
Clinical distribution and molecular profiling on postoperative colorectal cancer patients with different traditional Chinese medicine syndromes
2020-01-15 01:57LiJunJinYingLiuMingMingZhangXueMengHanQiuJieLiYuXiangBingTaoZhaiPengChenXiaYingChenWenGangWangShuiPingLiuDuanTingJiaoFengTianXieXinBingSui2
Traditional Medicine Research 2020年1期
Li-Jun Jin, Ying Liu, Ming-Ming Zhang, Xue-Meng Han, Qiu-Jie Li, Yu Xiang, Bing-Tao Zhai, Peng Chen, Xia-Ying Chen, Wen-Gang Wang, Shui-Ping Liu, Duan Ting, Jiao Feng, Tian Xie, 4, *, Xin-Bing Sui2, , 4, *
Clinical distribution and molecular profiling on postoperative colorectal cancer patients with different traditional Chinese medicine syndromes
Li-Jun Jin1, #, Ying Liu2, #, Ming-Ming Zhang3, Xue-Meng Han3, Qiu-Jie Li3, Yu Xiang3, Bing-Tao Zhai3, Peng Chen3, Xia-Ying Chen3, Wen-Gang Wang3, Shui-Ping Liu3, Duan Ting3, Jiao Feng3, Tian Xie3, 4, *, Xin-Bing Sui2, 3, 4, *
1Department of Traditional Chinese Medicine, Hangzhou Jianggan District People’s Hospital, Hangzhou, China.2Department of Medical Oncology, Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University, Hangzhou, China.3Holistic Integrative Pharmacy Institutes and Comprehensive Cancer Diagnosis and Treatment Center, the Affiliated Hospital of Hangzhou Normal University, College of Medicine, Hangzhou Normal University, Hangzhou, China.4Key Laboratory of Elemene Class Anti-cancer Chinese Medicine of Zhejiang Province and Engineering Laboratory of Development and Application of Traditional Chinese Medicine from Zhejiang Province, Hangzhou Normal University, Hangzhou, China.
Traditional Chinese medicine (TCM) syndrome, also named syndrome, are comprehensive and integral analyses of clinical information which helps to guide different individualized treatment prescriptions.Thirty healthy controls and 80 colorectal cancer (CRC) patients (including 33 Spleen Qi Deficiency syndrome, 23 Dampness Heat syndrome, 17 Blood Stasis syndrome and 7 other syndrome) were enrolled into this study. Human mRNAs were extracted from peripheral blood mononuclear cells. The gene expression for CRC patients with different TCM syndrome was determined by microarray and qRT-PCR.Spleen Qi Deficiency, Dampness Heat and Blood Stasis were the most common syndromes in CRC patients. There is a significant difference was found in mRNA expression levels (especially for,,and) among Spleen Qi Deficiency, Dampness Heat and Blood Stasis syndrome groups. The higher mRNA levels of,,,,,,,,,,and the lower expression of inflammatory cytokinewere found in Spleen Qi Deficiency group but not other syndrome types. The higher mRNA levels of,,,,,,,,,,and some inflammatory cytokines (,,,) were found in Dampness Heat group but not other syndrome types. Blood Stasis syndrome showed higher expression of,,,,,and, and lower mRNA levels of,,,,and. The CRC patients with Dampness Heat syndrome might have a poor prognosis than other syndrome types.The identification of syndrome conditions had different impacts on CRC prognosis, and which might be related with different mRNA expression levels. Some oncogenes and pro-inflammatory cytokines were highly expressed in Dampness Heat group but not other syndrome types, suggesting that the CRC patients with Dampness Heat syndrome might have a poor prognosis. Our results prelimitarily uncovered the molecular basis of syndrome differences in CRC prognosis, a better understanding for TCM treatment of CRC.
Traditional Chinese medicine, Clinical distribution, Molecular profiling, Colorectal cancer, Syndrome differentiation, Pattern diagnosis.
