopic RP(LRP)and robot assisted RP(RARP)techniques[3-5].Actually,RARP is increasingly displacing RRP all over the world[3,4],and associates with lesser blood loss than RRP.However,postoperative complications related to RARP and RRP appear similar.Although there are no prospective randomized trials comparing RRP vs.RARP,experts consider RARP a valuable therapeutic option for treating clinically localized PCa[5].
It has been shown that major surgery trauma induces profound immunological dysfunction[6]by triggering the stress system which is represented by the hypothalamic-pituitary-adrenal(HPA)axis[7-9].The HPA axis is a neuroendocrine system that regulates the circulating levels of glucocorticoid hormones(mainly cortisol)that are important for homeostasis and play a critical role in stress response[7-9].
The hormones of the stress system include the corticotrophin-releasing hormone(CRH)which is released by the hypothalamus,the adrenocorticotropic hormone (ACTH)which is produced by the pituitary and cortisol which is the main glucocorticoid hormone secreted by the adrenals.Approximately,95%of plasma cortisol is bound to proteins that include the cortisol binding globulin(CBG, 95%)and albumin(10%-15%);moreover,the remaining 5%is unbound,free to cross cell membranes and binds to glucocorticoid and mineralocorticoid receptors[9].
Major surgery is a significant challenge to homeostasis because it alters the steady state of neuroendocrine systems of which the most pivotal is the HPA axis[9].Clinical models and studies investigating on the stress system after major surgery are actually unknown.Although it has been shown that RARP is less invasive than RRP[10],studies dealing with the effects of RARP and RRP related to the stress system are missing.Actually,the pathophysiology of the HPA axis after PCa surgery is an unexplored field because we are missing clinical models which are important for progressing and improving care.The present study explores the pathophysiology of the stress system by RARP and RRP as well as complications related to the HPA axis by the two procedures.
2.Patients and methods
Exclusion criteria were as follows:(i)sarcoma of the prostate,(ii)preceding focal therapies,(iii)androgen blockade,(iv)history of glucocorticoid medications or adrenal surgery.The choice of the procedure,RARP or RRP,was based on a joint decision by urologists and patients who were sharply informed and provided written consent to surgery as well as to the use of their data. Robot assisted RP was delivered by the three-arm da Vinci Robot System(Intuitive Surgical,Inc,Sunnyvale,CA,USA) and performed by two experienced surgeons who were experienced in both techniques.The approach was transperitoneal with prostatic dissection in all cases[11]. RRP was performed by experienced surgeons according to the Walsh technique[12].According to the D’Amico class risk classification[13],LND was planned in all high riskpatients and intermediate risk cases with a risk of metastases≥5%according to the Briganti’s nomogram [14].The protocol after surgery was standardized for both procedures and patients were discharged on postoperative day(POD)4-6 when there were no further complications. The peri-operative surgical risk of patients was evaluated by the American Society of Anesthesiologists(ASA)score system[15].The complications were classified and coded according to Clavien-Dindo system(CDS)[16].
The study is part of a larger trial of PCa biobanking which has been already approved by the local Ethical Committee. The design was prospective and the data of each case were collected in one data base.The evaluated variables included age(years),body mass index(BMI,kg/m2),ASA score,baseline total prostate specific antigen(PSA)serum levels(ng/mL),proportion of positive cores(P+),prostate volume(PV,mL),operating time(OT,min),blood lost(BL, mL),clinical stage(cT),biopsy Gleason score(bGS),pathology Gleason score(pGS),pathologic tumor stage(pT), lymph node status(pN)and surgical margin status (R,1 positive,0 negative).PV was estimated by the ellipsoid method,using prostate diameters calculated from TRUS.In patients undergoing RARP,OT was calculated from the insertion of the Veress needle to the suture of the last laparoscopic port,whereas in RRP it was computed from skin incision to suture.Patients were classified according to primary tumor stage,lymph node and metastatic status, using the TNM categories recommended by the 1997 International Union against Cancer TNM classification system [17].Finally,the discharge day(DD,days)was measured as a continuous variable and reported as median and range, while readmission to the hospital(R-AD)was coded as a categorical variable.
Serum cortisol concentrations were measured on an Immulite 2000 automated immunoassay analyzer(Siemens Healthcare,Marburg,Germany)by the Immulite 2000 Cortisol assay.The Immulite 2000 Cortisol is a solid-phase, competitive chemiluminescent enzyme immunoassay, displaying a within-run imprecision of 4.9%-6.7%and 5.3%-10.8%,respectively[18].Cortisol venous blood samples were taken 20-30 days before surgery at 8:00 a.m. (Tb),4 h after surgery(T0),on POD 1(T1),3(T3),5(T5) and 45(T45).Serum levels of cortisol were expressed by ng/mL(normal range:4.0-25.0).
