
克罗米芬与定坤丹对PCOS不孕症临床促排卵和临床妊娠疗效的研究
2017-11-11 07:43陈兰谈勇陈淑萍
中国中药杂志 2017年20期
关键词:多囊卵巢综合征
陈兰 谈勇 陈淑萍
[摘要]评价在克罗米芬(CC)+促性腺激素(Gn)基础上,CC与定坤丹对PCOS不孕症患者临床促排卵和临床妊娠疗效的研究,为中药助孕治疗提供思路和方法。选择2015年10月1日—2017年4月23日在江苏省中医院生殖医学科门诊行促排卵治疗的PCOS不孕症患者60例。按随机数字表法分为A组[CC+Gn+人绒毛膜促性腺激素(HCG)]和B组(CC+Gn+定坤丹)。观察周期排卵率、周期取消率、周期妊娠率、累积妊娠率、排卵日子宫内膜厚度、Gn使用天数和总用量、未破裂卵泡黄素化综合征(LUFS)及卵巢过度刺激综合征(OHSS)发生率。A组的周期排卵率、周期妊娠率、累积妊娠率及排卵日子宫内膜厚度均小于B组,而周期取消率、Gn使用天数及总用量均大于B组,且差异均具有统计学意义(P<005)。该研究未出现1例LUFS或OHSS。CC与定坤丹对PCOS不孕症患者具有促排效应,且CC+Gn+定坤丹联合促排方案能显著提高临床妊娠率。
[关键词]定坤丹; 多囊卵巢综合征; 克罗米芬
[Abstract]The evaluation is based on clomiphene citrate (CC)+gonadotropin (Gn), clinical study on CC and Dingkun Dan′s treatment on ovulation induction and clinical pregnancy effect of PCOS, and to provide ideas and methods for traditional Chinese medicine assisted reproductive treatment This study selected 60 PCOS infertility patients treated with ovulation induction in reproductive medicine clinic, Jiangsu Province Hospital of traditional Chinese medicine during 20151001—20170423 They were randomly divided into two groups: Group A (CC+Gn+HCG) and Group B (CC+Gn+Dingkun Dan) These results were observed and compared including cycle ovulation rate, cycle cancellation rate, cycle pregnancy rate, cumulative pregnancy rate, endometrial thickness, duration of Gn, total amount of Gn, the occurring rate of luteinized unruptured follicle syndrome and ovarian hyperstimulation syndrome Group A had lower cycle ovulation rate, cycle pregnancy rate, cumulative pregnancy rate and endometrial thickness, compared with Group B, the difference was statistically significant(P<005) However, Group A had higher cycle cancellation rate, duration of Gn and total amount of Gn, compared with Group B, the difference was statistically significant(P<005) In this study, no case of LUFS or OHSS was found in all patients CC and Dingkun Dan had the effect of promoting ovulation on PCOS infertility patients, and CC+Gn+Dingkun Dan could elevate clinical pregnancy rate.