The identification of syndrome conditions had different impacts on CRC prognosis, and which may be related with different mRNA expression levels. Our results prelimitarily uncovered that some oncogenes and pro-inflammatory cytokines were highly expressed in Dampness Heat group but not other syndrome types and CRC patients with Dampness Heat syndrome might have a poor prognosis.
TCM syndrome is a kind of pathological profiles that reflect signs and symptoms at a certain stage of a disease, which is the most essential guidelines for the prescription of Chinese herbal formulae and also an important classification for CRC TCM therapy. A clear understanding biological basis of TCM syndrome will help the clinical diagnosis and the treatment for CRC patients hopefully.
Background
The disease of Jiju was recorded on the ancient book of Chinese medicine namedin Sui Dynasty of ancient China (610 C.E.), with the characters of abdominal pain, loose stools, abdominal mass, etc., which is similar to the clinical symptoms of colorectal cancer (CRC) in Western medicine. Till now CRC is one of the most common cancer around the world, although a lot of progress has been made over the past years [1]. Now, surgical resection is the main treatment strategy for early CRC patients, however, approximately 40% patients with stage II or III CRC may have a recurrence after surgery [2, 3]. Therefore, identifying efficient prognostic factors and improving the overall survival of CRC patients are important issue.
Traditional Chinese medicine (TCM) emphasizes integration concept of the environment and the human body. For patient cancer, TCM is one of the most common complementary and alternative therapy [4, 5]. TCM depends on syndrome differentiation diagnosis, which includes four diagnostic procedures: observation, listening, questioning, and pulse analyses. Syndrome is a kind of pathological profiles that reflect signs and symptoms at a certain stage of a disease [6]. Therefore, TCM syndrome is the most essential guidelines for the prescription of Chinese herbal formulae and also an important classification for CRC TCM therapy [7]. The CRC patients should be treated by different herbal prescription when they are diagnosed with different syndrome. However, when TCM meets modern medicine, the molecular basis and the validity of syndrome is poorly understood. So, a clear understanding biological basis of TCM syndrome will help the clinical diagnosis and the treatment for CRC patients hopefully.
In this study, we hypothesized that the identification of syndrome conditions had different impacts on CRC patients, and which mighbe related with different mRNA expression levels. To test this hypothesis, thirty healthy controls and 80 CRC patients broken down into four types of syndrome. As a result, we showed that Spleen Qi Deficiency, Dampness Heat and Blood stasis were the most common syndrome types in CRC. In the further study, we evaluated the expression of mRNA among these different TCM syndrome and demonstrated that the expression levels of,,andwere significantly associated with different syndrome types. For the molecular basis of different TCM syndrome in CRC, our results provide a new understanding.
Materials and methods
Literature search for publications on TCM syndrome in Chinese CRC patients
From January 2000 to June 2019, relevant studies were found based on searching the databases of PubMed, Web of Science, EMBASE, MEDLINE, and Cochrane library database. Meanwhile, we also consulted some Chinese periodicals, including CNKI (China Academic Journals), Wanfang and Weipu. The search strategy is the following: “Zhong Yi” (traditional Chinese medicine), “syndrome” or “Zheng” (syndrome), and“Rectal cancer” or “Colon cancer” or “Colorectal cancer”. More than 600 papers on TCM syndrome in CRC were initially identified.
Study subjects
This research protocol (2009-0007) was approved by the medical ethics committee of Jianggan District People’s Hospital and Sir Run Run Shaw Hospital. A total of 80 colorectal adenocarcinoma patients were consecutively recruited in Hangzhou, Zhejiang, China from January 2009 to July 2017 and healthy volunteers were used as the control group.