Statistical methods.It was used the advanced SPSS statistical software(IBM,Chicago,IL,USA).Data on continuous variables are reported as medians with their respective ranges,and differences between groups analyzed with the Mann-Whitney U test.Data on categorical variables are presented as proportions,and differences between groups analyzed with Pearson’s chi-squared test or Fisher exact test as appropriate.
To generate logistic simple logistic regression models of predictors associating with CDS≥3a,all continuous variables were entered as continuous variables unless otherwise stated.Only variables that were significant in univariate models were included in the multivariable analysis.To generate simple linear regression models of covariates associating with DD,all continuous variables were entered as continuous variables unless otherwise stated.Only variables that were significant in univariate models were included in the multivariable analysis.Where significant co-linearity existed between independent variables,the one with the most predictive power was used in preference in the multivariate model.Multivariate models were generated using a simple stepwise model.
All tests were two-sided with p<0.05 considered to indicate statistical significance.
3.Results
After excluding criteria,290 patients were evaluated. Surgery included RARP in 220 patients(75.9%)and RRP in 70 cases(24.1%).Table 1 shows the demographics of the cohort study.Patients who underwent RARP were younger (p=0.002),had lower median PSA levels(p<0.0001)and showed higher ASA 2 score rates(p=0.009).Patients who underwent RRP had higher median BL(p<0.0001),showed higher perioperative complications(p<0.0001)and R-AD(p<0.0001)rates than RARP cases who had lower median values of length of hospital stay(p<0.0001).
盖碗茶具的出现与饮茶习俗的变化发展密不可分,是在中国古代茶具积淀之上形成的,符合中国茶事美学与实用的茶具。如今,仍以其独特的人文属性及灵活可变的功能形制,在现代茶事活动中成为不可或缺的一类茶具。在茶文化大发展的时代背景下进行概念厘清及发展梳理,具有非常重要的现实意义。
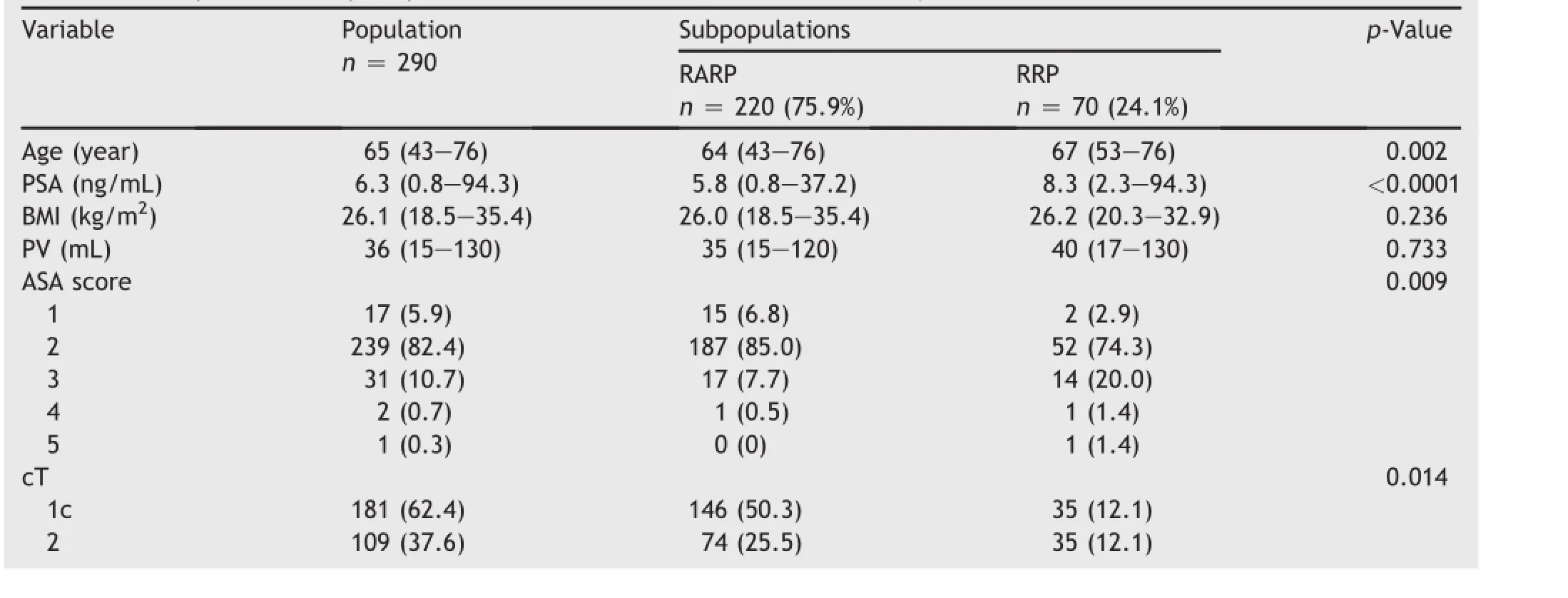
Table 1Preoperative and perioperative variables related to the cohort study.