[Key words]Dingkun Dan; polycystic ovary syndrome; clomiphene citrate
多囊卵巢綜合征(polycystic ovary syndrome,PCOS)是一种以慢性无排卵、临床/生化高雄激素血症、多囊卵巢(polycystic ovaries,PCO)和胰岛素抵抗(insulin resistance,IR)为特征的妇科常见病[1]。PCOS与月经失调、不孕及早期妊娠丢失相关,并且成为女性不孕最常见的原因[23]。笔者运用定坤丹对PCOS不孕症患者进行促排卵治疗,取得较好疗效,现将结果报道如下。
1资料与方法
11PCOS的诊断标准参照2003年鹿特丹ESHRE/ASRM资助的PCOS协商研讨组修订的PCOS诊断标准[4]:①稀发排卵或无排卵;②高雄激素血症的临床和/或生化体征;③多囊卵巢(PCO:每侧卵巢含有至少12个直径2~9 mm的卵泡,和/或卵巢体积>10 mL。卵巢体积的计算方法为05×卵巢长×宽×厚)。以上3条中具备2条即可。并需排除先天性肾上腺增生、分泌雄激素的肿瘤、库欣综合征等疾病。不孕症参照《妇产科学》诊断标准:女性未避孕,正常性生活至少12个月而未孕。
12纳入标准①符合PCOS及不孕症诊断标准;②研究前中西药结合对症基础治疗≥3个月;③2个自然周期阴道B超或BBT监测均显示排卵异常;④子宫输卵管碘油造影检查或宫、腹腔镜检查证实至少一侧输卵管通畅;⑤配偶精液常规检查正常;⑥自愿签署知情同意书。endprint
13排除标准①其他原因所致的与PCOS临床和内分泌征象相仿的疾病,如卵泡膜细胞增殖症、卵巢或肾上腺肿瘤、肾上腺皮质增生症等;②阴道B超检查有子宫畸形,子宫肌瘤及附件包块;③其他原因导致的不孕;④患有严重的遗传、躯体疾病或精神心理疾患;⑤接触致畸量的射线、毒物、药物并处于作用期;⑥月经周期第2~4天卵巢有≥10 mm的无回声区;⑦本研究药物过敏者。
14一般资料选择2015年10月1日—2017年4月23日在江苏省中医院生殖医学科门诊行促排卵治疗的PCOS不孕症患者60例。本研究经南京中医药大学附属医院江苏省中医院伦理委员会批准。
15治疗方法A组:克罗米芬(clomiphene citrate,CC)+促性腺激素(gonadotropin,Gn)+人绒毛膜促性腺激素(human chorionic gonadotropin,HCG),从月经或撤退性出血第2~5天开始使用CC(高特制药有限公司,批准文号H20140688,50 mg/片),每次50~100 mg,每日1次,连续服用5 d。根据卵泡发育情况使用Gn[人绝经尿促性素(human menopausal gonadotropin,HMG)乐宝得,丽珠集团,批准文号H10940097,75 IU/支或丽申宝,丽珠集团,批准文号H20052130,75 IU/支],每次75 IU,每日1次。周期第9天经阴道B超对卵泡及子宫内膜连续监测,当最大卵泡直径≥16~18 mm,当日肌肉注射HCG(丽珠集团,批准文号H44020668,5 000 U/支)5 000~1万 U,指导患者隔日性交1次。
B组:CC+Gn+定坤丹,CC及Gn使用与A组相同。定坤丹由红参、鹿茸、西红花、三七、白芍、熟地黄、当归、白术、枸杞子、黄芩、香附、茺蔚子、川芎、鹿角霜、阿胶、延胡索等组成(山西广誉远国药有限公司生产,批准文号国药准字Z14020656,108 g/丸)口服,每次1丸,每天2次,从月经或撤退性出血第8天开始服药,连续服用7 d。周期第9天经阴道B超对卵泡及子宫内膜连续监测,当最大卵泡直径≥16~18 mm,指导患者隔日性交,直至排卵或已超出预计排卵日1周且阴道B超监测卵泡异常增大或已明显缩小。
所有患者排卵后给予地屈孕酮(Abbott,批准文号H20130110,10 mg/片)40 mg·d-1,口服。排卵后14 d测血βHCG或尿HCG,排卵后35 d阴道B超看到子宫腔内有妊娠囊及胎心搏动为临床妊娠。
16觀察指标观察周期排卵率、周期取消率、周期妊娠率、累积妊娠率、排卵日子宫内膜厚度、Gn使用天数、Gn总用量、未破裂卵泡黄素化综合征(luteinized unruptured follicle syndrome,LUFS)及卵巢过度刺激综合征(ovarian hyperstimulation syndrome,OHSS)发生率等。