Diagnostic criteria
The diagnoses of all CRC patients were confirmed by pathology from surgical specimens. Trained interviewers used a uniform questionnaire to collect the TCM diagnostic information including name, gender, age, etc., and known risk factors for CRC. According the previous report, the standard criteria for the classification of CRC syndrome was performed [8]. CRC patients were divided into four main syndrome types: Spleen Qi Deficiency syndrome, Dampness Heat syndrome, Blood Stasis syndrome, and other syndromes.
a. Spleen Qi Deficiency syndrome: its clinical symptom is similar to that of cancer related fatigue and the digestion process is perturbed, making the person usually feel tired, are low in spirit and reluctant to talk as well as causing abdominal discomfort and loose stool [9–10].
b. Dampness Heat syndrome: it is similar to strong inflammation response and flat in Western medicine. So, these patients usually have heavy body weight, lack of appetite, thirsty but little/no desire to drink, brown yellowish urine, loose stools, etc. [11].
c. Blood Stasis syndrome: it is similar to hypercoagulable state of blood and is considered to be related with hemorheological properties changing. Usually, these patients have tingling pain, cyanosis or purple, dry stool (of skin, lips, nails, and/or tongue) with stasis maculae or spots [12].
Inclusion criteria
All CRC patients meet Western medicine and TCM criteria and the following characteristics: (a) Han (Chinese main ethnic group) Chinese ethnicity, (b) histopathologically diagnosed with primary CRC, (c) aged between 18 and 80 years, (d) had no antitumor therapy before recruitment, including radiotherapy and chemotherapy, and (e) did not have severe heart failure, pulmonary insufficiency, or kidney disease.
Exclusion criteria
Patients with appendix tumor, jejunum tumor, colorectal adenoma, E. stromal tumor, large intestine leiomyosarcoma, large intestine malignant melanoma and cases without pathological diagnosis and completed data were excluded.
CRC sample preparation
CRC serum samples were obtained from patients who had undergone a surgical procedure at the Affiliated Hospital of Hangzhou Normal University (Hangzhou, China). The written informed consent was obtained from all patients and all protocols regarding the use of patient samples in this study were approved by the Ethics Committee of Hangzhou Normal University. Serum samples were stored at -80 °C. All experiments were approved by the guidelines of the Hangzhou Normal University and performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). The method of Ficoll-Hypaque density gradient centrifugation was used to separate the peripheral blood mononuclear cells (PBMCs) from the peripheral venous blood of all patients [13]. Total human RNA (100 ng), extracted from PBMCs using Trizol Reagent (Invitrogen, CA, USA), was used as inputs for sample labeling and hybridization preparation in accordance with the manufacturer’s protocol (Agilent Technologies, Santa Clara, CA). Serum levels of carcinoembryonic antigen (CEA) and lactate dehydrogenase (LDH) were detected in hospital laboratory of Hangzhou Normal University. Microarray was used to detect mRNA expression profile and qRT-PCR was used to determine mRNA fold change [14].
Gene expression profiling and data processing
According to the protocol for manufacturer, gene expression profiling was performed by LC-Bio Technology Co., Ltd. (Hangzhou, Zhejiang, China) [15, 16] and ComBat was used to adjust possible batch effects [17]. All preprocessing steps were carried out in the statistical software R 3.1.0 with the lumi and sva packages [18, 19]. Libraries were prepared using the NebNext Ultra II Directional RNA library prep kit for Illumina (NEB #E7760) and NEBNext Multiplex Oligos for Illumina (E7355). NextSeq500 instrument was used to sequence all samples with single-end 75bp reads to a depth of 30-50M reads/sample. Then, differentially expressed mRNAs were identified using the t-test with the cut-off criteria of< 0.05 and fold-change > 2 or < 0.5.
