
Age-related changes in proprioception of the ankle complex across the lifespan
2019-11-21 01:18NanYangGordonWaddingtonRogerAdamsJiaHan
Nan Yang ,Gordon Waddington ,Roger Adams ,Jia Han ,c,d,*
a School of International Education,Shanghai University of Sport,Shanghai 200438,China b Research Institute for Sports and Exercise,University of Canberra,Canberra,ACT 2600,Australia c Faculty of Health,Arts and Design,Swinburne University of Technology,Sydney,VIC 3122,Australia d School of Kinesiology,Shanghai University of Sport,Shanghai 200438,China Received 6 September 2018;revised 12 December 2018;accepted 7 March 2019 Available online 15 June 2019
Abstract Background:Ankle complex proprioceptive ability,needed in active human movement,may change from childhood to elderly adulthood;however,its development across all life stages has remained unexamined.The aim of the present study was to investigate the across-the-lifespan trend for proprioceptive ability of the ankle complex during active ankle inversion movement.Methods:The right ankles of 118 healthy right-handed participants in 6 groups were assessed:children(6-8 years old),adolescents(13-15 years old),young adults(18-25 years old),middle-aged adults(35-50 years old),old adults(60-74 years old),and very old adults(75-90 years old).While the participants were standing,their ankle complex proprioception was measured using the Active Movement Extent Discrimination Apparatus.Results:There was no significant interaction between the effects of age group and gender on ankle proprioceptive acuity(F(5,106)=0.593,p=0.705,=0.027).Simple main effects analysis showed that there was a significant main effect for age group(F(5,106)=22.521,p <0.001,η2p=0.515)but no significant main effect for gender(F(1,106)=2.283,p=0.134,η2p=0.021)between the female(0.723±0.092,mean±SD)and the male(0.712±0.083)participants.The age-group factor was associated with a significant linear downward trend in scores(F(1,106)=10.584,p=0.002,η2p=0.091)and a strong quadratic trend component(F(1,106)=100.701,p <0.001,η2p=0.480),producing an asymmetric inverted-U function.Conclusion:The test method of the Active Movement Extent Discrimination Apparatus is sensitive to age differences in ankle complex proprioception.For proprioception of the ankle complex,young adults had significantly better scores than children,adolescents,old adults,and very old adults.The middle-aged group had levels of ankle proprioceptive acuity similar to those of the young adults.The scores for males and females were not significantly different.Examination of the range of the scores in each age group highlights the possible level that ankle complex movement proprioceptive rehabilitation can reach,especially for those 75-90 years of age.2095-2546/©2019 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords:Aging;Ankle complex;Development;Motor control;Proprioception
1.Introduction
Changes in proprioception—the sensations of joint movement and joint position—that occur with increasing age have been a concern in both developmental and geriatric studies.1-4Notably,conflicting results have emerged from work on proprioceptive development at different joints. Laszlo and Bairstow5suggested that children develop adult-equivalent proprioceptive acuity in their arms by the age of 7,while Goble et al.6proposed that proprioceptive ability at the elbow joint continues to improve into adolescence.In a test of standing stability,Steindl et al.7found that mature proprioceptive function occurred by approximately 3 to 4 years of age.
Similarly,conflicting conclusions regarding the age-related decline in proprioception has been documented in several studies of geriatric people.Both Deshpande et al.8and Westlake et al.9found a significant age-related degradation in ankle proprioception when using the threshold to detect passive movement(TTDPM)test,even though they failed to find any difference between younger and older adults in the results of active or passive joint position reproduction(JPR)tests.Given the different methodologies employed,these conflicting results indicate that some test protocols(e.g.,JPR)may not be sufficiently sensitive to age-related differences.10
Since previous results from studies of proprioceptive development and degeneration are inconsistent,no studies have yet examined ankle proprioception among typically developing children and adolescents,and no studies have compared the ankle proprioceptive function of children and adolescents with that of adults,the present study set out to determine proprioceptive acuity at the ankle complex for children,adolescents,and adults of various ages.The ankle complex,including the talocrural joint,the subtalar joint,and the inferior tibiofibular joint,is the last joint before contact with the ground and thus represents the final opportunity for adjustments to be made to maintain an upright stance.The crucial role that ankle complex proprioception plays in balance control,daily activities,and mobility has been widely acknowleged.11-14Accordingly,scores for ankle-complex proprioception across the human lifespan can provide a normative base against which the proprioceptive status of pediatric and gerontology populations can be compared and,thus,can facilitate the evaluation of interventions designed to improve ankle proprioception.