17疗效判定标准及内容①痊愈:尿HCG或血βHCG阳性,阴道B超检查显示孕囊和胎心搏动为临床妊娠;②有效:治疗周期中阴道B超检测,有排卵但未受孕;③无效:治疗周期中阴道B 超检测,无优势卵泡。
18统计学方法用SPSS 210软件进行统计学分析,计量资料以±s表示,对各组变量进行正态性检验,对非正态性数据经变换进一步分析,各组样本均数比较采用单因素方差分析,两两比较采用LSD法;以P<005为差异有统计学意义,P<001为差异有显著统计学意义。
2结果
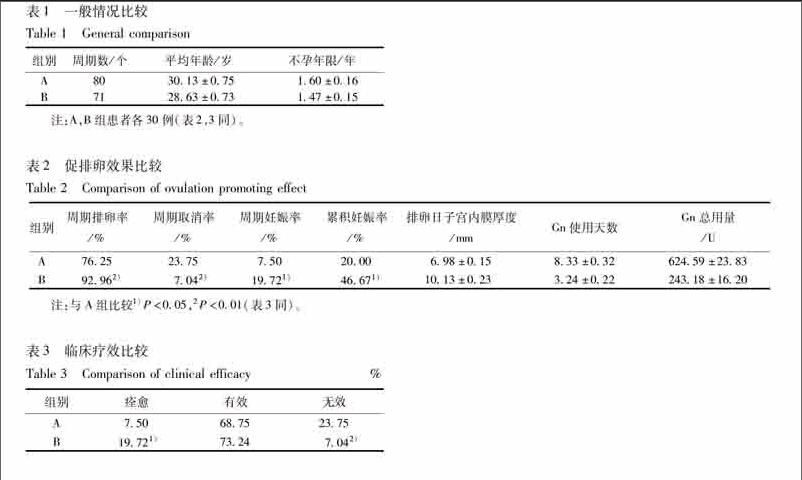
21一般情况比较纳入的受试者按随机数字表法分A,B 2组,每组30例。2组患者年龄、不孕年限比较差异无统计学意义(表1)。
22促排卵效果比较A组的周期排卵率、周期妊娠率、累积妊娠率及排卵日子宫内膜厚度均小于B组,而周期取消率、Gn使用天数及总用量均大于B组,且差异均具有统计学意义(P<005)。本研究未出现LUFS或OHSS(表2)。
23临床疗效比较B组的痊愈率高于A组,而无效率低于A组,且差异均具有统计学意义(P<005)(表3)。
24安全性评估2组患者治疗后进行血、尿常规及肝肾功能检查均未见明显异常。
3讨论
目前推荐CC作为PCOS相关性不孕症的主要治疗方法,其具有排卵率高、多胎妊娠风险适中、治疗简单价廉等优点[5],并且CC治疗PCOS患者的妊娠率与HCG日优势卵泡大小无关[6]。虽然CC是PCOS的一线治疗用药,但是大约15%~40% PCOS患者对CC抵抗[7]。有许多因素可以预测CC诱导排卵的效果,如体重指数(body mass index,BMI)、总睾酮(total testosterone,TT)、抗苗勒氏管激素(anti mullerian hormone,AMH)、卵巢体积、卵巢间质动脉搏动指数、内脏脂肪面积、促炎性细胞因子等[78]。Xi W等[9]研究发现小窦状卵泡合成的AMH[10]是PCOS患者CC促排卵最有效的预测因子,且当AMH为777 mg·L-1时预测特异性达92%,敏感性达65%。而Vaiarelli A等[11]却认为AMH的预测作用非常有限。在CC治疗前通过改变生活方式(包括限制热量的摄入、减肥药物、行为矫正、运动)和/或连续口服避孕药可以提高促排卵的效果[12]。Paulson M等[13]研究也发现通过饮食管理与体育锻炼能显著提供CC的促排效果。而Foroozanfard F等[14]通过给予超重或肥胖的PCOS患者连续12周以水果、蔬菜、全谷物、低脂肪乳制品为主的饮食治疗显著提高CC的促排卵率。Ding N等[15]研究发现黄体晚期及早卵泡期CC对PCOS患者的促排效果更佳,Elbohoty A E等[16]的研究亦得出相似的结论。
Gn作为二线治疗用药[17]。Birch Petersen K等[5]通过对PCOS患者单排卵的临床研究发现,低剂量Gn递增方案对PCOS患者有高效的促排效果,尤其在生活方式干预治疗后。Hassan A等[18]研究也发现Gn对CC抵抗的PCOS患者有较好的促排效果,但成本较高。而且Gn促排更容易发生OHSS和卵巢囊肿,因此Salaheldin AbdelHamid A M等[19]建议用CC递增方案替代Gn。endprint
本研究发现,B组(CC+Gn+定坤丹)的周期排卵率显著高于A组(CC+Gn +HCG)(P<001),说明定坤丹不仅具有促进卵泡排出的作用而且其效果优于HCG。同时B组周期取消率、Gn使用天数及总用量均显著低于A组(P<001),說明CC+Gn+定坤丹用于PCOS患者促排卵治疗较目前临床常用的CC+Gn+HCG更佳经济省时。宋玉荣等[20]研究发现定坤丹对于多囊卵巢模型大鼠有促排卵作用,其机制可能通过调节下丘脑垂体卵巢轴,降低黄体生成素(luteinizing hormone,LH)及睾酮(testosterone,T),升高卵泡刺激素(folliclestimulating hormone,FSH),抑制卵巢血管内皮生长因子(vascular endothelial growth factor,VEGF)表达,抑制卵巢新生血管形成,改善卵巢血流,提高卵泡质量,促进卵巢排卵。