qRT-PCR
According to the manufacturer’s instructions, total RNA was reversely transcribed into cDNA via using the SuperScript@III Reverse Transcriptase Kit (Invitrogen, CA, USA). Quantitative real-time PCR was performed using SYBR Green dye (Ambion, Carlsbad, CA, USA) on an Applied Biosystems 7500 Sequence Detection System (Applied Biosystems, Foster City, CA). The thermal cycling conditions were as follows: an initial step at 95°C for 15 s followed by 40 cycles of 95°C for 5 s and then 60°C for 30 s. Each experiment was performed in a final 20 μl of reaction volume containing 2 μl of cDNA, 0.8 μl of forward primer and reverse primer at the concentration of 10 μM for each one, 10 μl of SYBR®Prime Ex Taq™ II (2×), 0.4 μl of ROX Reference Dye or Dye II (50×) and 6 μl of H2O. All of the reactions were run in triplicate. The fixed threshold settings were used to determine the cycle threshold (CT) data and a comparative CTmethod was used to compare each condition to the control reactions. Relative gene expression levels were normalized to the internal control GAPDH. The primers for quantitative real time PCR (qRT-PCR) analysis were as follows: PIK3CA-F 5’- GGTGAAAGACGATGGACAACTGT -3’PIK3CA-R 5’- TGTAACACATCTCCTGAAACCTCTC -3’STAT3-F 5’- CAGAGCCCCATTTTCTGGTA -3’STAT3-R 5’- AGGACAGGGAGTGGTGTTTG -3’SOX9-F 5’- AAGCTCTGGAGACTTCTGAACG -3’SOX9-R 5’- CGTTCTTCACCGACTTCCTCC -3’KDM5C-F 5’- CGGCAGTACCTGCGGTATC -3’KDM5C-R 5’- TCAGTTCTTCAAGGCTGCG -3’GAPDH-F 5’- CTATAAATTGAGCCCGCAGC -3’GAPDH-R 5’- GACCAAATCCGTTGACTCCG -3’
Statistical analyses
The Chi-square and Fisher's exact tests were used to evaluate the correlation coefficient of two factors. The Kaplan-Meier method was used to compare the survival of patients with colorectal cancer with different syndrome and the logrank test was used to test the differences between the survival curves. The analysis of variance was used to examine the difference among gene expression levels. All data analysis was conducted with GraphPad Prism Software Version 6 (GraphPad, San Diego, CA) and all data are showed as mean ± Std.< 0.05 was defined as statistically significant.
Results
Investigation of TCM syndrome in Chinese colorectal cancer patients
From January 2000 to June 2019, relevant studies were found by searching various English and Chinese databases. More than 600 papers on TCM syndrome in CRC were initially identified. Summary analysis from these publications indicated the main deficiency syndrome for CRC were Spleen Qi Deficiency, Weakness of Spleen and Stomach, Yin Deficiency of Liver and Kidney, Deficiency of both Qi and Blood, and Yang Deficiency of Spleen and Kidney (Figure 1A), which accounted for 90.8% of the total. The main excessive syndrome for CRC were Dampness Heat, Blood Stasis, and Stagnation of Qi, which accounted for 96.81% of the total (Figure 1B).