Currently,much of the knowledge about age effects on ankle proprioception is based on comparisons of proprioception between 1 group of younger adults and 1 group of older adults.2,15-17In these studies,age-related deterioration in ankle proprioception has been investigated in tests of ankle position sense and/or thresholds for perception of passive movement.2,15-17Although active movement tests of proprioception are closer to the normal function of the ankle complex in daily activities,ankle complex proprioception assessed as active movement discrimination across the lifespan has not yet been investigated.In the present study,we examined proprioceptive acuity at the ankle complex among 6 age groups,ranging from children to very old adults,using a full weight-bearing active movement test:the Active Movement Extent Discrimination Assessment(AMEDA).18Unlike tests of JPR and tests for the threshold of perception of externally applied passive movement,the AMEDA assesses the ability to judge the extent of functional ankle movements made in normal weight-bearing stance with vision of the target movement obscured.This allows for an examination across the lifespan of changes in ankle complex proprioception ability in functional standing.
The primary aim of the present study was to investigate the trend across the lifespan for ankle complex proprioceptive ability,tested by active ankle inversion movements.From the perspective of physiology and use-dependent theory, we hypothesized that(1)the active movement discrimination assessment is sensitive to age differences in ankle complex proprioception, and (2) ankle complex proprioception improves throughout childhood,peaks at early adulthood,can be maintained during middle-aged adulthood,and declines in old age.The results of the current work will inform appropriate intervention at specific ages to improve or maintain proprioceptive ability across the life span.
Compared with age-related differences in ankle proprioceptive ability,gender-related differences are less commonly discussed.Ko,et al.2have compared the gender differences using 3 different proprioceptive tasks: threshold task(TTDPM),position task(JPR),and tracking task,but their results showed that men and women differed only in trackingrelated ankle proprioception tasks.To date,no studies have yet reported on gender differences using the proprioceptive task of AMEDA.Therefore,this study set it as a secondary purpose to examine the gender difference.
2.Methods
2.1.Participants
Healthy participants were recruited into 6 groups,with mean ages and ranges as follows: (1) children (n=20;7.1±0.9 years, mean ±SD; 6-8 years);(2) adolesents(n=20;14.2±0.8 years,mean±SD;13-15 years);(3)young adults(n=20;20.9±2.0 years,mean±SD;18-25 years);(4)middle-aged adults(n=20;41.2±5.0 years,mean± SD; 35-50 years); (5) older adults (n=20;66.3±4.7 years,mean±SD;60-74 years);and(6)very old adults(n=18;81.3±4.0 years,mean±SD;75-90 years).
All participants were right-handed and rigt-footed as classified by the Edinburgh Handedness Inventory(Chinese version)19,20and the Waterloo Footedness Questionnaire(Chinese version),20,21respectively.At testing,participants were screened to exclude those having neuromuscular impairment and those using psychoactive or vasoactive medications.Participants who had histories of lower limb surgery,including ankle,knee,or hip arthroplasty;pathology of either the ankle or the subtalar joint;restricted right ankle range of motion;severe arthritis of lowerextremity joints;or symptoms of central or peripheral nervous system dysfunction were also excluded.All the participants older than 60 years of age who were tested were generally physically fit and had good scores(i.e.,>26)on the Mini-mental State Examination.22Because impaired proprioception has been associated with risk of falls,23,24we excluded older adults who had fallen within the past 2 years in order to minimize the effects of fall-related proprioception changes and to obtain normal data from healthy elderly people.All participants provided written informed consent at the time of testing.If participants were younger than 18 years,written informed consent was obtained from parents.The study was approved by the Human Research Ethics Board at Shanghai University of Sport(2015012).