本研究还发现,B组(CC+Gn+定坤丹)的排卵日子宫内膜厚度大于A组(CC+Gn+HCG)(P<001)。易星星等[21]研究发现定坤丹与戊酸雌二醇均可使患者子宫内膜增厚,但在增加月经量、改善临床症状及总疗效方面,定坤丹更具优势。而且定坤丹具有提高子宫内膜容受性作用,机制可能与改善大鼠体内激素分泌、降低T、上调同源框蛋白A10(homeobox protein A10,HOXA10)表达有关[20]。这可能是B组妊娠率高于A组的可能机制之一。
定坤丹始于清代乾隆年间,虽有几百年的历史,但有关研究在最近几十年才逐渐增多[22]。李启佳等[23]应用红外热成像技术发现定坤丹靶向药效集中在生殖相关区域。本研究旨在为PCOS不孕症患者提供一个既简单方便、安全有效,又经济省时的促排方案,并为中药助孕治疗提供思路和方法。但是由于样本量有限,因此尚需进一步扩大样本量以验证其疗效与安全性,更需要进一步摸索合适的用药量及用药时间,以期达到更佳的临床疗效。
[参考文献]
[1]Wang L, Qi H, Baker P N, et al Altered circulating inflammatory cytokines are associated with anovulatory polycystic ovary syndrome (PCOS) women resistant to clomiphene citrate treatment [J]. Med Sci Monit, 2017, 23:1083.
[2]Su Y, Wu J, He J, et al High insulin impaired ovarian function in early pregnant mice and the role of autophagy in this process [J]. Endocr J, 2017, doi: 101507/endocrjEJ160494.
[3]Brüggmann D, Berges L, Klingelhfer D, et al Polycystic ovary syndrome: analysis of the global research architecture using density equalizing mapping [J]. Reprod Biomed Online, 2017, doi: 101016/jrbmo201703010.
[4]The Rotterdam ESHER/ASRMSponsored Pcos Work Shop GroupRevised 2003 consensus on diagnostic criteria and long termheal thrisks related to polycystic ovary syndrome [J]. Fertil Steril, 2004, 81(1): 19.
[5]Birch Petersen K, Pedersen N G, Pedersen A T, et al Monoovulation in women with polycystic ovary syndrome: a clinical review on ovulation induction [J]. Reprod Biomed Online, 2016, 32(6):563.
[6]Seckin B, Pekcan M K, Bostanc E I, et al Comparison of pregnancy rates in PCOS patients undergoing clomiphene citrate and IUI treatment with different leading follicular sizes [J]. Arch Gynecol Obstet, 2016, 293(4):901.
[7]Azziz R Introduction: determinants of polycystic ovary syndrome [J]. Fertil Steril, 2016, 106(1):4.