Characteristics and syndrome distribution of the study subjects
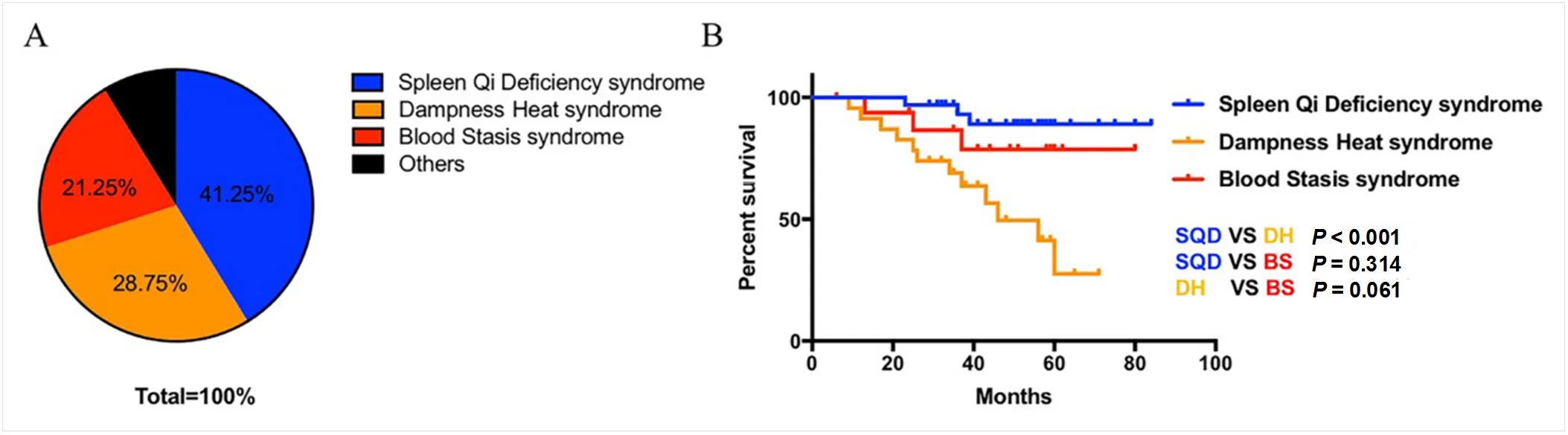
A total of 80 CRC patients were included in the study. The most common syndrome in CRC are Spleen Qi Deficiency (41.25% of studies), Dampness Heat (28.75%) and Blood Stasis (21.25%) (Figure 2A). Gender, age, tumor stage, the expression level of CEA and LDH, and syndrome distribution of subjects are shown in Table 1. The CRC patients with Dampness Heat syndrome has a higher CEA and LDH expression than those patients with Spleen Qi Deficiency and Blood Stasis subtype (< 0.05). However, there is no significant difference among gender proportion, age, drinking, diet habit, individual disease history and tumor stage (> 0.05). In further study, we evaluated whether different syndrome subtypes had different impact on the prognosis of CRC patients. As a result, the CRC patients with Dampness Heat syndrome are found to have a poor prognosis (Figure 2B). Altogether, our study demonstrated a correlation between syndrome types and the expression level of CEA and LDH as well as prognosis in CRC patient.
Analysis of gene expression profiles in the three groups of CRC patients
To determine the gene expression of CRC patients with different TCM syndrome, we first detected mRNA expression of three blood samples of patients with CRC from the Spleen Qi Deficiency, Dampness Heat, Blood Stasis, and control groups by gene expression array. As shown in Figure 3A, we found that there is a significantly different mRNA expression among the Spleen Qi Deficiency, Dampness Heat, Blood Stasis, and control groups. The higher mRNA levels of,,,,,,,,,,and the lower expression of inflammatory cytokineare found in Spleen Qi Deficiency groups but not other syndrome types. The higher mRNA levels of,,,,,,,,,,and some inflammatory cytokines (,,,) are found in Dampness Heat groups but not other syndrome types. Meanwhile, the lower mRNA levels of,,,,,,,,,,,,,andare shown in Dampness Heat groups but not other syndrome types. Compared with Dampness Heat groups, Blood Stasis syndrome shows higher expression of,,,,,and, and lower mRNA levels of,,,,and. We also examined the expression of,,andby. As a result, we demonstrate that the Dampness Heat group expresses the highest levels ofandand the lowest levels ofand(Figure 3B). Therefore, different TCM syndrome showed different mRNA expression level and the higher expression of some oncogenes (,,,,,,,) and pro-inflammatory cytokines () contributed to Dampness Heat syndrome types, which indicated that the molecular basis of Dampness Heat syndrome in CRC might be different from other syndrome types and the CRC patients with Dampness Heat syndrome might have a poor prognosis.