Table 2 shows the perioperative kinetics of cortisol plasma levels.Preoperative basal levels of cortisol did not differ between RARP and RRP cases.Median cortisol plasma levels detected 4 h after surgery were significantly lower in RRP cases than RARP patients who however in the subsequent perioperative period showed lower median cortisol plasma levels on POD 5(p<0.0001)and 45(p<0.0001). Fig.1 depicts the variations(%)of cortisol plasma levels as follows:basal,perioperative period and POD 45.As reported,significant variations were detected at T0,T5 and T45.
Table 3 shows the logistic regression models predicting a Clavien-Dindo complication score≥3a.The multivariate logistic regression model showed that only DD(p<0.0001)and BL(p<0.0001)were independent predictors associating with CDS≥3a;however,the former showed a stronger association(OR=1.425;95%CI:1.168-1.739) than the latter(OR=1.002;95%CI:1.001-1.003).Because of the strong association of LOHS with the CDS,we computed a linear regression analysis in order to detect potential covariates predicting DD.As shown in Table 4, analysis of simple models showed that DD directly associated with LND(p<0.0001),age(p=0.015),ASA≥3, cortisol levels on POD 1(p=0.023),and cortisol plasma levels on POD 5(p<0.0001),but inversely with RARP (p<0.0001).However,analysis of the multivariate model showed that independent covariates predicting DD were ASA≥3(b=1.22;p<0.0001),CDS≥3a(b=1.253; p<0.0001),cortisol plasma levels on POD 5(b=0.097; p=0.002),and RARP(b=-0.901;p=0.005).As depicted in Fig.2,the median length of DD was significantly shorter in RARP cases(5 days)than RRP patients(6 days) who showed,as illustrated in Fig.3,significantly higher median plasma levels of T5 cortisol.
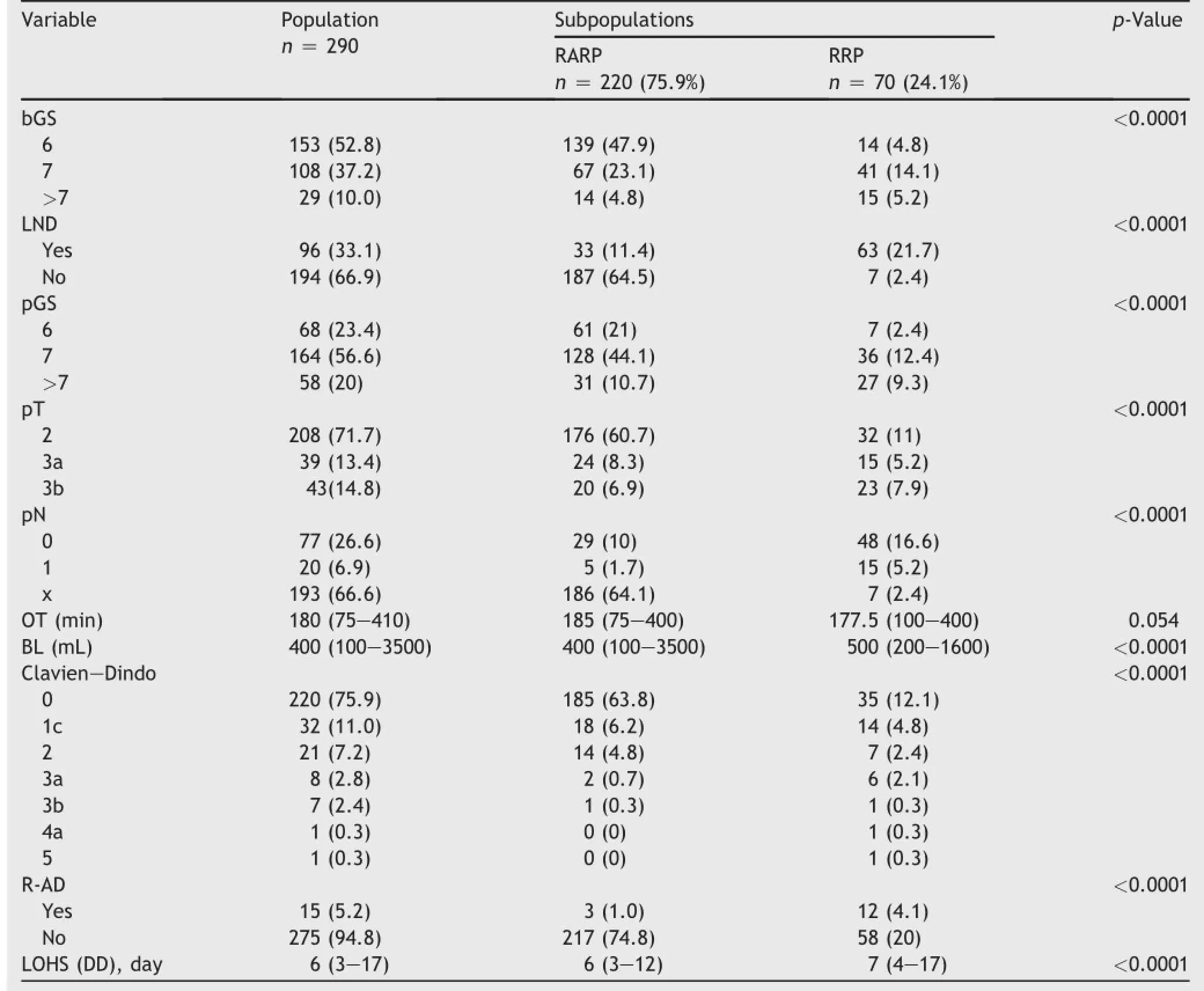
Table 1(continued)
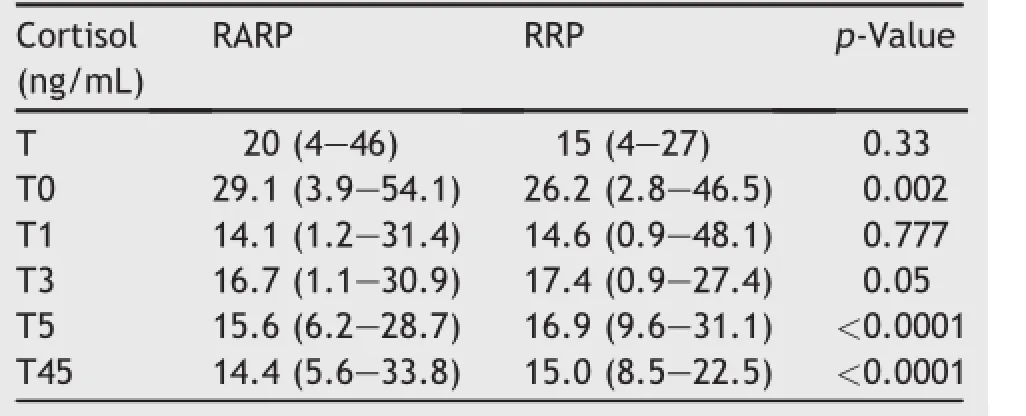
Table 2Basal and perioperative cortisol plasma levels in PCa patients undergoing surgery(median(range)).
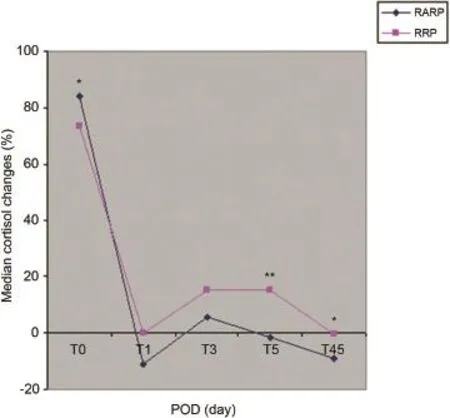
Figure 1Median cortisol perioperative changes(as percentage)from basal preoperative levels.*p<0.05,**p<0.001. RARP,robot assisted radical prostatectomy;RRP,retropubic radical prostatectomy;T0,cortisol 4 h after surgery;T1, cortisol on POD 1;T3,cortisol on POD 3;T5,cortisol on POD 5; T45,cortisol on POD 45.