[8]Ellakwa H E, Sanad Z F, Hamza H A, et al Predictors of patient responses to ovulation induction with clomiphene citrate in patients with polycystic ovary syndrome experiencing infertility [J]. Int J Gynaecol Obstet, 2016, 133(1):59.endprint
[9]Xi W, Yang Y, Mao H, et al Circulating antimullerian hormone as predictor of ovarian response to clomiphene citrate in women with polycystic ovary syndrome [J]. J Ovarian Res, 2016, doi: 101186/s1304801602142.
[10]Bani Mohammad M, Majdi Seghinsara A Polycystic ovary syndrome (PCOS), diagnostic criteria, and AMH [J]. Asian Pac J Cancer Prev, 2017, 18(1):17.
[11]Vaiarelli A, Drakopoulos P, Blockeel C, et al Limited ability of circulating antiMüllerian hormone to predict dominant follicular recruitment in PCOS women treated with clomiphene citrate: a comparison of two different assays [J]. Gynecol Endocrinol, 2016, 32(3):227.
[12]Legro R S, Dodson W C, Kunselman A R, et al Benefit of delayed fertility therapy with preconception weight loss over immediate therapy in obese women with PCOS [J]. J Clin Endocrinol Metab, 2016, 101(7):2658.
[13]Paulson M, Sahlin L, Hirschberg A L Progesterone receptors and proliferation of the endometrium in obese women with polycystic ovary syndromea lifestyle intervention study [J]. J Clin Endocrinol Metab, 2016, doi: 101210/jc20163155.
[14]Foroozanfard F, Rafiei H, Samimi M, et al The effects of DASH diet on weight loss, antiMüllerian hormone and metabolic profiles in women with polycystic ovary syndrome: a randomized clinical trial [J]. Clin Endocrinol (Oxf), 2017, doi: 101111/cen13333.
[15]Ding N, Chang J, Jian Q, et al Luteal phase clomiphene citrate for ovulation induction in women with polycystic ovary syndrome: a systematic review and Metaanalysis [J]. Gynecol Endocrinol, 2016, 32(11):866.
[16]Elbohoty A E, Amer M, Abdelmoaz M Clomiphene citrate before and after withdrawal bleeding for induction of ovulation in women with polycystic ovary syndrome: randomized crossover trial [J]. J Obstet Gynaecol Res, 2016, 42(8):966.
[17]Balen A H, Morley L C, Misso M, et al The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance [J]. Hum Reprod Update, 2016,22(6):687.
[18]Hassan A, Shehata N, Wahba A Cost effectiveness of letrozole and purified urinary FSH in treating women with clomiphene citrateresistant polycystic ovarian syndrome: a randomized controlled trial [J]. Hum Fertil (Camb), 2017,20(1):37.
[19]Salaheldin AbdelHamid A M, Rateb A M, Ismail Madkour W A Is clomiphene citrate stairstep protocol a good alternative to gonadotrophins in clomipheneresistant PCO patients prospective study [J]. J Obstet Gynaecol Res, 2016,42(5):547.
[20]宋玉榮,王文艳,卫兵 定坤丹对多囊卵巢模型大鼠生殖功能的影响[J]. 安徽医科大学学报,2016,51(10):1473.
[21]易星星,林洁 定坤丹治疗肾虚肝郁证月经过少患者30例临床观察[J]. 中国中西医结合杂志,2016,36(5):629.
[22]陈燕霞,马堃 定坤丹临床应用的系统评价[J]. 中国中药杂志,2015,40(20):3916.
[23]李启佳,陆华,刘影应用红外热成像技术评价定坤丹靶向药效[J]. 中成药,2016,38(12):2560
[责任编辑张燕]endprint
猜你喜欢
中国当代医药(2016年29期)2017-01-03
中国实用医药(2016年30期)2016-12-28
家庭用药(2016年9期)2016-12-03
中国实用医药(2016年27期)2016-11-30
中国实用医药(2016年27期)2016-11-30
云南中医中药杂志(2016年9期)2016-11-29
云南中医中药杂志(2016年9期)2016-11-29
中国现代医生(2016年26期)2016-11-28