Figure 1 Summary analysis of TCM syndrome from annual publications. (A) Deficiency syndrome description; (B) Excessive syndrome description. TCM, Traditional Chinese medicine.
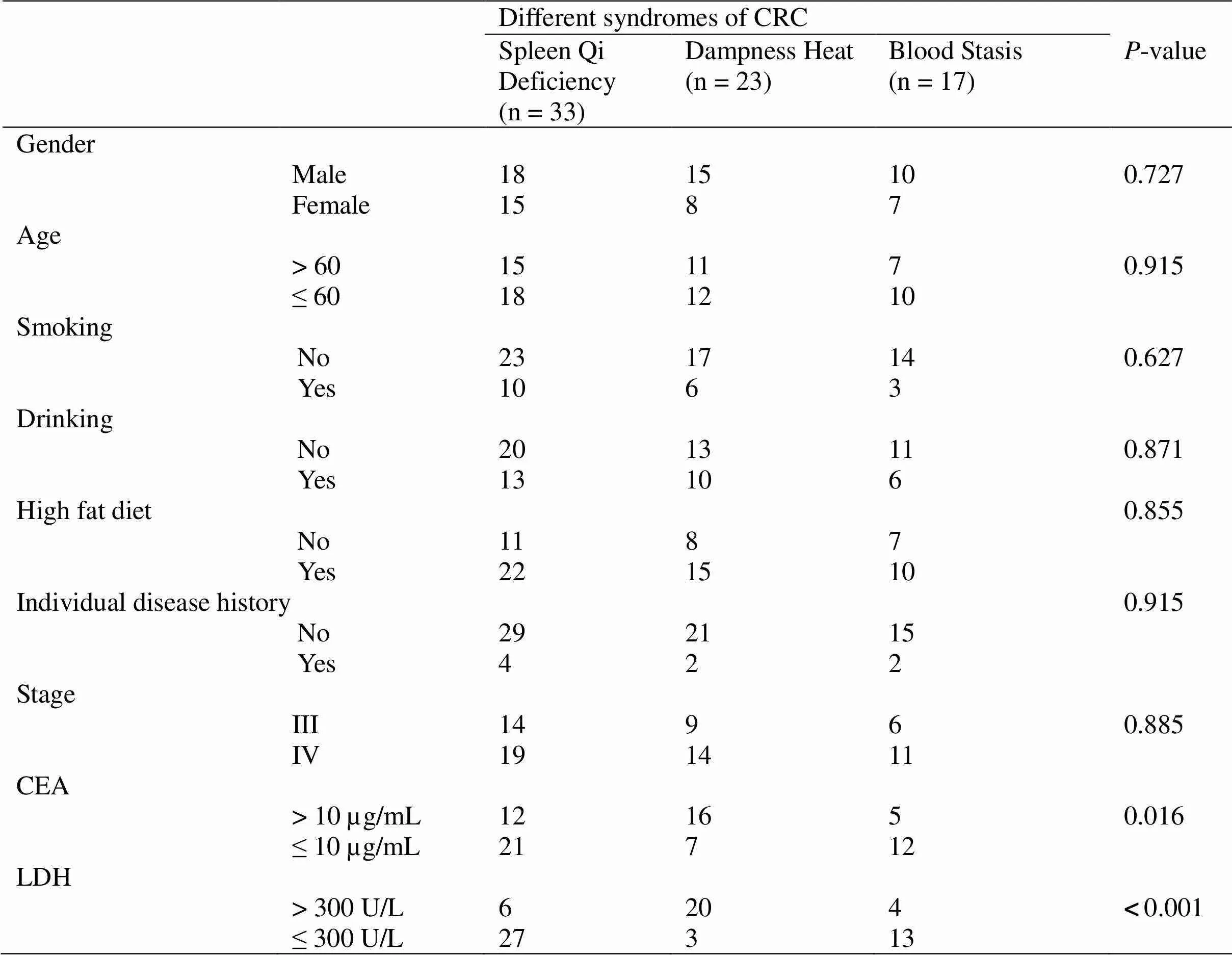
Table 1 Correlation between clinicpathological background and different traditional Chinese medicine syndromes in 73 cases of CRC patients
CRC, colorectal cancer; CEA, carcinoembryonic antigen; LDH, lactate dehydrogenase.