4.Discussion
Major surgery trauma is a significant challenge to homeostasis because it activates compensatory autonomic and neuro-endocrine systems,of which the HPA axis is the most pivotal one[9].Initially,production of pro-inflammatory cytokines;tumor necrosis factor a(TNF-a)and interleukin-1(IL-1)and interleukin-6(IL-6)cause direct stimulation of CRH and ACTH by the hypothalamus and pituitary respectively.After stress stimulation,along the HPA axis,adrenal glands undergo cortisol overproduction;as a result,there is a significant increase in total serum levels of cortisol which is the main hormone in the pathway of the neuro-endocrine stress response.In the present study,we showed that the patient population recovered from stress on POD 5(sample F);moreover,stress recovery was more effective in RARP patients compared to RRP cases(Table 2 and Fig.3).Interestingly,as shown in Table 2,significant higher mean levels of cortisol were detected in RARPpatients on T0(few hours after surgical stress).An explanation of this finding might be related to the surgical injury and stretching of the peritoneum related to the laparoscopic procedure.The present study shows that RARP,along the HPA axis,is major surgical procedure that triggers lower stress levels than RRP,as shown by MLR analysis in which RARP showed a negative independent association with F cortisol(Table 3 and Fig.3).As a theory,the negative feedback mechanism of cortisol serum levels on the stress system were faster in patients who underwent RARP because of the negative association of the procedure with stress recovery.Indeed,as shown by F cortisol serum levels, the negative feedback was almost concluded in RARP patients while it was still ongoing in RRP cases.
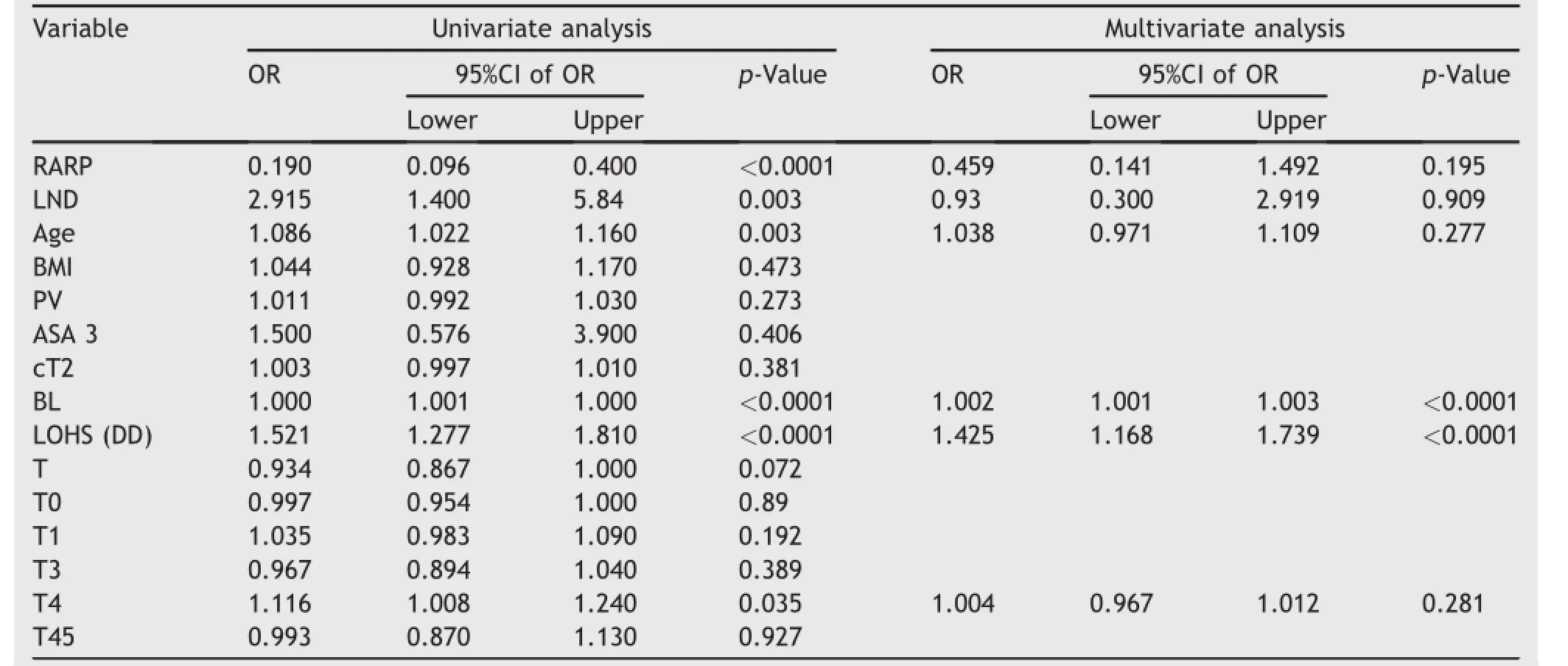
Table 3Covariates associating with Clavien-Dindo score≥3a by logistic regression analysis
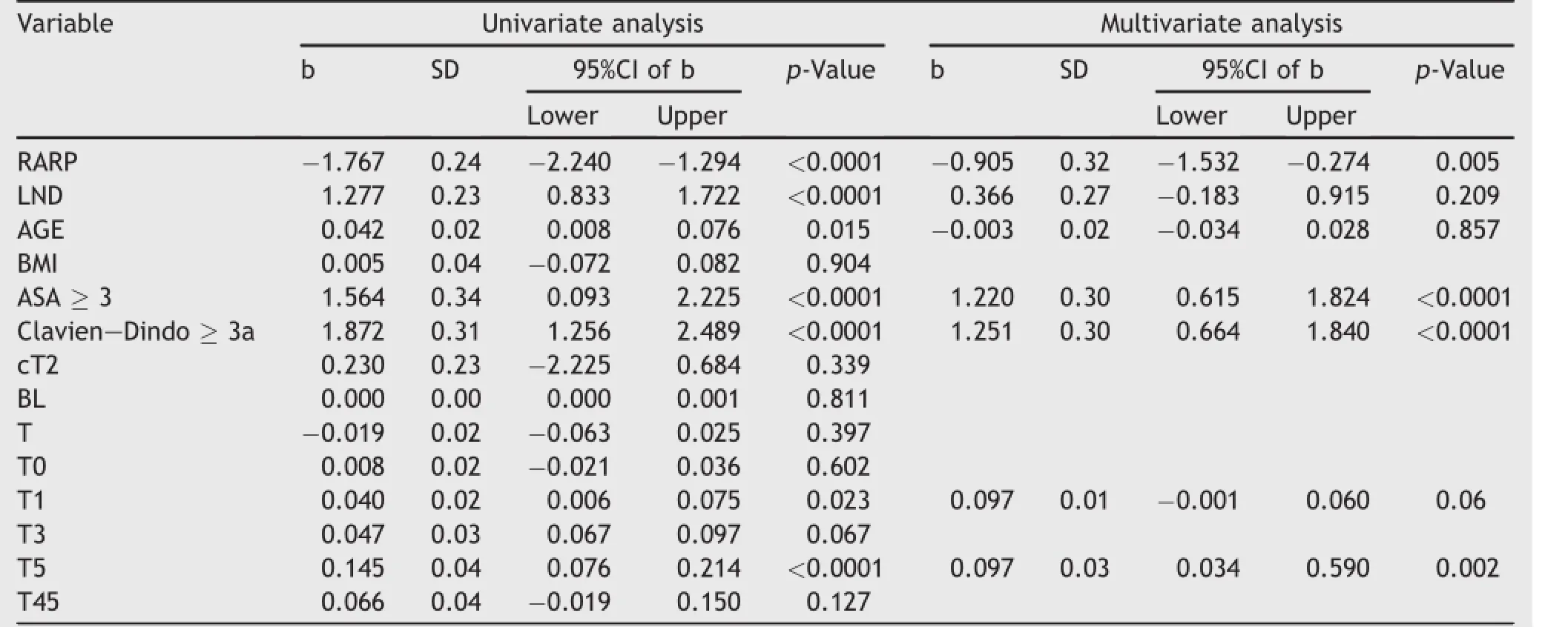
Table 4Covariates predicting LOHS(DD)by linear regression analysis.
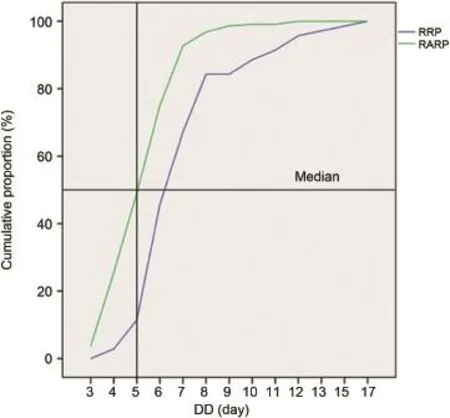
Figure 2Cumulative proportion(%)of length of hospital day (DD,days)in RARP and RRP patients.DD,discharge day; RARP,robot assisted radical prostatectomy;RRP,retropubic radical prostatectomy.
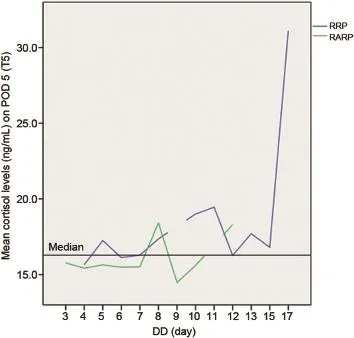
Figure 3Mean cortisol plasma levels(ng/mL)on POD 5(T5) as a function of DD(days)in RARP and RRP cases.Patients who underwent RARP show significantly lower median levels of cortisol plasma levels than RRP cases.DD,discharge day; POD,postoperative day;RARP,robot assisted radical prostatectomy;RRP,retropubic radical prostatectomy;T5,cortisol on POD 5.