2.2.Active ankle complex movement proprioception assessment
2.2.1.Apparatus

Fig.1.Ankle complex active movement extent discrimination apparatus(AMEDA).(A)the start position of the test;(B)one of the 4 possible positions reached during the test with an ankle inversion movement.
Since apparatus to assess proprioception had previously been developed for judging movements made to physical stops at the wrist25and elbow,26these studies were used as the basis for the development of the ankle complex apparatus,AMEDA.27AMEDA was developed in 1990s to test proprioception of the ankle complex in full weight-bearing stance(Fig.1).This method provides ankle complex movement discrimination scores that represent participants'sensitivity to small differences in the extent of active ankle inversion.The purpose-built AMEDA apparatus consists of a fixed wooden platform housing a swinging square wooden plate that rotates around an axle aligned to the long axis of the foot being tested.During the test,participants are instructed to look straight ahead and stand astride the device in an even weight-bearing stance,with their left foot on the fixed platform and their right foot centered over the axle of the swinging plate.For each trial,participants are required to make an active ankle inversion that rotates the hinged plate from the horizontal start position downward until the rim of the hinged plate contacts the height-adjustable stop,and thereafter,to actively return the hinged plate back to the horizontal start position.The height-adjustable stop can generate 4 inversion extents from horizontal:Position 1=10°,Position 2=12°,Position 3=14°,and Position 4=16°.
2.2.2.Testing protocols
Before data collection,participants were given a familiarization session in which they experienced the 4 ankle inversion positions in order 3 times,going from the smallest(Position 1=10°)through to the largest(Position 4=16°),for 12 inversion movements in total.During the test,participants undertook 40 trials without feedback,with 10 randomly presented trials for each of the 4 different inversion displacements.With eyes directed forward at a point on the opposite wall,participants were required to identify each test ankle inversion position based on proprioceptive information and to respond with a number(1,2,3,or 4)indicating the ankle inversion position they felt that they had just experienced.Therefore,there were 4 possible responses(Numbers 1-4)that could be made to each of the 4 possible ankle inversion extents(10°,12°,14°,and 16°).The AMEDA apparatus has been tested for validity and displays sensitivity to a variety of injury and training conditions affecting active ankle complex movement proprioception.18,27High AMEDA scores on the test are related to sports achievement,in that ankle complex proprioception tested in this manner is significantly correlated with level of sports performance.11
2.3.Data analysis
A movement discrimination score was calculated for each participant to represent that individual's proprioceptive acuity at the ankle complex.To obtain this acuity score,raw data were first entered into a 4×4 matrix representing the frequency with which each response was made for each stimulus.Non-parametric signal detection analysis(SPSS Version 21.0;IBM Corp.,Armonk,NY,USA)was used to produce 3 pair-wise receiver operating characteristic(ROC)curves.28Thereafter,the mean area under the curve(AUC)was calculated using SPSS Version 21.0(IBM Corp.)to give each participant an ankle complex movement discrimination score,which provides an unbiased estimate of the ability of an individual to discriminate between adjacent pairs of stimuli.AUC values range from 0.5,equivalent to chance responding,to 1.0,representing perfect discrimination.
A two-way analysis of variance(ANOVA)was conducted using the factors of gender (male, female) and age group(6-8 years, 13-15 years, 18-25 years, 35-50 years,60-74 years,and 75-90 years).Effect sizes using partial eta squared(η2p)for the measures were included.Orthogonal polynomial trend analysis was selected to examine the ankle complex proprioception score function across the life span.Pearson correlations,with statistical significance at p <0.05,were calculated to assess the relationship between age and ankle complex movement discrimination scores.