Figure 2 Syndrome distribution and prognosis of CRC patients. (A) Clinical distributions of TCM syndrome in CRC; (B) The prognosis of CRC patients with different syndrome types. SQD: Spleen Qi Deficiency; DH: Dampness Heat; BS: Blood Stasis.
Discussion
TCM is widely used to improve the efficacy of chemotherapy and relieve the clinical symptom of China. In TCM theory, Chinese medicine is prescribed according to syndrome [20]. Syndrome differentiation has been considered to guide the choiceofindividualizedtreatmentwithTCM herbal formulae since the ancient time of China [21–23].Therefore, the classical TCM therapeutic principle, “same disease treated by different therapies” or “different diseases treated by same therapy”, is usually adopted in cancer treatments [20]. However, it is difficult to cover the scientific basis of the complexity of syndrome, which limits the widespread application of TCM in the world [6, 24–26]. Therefore, understanding the potential molecular mechanisms underlying syndrome in CRC is urgently needed.

Figure 3 The molecular basis of TCM syndrome in CRC patients. (A) mRNA expression profiles of blood samples of CRC from the Spleen Qi Deficiency, Dampness Heat, Blood Stasis, and control groups are detected by gene expression array; (B) mRNA expression levels ofandare confirmed by. a, For, compare with other syndrome,< 0.001; b, For, compared with other syndrome,< 0.001; c, For, compared with other syndrome,= 0.001; d, For, compared with other syndrome,< 0.001.
It is known that cancer is often influenced by changes from the genes that control the body’s phenotypes and gene expression profiles are tightly correlated with carcinogenesis and cancer development [27–29]. A large number of studies have investigated the relationship between molecular basis and TCM syndromes [30, 31]. Dai, et al. found the existence of TCM syndrome could influence the tumor growth in pancreatic cancer, which might be mediated by the expression of chemokines CCR5/CCL5/CCL4 [6]. Tao, et al. and Hu, et al. showed that serum and plasma biomarkers could be a potential screening tool for the diagnosis and stratification of CRC patients with different syndrome differentiation [32, 33]. Wang and her colleagues identified that the emergence of syndrome conditions before or after tumor occurrence had significant different impacts on pancreatic cancer development. In the further study, they declared that tumor-associated macrophage infiltration and inflammatory cytokines including IL-6, IL-10, and p-STAT3 contributed to these differences [34]. However, the studies about the relationships between CRC syndrome and genetic susceptibility are few.
In the present study, we investigated the clinical distribution of TCM syndrome in CRC patients and found Spleen Qi Deficiency, Dampness Heat and Blood Stasis were the most common syndrome types in CRC. Next, we analyzed the clinicopathological characteristics of CRC patients with different TCM syndrome. We showed that the Dampness Heat subtype in CRC had a significantly higher CEA and LDH expression, compared with Spleen Qi Deficiency and Blood Stasis group. However, there was no significant differences among gender proportion, age and tumor stage. In further study, we evaluated the impact of different syndrome types on CRC prognosis and found CRC patients with Dampness Heat syndrome had a poor survival. To further determine the possible molecular mechanisms underlying different TCM syndrome, gene expression array was used to detect mRNA expression of blood samples of CRC from the Spleen Qi Deficiency, Heat Dampness, Blood Stasis, and control groups. Interestingly, some oncogenes (,,,,,,,) and inflammatory cytokines (,,,) were found higher expression in Dampness Heat groups but not other syndrome types. EGFR inhibitors were reported to significantly inhibit LPS-induced IL-1β, IL-6, and TNF-α production via NF-κB inactivation [35]. ARID1A and PIK3CA mutations were demonstrated to cooperate to promote tumor growth through sustained IL-6 inflammatory cytokine signaling [36]. Therefore, our results indicated the CRC patients with Dampness Heat syndrome might have a poor prognosis. However, we only examined three blood samples for each syndrome group, large-scale and multicenter collaboration will be necessary in the future.