It has been shown that RARP induces lower tissue trauma than RRP because of the more limited increase in acutephase inflammatory mediators,such as IL-6 and C reactive protein(CRP)[10].As a consequence,the stress system, along the HPA axis,is triggered to a lesser degree,according to the physiopathology of the stress system[6-9]. The present study shows that RARP accelerates surgical stress recovery along the neuroendocrine system.Our results are confirmed by an experimental study that compared the stress response to robotic technology during thoracoscopic mobilization and anastomosis of the esophagus vs.the conventional open approach[19].As a theory, RRP increased the hyper inflammatory response followed by cell-mediated immunosuppression which triggered higher stress levels along the HPA axis(Fig.4).Our study showed that acute stretching of the peritoneum by insufflation of carbon dioxide,as a trigger of cortisol release along the HPA axis,did not play an important role in RARP.Moreover, the lesser pain levels,as a theory,might explain the faster stress recovery following RARP.These different cortisol stress related kinetics could explain why,in RARP cases, cortisol levels on POD 4 to 5 were significantly lower than those detected in RRP patients(Table 3 and Fig.3).
There are limits in our study.First,the lack of randomized allocation of the patients might impact for the differences in the baseline characteristics of the two subpopulations,as shown in Table 1.However,now a days very few patients are willing to undergo randomization to RARP vs.RRP.As a result,the choice of surgical approach for RP is effectively based on the request and preference of the patient.Consequently,the present study reflects what’s daily clinical practice in a urologic unit.Second, factors triggering the stress system as well as the measurement of both CRH and ACTH were not investigated. Third,although significant differences between RARP and RRP related to age,PSA and ASA,the multivariate independent regression models(logistic and linear)showed that RRP strongly associated with major postoperative surgical complications(Clavien-Dindo score≥3a)that delayed LOHS.It would be interesting to compare the acquired data to studies that describe the cortisol level from other surgical procedures which are lacking at the moment.However,the present study confirms definitively the preliminary results of our trial[20]and provides a useful framework for planning further trials for investigating PCa surgery feed-backs on the stress system.As a theory,in high risk PCa surgery,the probability of disease progression, such as loco-regional and systemic migration of malignant cells,should be less likely when the stress system is triggered to lower degree levels and to a shorter perioperative period.
Therefore we conclude that our study shows that PCa surgery immediately(POD 0)triggers the stress system which respond by overproduction of cortisol which induces the negative feedback mechanism that starts on POD 1, is still ongoing on POD 5,but is completely settled on POD 45.Moreover,our study gives evidence that,after surgical trauma,the RARP procedure associates with stress recovery fester than RRP.Further confirmatory studies are required.
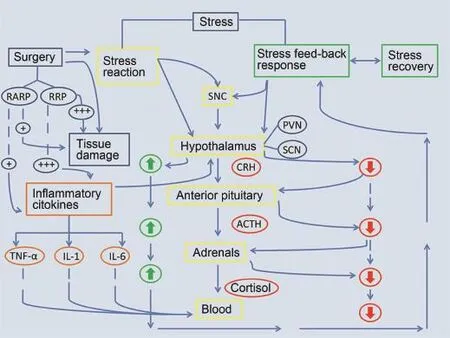
Figure 4Pathways of post-operative stress kinetics along the neuroendocrine system after acute surgical trauma(see Discussion section for details).ACTH,adrenocorticotropic hormone;CRH,corticotrophin-releasing hormone;RARP,robot assisted radical prostatectomy;RRP,retropubic radical prostatectomy;SNC,central nervous system;PVN,paraventricular nucleus;SCN, suprachiasmatic nucleus.
Conflicts of interest
The authors declare no conflict of interest.
[1]Siegel R,Niashadham D,Jemal A.Cancer statistic,2012.CA Cancer J Clin 2012;62:10-29.
[2]Ferlay J,Autier P,Boniol M,Heanue M,Colombet M,Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006.Ann Oncol 2007;18:581-92.
[3]Heidenreich A,BellmuntJ,Bolla M,Joniau S,Mason M,Matveev V, et al.,European Association of Urology.EAU guidelines on prostate cancer.Part 1:screening,diagnosis,and treatment of clinically localized disease.Eur Urol 2011;59:61-71.
[4]Mullins JK,Feng Z,Trock BJ,Epstein JI,Walsh PC,Loeb S.The impact of anatomical radical prostatectomy on cancer control:the 30-year anniversary.J Urol 2012;188:2219-24.
[5]Montorsi F,Wilson TG,Rosen RC,Ahlering TE,Artibani W, Carrol PR,et al.,Pasadena Consensus Panel.Best practices in robot-assisted radical prostatectomy:recommendations of the Pasadena Consensus Panel.Eur Urol 2012;62:368-81.