3.Results
A two-way ANOVA was conducted to examine the effect of age group and gender on ankle complex proprioceptive acuity represented by AMEDA AUC scores.The Shapiro-Wilk test for non-normality applied to ankle complex proprioceptive acuity scores for each of the age groups showed that none of them were significantly non-normal(all p >0.22).The mean and 95%confidence intervals(CIs)for the male and female participants in each of the 6 age groups are shown in Fig.2.There was no significant interaction between the effects of age group and gender on ankle proprioceptive acuity (F (5,106)=0.593,p=0.705,η2p=0.027).Simple main effects analysis showed that there was a significant main effect for age group(F(5,106)=22.521,p <0.001,η2p=0.515).But analysis of the proprioceptive acuity scores of the 64 female participants(0.723±0.092,mean±SD)compared with the scores of the 54 males(0.712±0.083,mean±SD)showed no significant main effect of gender(F(1,106)=2.283,p=0.134,η2p=0.021).However,the age group factor was associated with 2 significant trend components:a linear downward trend in scores(F(1,106)=10.584,p=0.002,η2p=0.091)with a strong quadratic trend component(F(1,106)=100.701,p <0.001,η2p=0.480),producing an asymmetric inverted-U function.No higher-order trend component was significant(all p >0.13).Interaction analysis showed that there was no significant difference between genders in terms of these trend components in the score function across age(both p >0.79).To examine the range of scores for each age group,the lowest scores and highest scores achieved by a participant in the group are plotted with the age group mean in Fig.3.Post hoc tests indicated that the AMEDA mean AUC score of young adults was significantly greater than other 4 groups:children(p <0.001),adolescents(p <0.05),old adults(p <0.05),and very old adults(p <0.001).The AUC score of very old adults was significantly lower than the other 5 groups(all p <0.01).
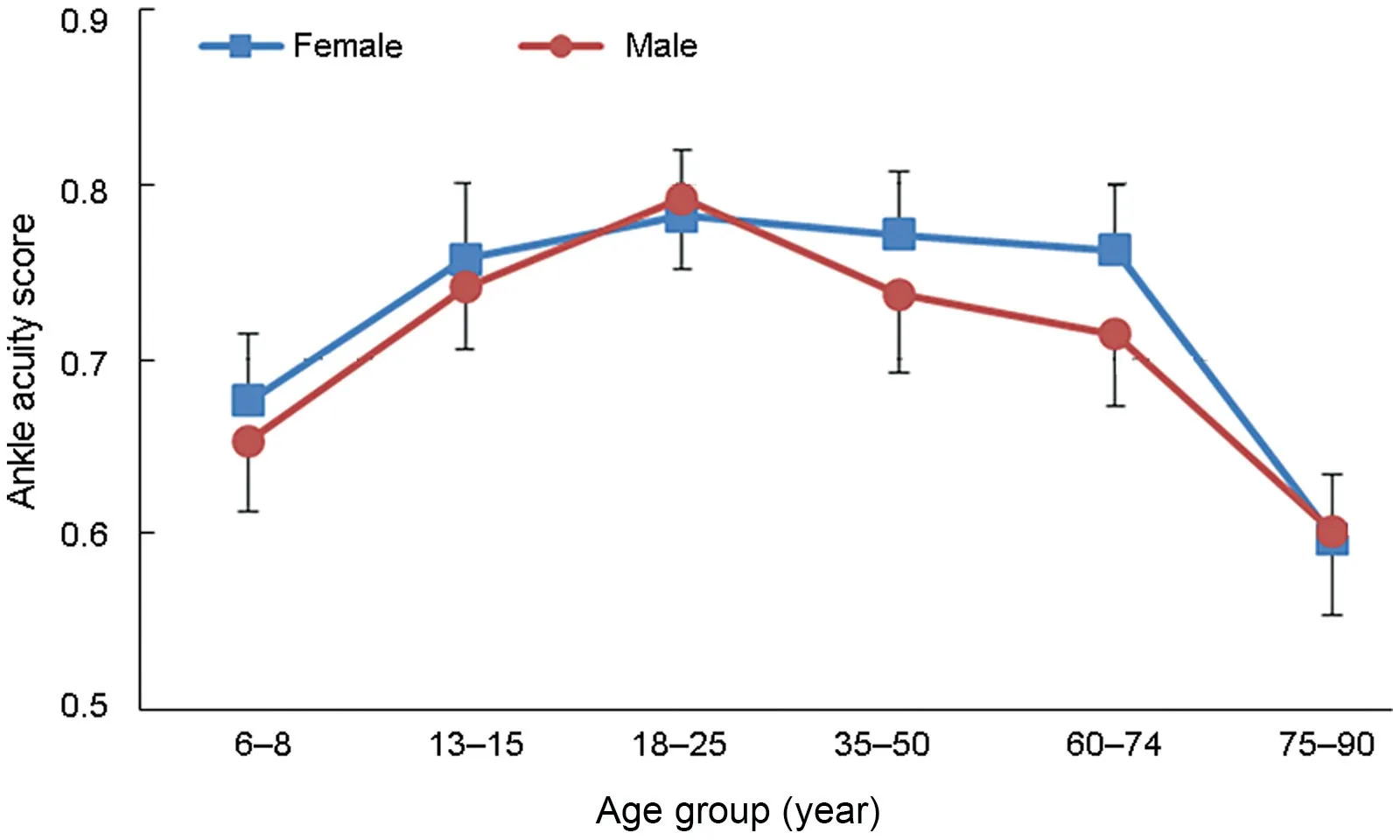
Fig.2.Curvilinear plots of ankle complex proprioceptive acuity(represented by active movement extent discrimination apparatus mean area under the curve score) and age for males and females. The error bars represent 95%confidence intervals. No significant difference between genders was identified.

Different trends are evident in the function presented in Fig.3.The mean ankle complex movement discrimination score improves from children to young adults;then scores gradually become worse and dramatically decline in older adulthood.Pearson correlation values show that from childhood to young adulthood,ankle complex movement discrimination was significantly and positively correlated with age(r=0.67,p <0.001),while from young adulthood to very old adulthood,ankle complex movement discrimination and age were significantly and negatively correlated (r = -0.65,p <0.001).
4.Discussion