[6]Ni Choileain N,Redmond HP.Cell response to surgery.Arch Surg 2006;141:1132-40.
[7]Chrousos GP,Gold PW.The concepts of stress and stress system disorders.Overview of physical and behavioral homeostasis.JAMA 1992;267:1244-52.
[8]Tsigos C,Chrousos GP.Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress.J Psychosom Res 2002;53: 865-71.
[9]Gibbison B,Angelini GD,Lightman L.Dynamic output and control of the hypothalamic-pituitary-adrenal axis in critical illness and major surgery.Br J Anesth 2013;111:347-60.
[10]Fracalanza S,Ficarra V,Cavalleri S,Galfano A,Novara G, Mangano A,et al.Is robotically assisted laparoscopic radically prostatectomy less invasive than retropubic radical prostatectomy?Results from a prospective,unrandomized, comparative study.BJU Int 2008;101:1145-9.
[11]Menon M,Tewari A,Peabody J,The VIP Team.Vattikuti Institute prostatectomy:technique.J Urol 2003;169:2289-92.
[12]Walsh PC.Anatomic radical retropubic prostatectomy.In: Walsh PC,Retik AB,Vaughan ED,Wein AJ,editors.Campbell’s urology.8th ed.Philadelphia:WB Saunders;2002.p.3107-29.
[13]D’Amico AV,Whittington R,Malkowicz SB,Shultz D,Blank K, Broderick GA,et al.Biochemical outcome after radical prostatectomy,external beam radiation therapy,or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998;280:969-74.
[14]Briganti A,Larcher A,Abdollah F,Capitanio U,Gallina A, Suardi N,et al.Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection:the essential importance of percentage of positive cores.Eur Urol 2012;61:480-7.
[15]Dripps RD,Lamont A,Eckenhoff J.The role of anesthesia in surgical mortality.JAMA 1961;178:261-3.
[16]Dindo D,Demartines N,Clavien PA.Classification of surgical complications.A new proposal with evaluation in a cohort of 6336 patients and results of a survey.Ann Surg 2004;240: 205-13.
[17]Flemming ID,Cooper JS,Henson DE,Hutte RVP,Kennedy BJ, Murphy GP,et al.,editors.American Joint Committee on Cancer Staging Manual.5th ed.Philadelphia:JP Lippincott; 1997.p.219-22.
[18]Roberts FS,Roberts WL.Performance characteristics of five automated serum cortisol immunoassays.Clin Biochem 2004; 37:489-93.
[19]Eisold S,Mehrabi A,Konstantinidis L,Mieth M,Hinz H, KashfiA,et al.Experimental study of cardiorespiratory stress factors in esophageal surgery using robot-assisted thoracoscopic or open thoracic approach.Arch Surg 2008;143: 156-63.
[20]Porcaro AB,Molinari A,Terrin A,De Luyk N,Bldassarre R, Brunelli M,et al.Robotic-assisted radical prostatectomy is less stressful than the open approach:results of a contemporary prospective study evaluating pathophysiology of cortisol stress-related kinetics in prostate cancer surgery.J Robot Surg 2015;9:249-55.
Received 3 September 2015;received in revised form 4 January 2016;accepted 3 March 2016
Available online 14 March 2016
*Corresponding author.
E-mail address:drporcaro@yahoo.com(A.B.Porcaro).
Peer review under responsibility of Second Military Medical University.
http://dx.doi.org/10.1016/j.ajur.2016.03.002
2214-3882/ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
猜你喜欢
大众文艺(2022年23期)2022-12-25
中学生数理化·八年级物理人教版(2022年5期)2022-06-05
中学生数理化·八年级物理人教版(2022年6期)2022-06-05
中国品牌(2021年7期)2021-08-09
中学生数理化·中考版(2020年11期)2020-12-14
少儿美术(快乐历史地理)(2020年4期)2020-08-24
收藏界(2018年1期)2018-10-10
商周刊(2018年12期)2018-07-11
福建茶叶(2018年4期)2018-01-19
福建茶叶(2018年5期)2018-01-19
 Asian Journal of Urology2016年2期
Asian Journal of Urology2016年2期
- Asian Journal of Urology的其它文章
- Prostate specific antigen bounce after intensity-modulated radiation therapy in an Asian population
- Advances in prostate cancer research models:From transgenic mice to tumor xenografting models
- Major histocompatibility complex I upregulation in clear cell renal cell carcinoma is associated with increased survival
- Risk factors for fever and sepsis after percutaneous nephrolithotomy
- Glass ampoule in urinary bladder as a foreign body
- Pediatric fibrous pseudotumor of the tunica vaginalis testis