In this first known study of weight-bearing ankle complex proprioceptive acuity from childhood to old age,the results were consistent with our hypothesis that the active movement discrimination assessment is sensitive to age differences in ankle complex proprioception.The results also support our hypothesis that the across-the-lifespan ankle complex proprioception in healthy participants improves from childhood to its highest level in young adulthood and then decreases from middle age to older adulthood,where proprioceptive acuity corresponds to that of the adolescents. The lowest level of proprioceptive acuity was seen in those aged 75-90 years.This function is similar to the across-the-lifespan patterns of somatosensory perception,increasing through childhood and adolescence,plateauing during adulthood,and declining in older adulthood.10
4.1.The development of ankle complex proprioception from children to young adults
The present study showed that proprioceptive acuity improved by 12.3%from childhood to adolescence and by 5.9%from adolescence to young adulthood.The peak for ankle complex proprioceptive acuity was found in the 20-to 25-year-old age group. Proprioception studies that have focused on the upper limbs of younger participants have shown a general improvement in proprioceptive ability as a function of age.6,10,29Furthermore,they have suggested that hand proprioception is substantially developed by late preschool age.5,30The difference found in developmental trends between the upper and lower limbs may be explained by the findings of Han et al.,31where proprioceptive discrimination scores from tests at the ankle complex,knee,and shoulder were found not to be correlated.The authors concluded that rather than being a general ability,the proprioception that underlies movement control is joint-specific.Thus,the function observed for ankle complex proprioceptive acuity over the lifespan may not be the same as the functions found for other joints.
Factors that might underlie proprioceptive development have been discussed in several studies.Goble et al.,6in work focused on the upper limbs,attributed the improvement seen through childhood to neural development and sensorimotor learning.These authors suggested that delayed maturation of the dorsolateral prefrontal cortex relative to sensorimotor cortical development may have contributed to the observed age-related changes in proprioceptive ability.The dorsolateral prefrontal cortex is one of the last brain regions to mature and plays a critical role in cognitive processes,such as working memory and sensory attention.32The ability to attend to the proprioceptive feedback mediating limb position awareness,as well as to generate and remember an internal model of limb position,depends on executive functions typically ascribed to the prefrontal cortex.Thus,the early developmental changes in proprioceptive ability observed in the present study most likely reflect maturation of more general cognitive abilities as well as experiential enhancement of sensorimotor processing.
4.2.Deterioration of ankle complex proprioception in adults
Young adults tested in the present study demonstrated peak proprioceptive acuity,and their ankle complex proprioception was significantly better than that of old adults and very old adults. The results showed that proprioceptive acuity decreased by 3.7%in middle-aged adults relative to young adults,2.3%in old adults relative to middle-aged adults,and 19.2%in very old adults relative to old adults.The general decline in ankle complex proprioception from younger to older adults observed in the present study is consistent with the findings of a straight-line decline obtained in other 2-group studies with at least a 40-year separation between groups.Those studies examined age-related differences in ankle complex proprioception using the following different testing protocols:active joint poition sense(JPS),33passive JPS,9dynamic JPS,16threshold for detection of passive movement,9and threshold for velocity discrimination.9However,the use in the present study of 6 age groups,with participants ranging from 6 to 90 years old,enables us,for the first time,to observe a function for ankle complex proprioception across the lifespan.Previous work has been limited to showing a straight-line decline in proprioception between 2 age groups separated by a 40-year gap.Because they used only 2 age groups,such studies were not sufficiently sensitive to determine the shape of the function across the lifespan.
In the present study,the AMEDA score found for middleaged adults indicated that proprioceptive acuity may be relatively well maintained from young adulthood until middle age.Thereafter,a sharp downturn appeared,with participants aged 75-90 years showing the worst proprioceptive sensitivity.This is consistent with reports of more frequent falling in this age cohort.34
The decline in proprioceptive acuity in elderly people can be seen to be a result of changes in the central nervous system and peripheral nervous system.3At the central level,normal aging may affect the conductive function of central somatosensory pathways35and induce neurochemical changes in the brain36and the progressive loss of the dendrite system in the motor cortex.37Recent neuroimaging studies in older adults have related decreased proprioceptive function to decreased right-sided subcortical activity and structural changes,most notably in the right putamen.This suggests that proprioceptive processing in the elderly is influenced by structural differences that limit activation within subcortical regions(i.e.,the putamen),which in turn influence performance in tests of JPS.38Previous studies have also suggested that decreased attention,memory,and cognitive resources in older adults can compromise their proprioceptive acuity compared to that of younger adults.39Age-related declines in cognitive processing ability are also thought to contribute to changes in proprioceptive function,especially in more cognitively demanding tasks.4Therefore,structural and functional changes at the central level may underlie the decrease in proprioceptive performance in older adults that was found in the current study.
Deterioration with age in cutaneous sensitivity may also contribute to the age-related decline observed in ankle complex proprioceptive performance.The cutaneous mechanoreceptors on the plantar surface of the foot can deliver information about the site and force of weight-bearing activities.40,41Several studies have noted a decline in plantar perceptual sensitivity that accompanies aging40,42,43and have confirmed that age-related anatomic and physiologic changes can reduce the sensitivity of the human foot sole.In the weight-bearing test used in the present study,cutaneous receptors in the skin around the sole of the foot provided critical tactile information that contributes to proprioceptive task performance.Therefore,the age-related decline in ankle complex proprioceptive performance observed in the present study may be attributed in part to the aging degradation of the tactile acuity in plantar skin.Because the ankle complex AMEDA test is conducted in a weight-bearing context,the information sources used during the test would include both proprioception and touch.44Thus,it is of note that 2-point touch discrimination also declines from early adulthood to older adulthood42and that plantar sole sensitivity similarly declines.43
4.3.Gender difference in ankle complex proprioception
Results in the present study showed that there is no gender difference in ankle complex proprioception when measured by the proprioceptive task of AMEDA.This result is similar to the findings observed in the study by Ko et al.,2in which no gender difference was identified in proprioception at the ankle with the proprioceptive tasks of TTDPM and JPR.However,controversies may be found in studies testing different joints or using different tasks.Nagai et al.45showed gender difference in knee proprioception in internal rotation but not in external rotation when they assessed the precision of knee internal/external rotation using the method of TTDPM.Similar gender difference was identified by Muaidi46when he assessed gender differences in rotation proprioception at knee joints using the absolute judgment task.However,Lee et al.,47who also used the method of TTDPM to evaluate pivoting proprioceptive acuity,found that when compared to males,females had significantly lower proprioceptive acuity under weightbearing in both internal and external pivoting directions.In another study,Millar et al.48assessed JPR by reproducing a single-leg squat in both adolescents and adults but found no differences between the genders.All these findings may suggest that testing tasks and tested joints can greatly affect the results,which means that further studies are needed to compare the gender differences in proprioception at different joints and with different tasks to have a full understanding of gender effect in proprioceptive performance.
4.4.Study limitations
Although statistically significant correlations were found between age and proprioceptive acuity scores in this research,our understanding of the effects of age on ankle complex proprioception is limited by the cross-sectional design of the present study and the number of participants in each age group.Longitudinal studies and larger sample sizes would be more definitive for determining the relationship between age and ankle complex proprioceptive ability.In addition,the results of this research can be generalized only to a relatively healthy,independently ambulatory population.Ankle complex proprioception is most likely worse in the older age group of the general population than reported here because older individuals who had fallen were excluded from our study,and some of the excluded individuals may have fallen due to deficient proprioception.Furthermore,regular physical activity is believed to contribute to the preservation of functional capacity;49therefore,future studies should investigate the effects of physical activity levels or mobility impairments on the maintenance of ankle complex proprioceptive acuity and examine the contribution of ankle complex proprioception to balance control in older adults.Finally,the proprioception findings in this study are limited to active inversion movement at the ankle complex.Proprioceptive performance in the movements of eversion,plantarflexion,and dorsiflexion is also important,as is proprioception loss in those movements because it relates to postural balance.Future research should include other movements in order to provide clinicians with additional information about age-related lower extremity proprioception changes and the role of ankle complex proprioception in balance control.
5.Conclusion
In the present study,ankle complex proprioceptive acuity across age was examined by using the AMEDA in a cross-sectional experimental approach.Data obtained here indicate that the AMEDA is sensitive to age differences in ankle complex proprioception and can be recommended for proprioception tests involving both children and adults. An inverted-U,across-the-lifespan pattern of change in ankle complex proprioception in healthy participants was established,in which proprioception progressed from a comparatively low level during childhood to its highest level in young adulthood.It then decreased from middle age to older age,when proprioceptive acuity corresponded to that of the adolescent participants.The reduction in proprioceptive ability observed in people 75-90 years of age suggests that targeting interventions to arrest this decline in proprioceptive acuity may be useful in areas such as fall prevention.
Acknowledgments
This work was supported by the Shanghai Shuguang Program(Grant number 16SG45),National Natural Science Foundation of China(Grant number 31870936),and China Ministry of Education Humanities and Social Science Project(Grant number 18YJA890006).It was also supported by the Program for Professors of Special Appointment(Eastern Scholar)at the Shanghai Institution of Higher Learning(TP2017062).
Authors’contributions
While conducting this study,NY played a role in conceiving and designing the study,collecting,analyzing and interpreting the data,writing the draft,and reviewing and editing the manuscript;GW played a role in conceiving and designing the study and reviewing and editing the manuscript;RA played a role in conceiving and designing the study,analyzing and interpreting the data,and reviewing and editing the manuscript;JH played a role in conceiving and designing the study,collecting the data,and reviewing and editing the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
 Journal of Sport and Health Science2019年6期
Journal of Sport and Health Science2019年6期
- Journal of Sport and Health Science的其它文章
- Physical activity and the prevention of chronic illness in the BRICS nations:Issues relating to gender equality
- The impact of health expenditures on public health in BRICS nations
- If you are physically fit,you will live a longer and healthier life:An interview with Dr.Steven N.Blair
- Variability:Human nature and its impact on measurement and statistical analysis
- Differences in transportation and leisure physical activity by neighborhood design controlling for residential choice
- Gender differences in nonlinear motor performance following concussion