Conclusion
Therefore, these results indicated that the gene expression profiling approach could be a potential approach for the diagnosis and stratification of CRC patients with different syndrome differentiation, which was also demonstrated by. In summary, our results provide insights into the potential utility and prognosis of TCM syndrome and may hopefully improve understanding of the molecular basis of TCM syndrome in CRC.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019, 69: 7–34.
2. Hong Y, Liew SC, Thean LF, et alHuman colorectal cancer initiation is bidirectional, and cell growth, metabolic genes and transporter genes are early drivers of tumorigenesis. Cancer Lett 2018, 431: 213–218.
3. Yang X, Xu ZJ, Chen X, et alClinical value of preoperative methylated septin 9 in Chinese colorectal cancer patients. World J Gastroenterol 2019, 25: 2099–2109.
4. Ling CQ, Yue XQ, Ling C. Three advantages of using traditional Chinese medicine to prevent and treat tumor. J Integr Med 2014, 12: 331–335.
5. McCulloch M, See C, Shu XJ, et alAstragalus-based Chinese herbs and platinum-based chemotherapy for advanced non-small-cell lung cancer: meta-analysis of randomized trials. J Clin Oncol 2006, 24: 419–430.
6. Dai HY, Wang P, Feng LY, et alThe molecular mechanisms of traditional Chinese medicine ZHENG syndromes on pancreatic tumor growth. Integr Cancer Ther 2010, 9: 291–297.
7. Su SB, Lu A, Li S, et alEvidence-Based ZHENG: A Traditional Chinese Medicine Syndrome. Evid Based Complement Alternat Med 2012, 2012: 246538.
8. Cheng CW, Kwok AO, Bian ZX, et alThe Quintessence of Traditional Chinese Medicine: Syndrome and Its Distribution among Advanced Cancer Patients with Constipation. Evid Based Complement Alternat Med 2012, 2012: 739642.
9. Hou FG, Cen Y, Guan J, et alQuantified diagnositic standard for large intestinal cancer of Spleen Qi Deficiency syndrome. J Chin Integr Med 2009, 7: 814–818. (Chinese)
10. Yang L, Li TT, Chu YT, et alTraditional Chinese medical comprehensive therapy for cancer-related fatigue. Chin J Integr Med 2016, 22: 67–72.
11. Yao W, Yang C, Wen Y, et alTreatment effects and mechanisms of Yujin Powder on rat model of large intestine Dampness Heat syndrome. J Ethnopharmacol 2017, 202: 265–280.
12. Hsu PC, Huang YC, Chiang JY, et alThe association between arterial stiffness and tongue manifestations of blood stasis in patients with type 2 diabetes. BMC Complement Altern Med 2016, 16: 324.
13. Vasanthkumar T, Hanumanthappa M, Lakshminarayana R. Curcumin and capsaicin modulates LPS induced expression of COX-2, IL-6 and TGF-β in human peripheral blood mononuclear cells.Cytotechnology 2019: 1–14.
14. Sui X, Guo Y, Ni W, et alMolecular profiling analysis for colorectal cancer patients with Pi-Xu or Shi-Re syndrome. Integr Med Res 2019, 8: 21–25.
15. Eberwine J, Yeh H, Miyashiro K,et alAnalysis of gene expression in single live neurons. Proc Natl Acad Sci U S A 1992, 89: 3010-3014.
16. Wu J, Wang C, Zhu X, Chen J. Sequence analysis of double-strand RNA6 and RNA9 from the fungus Sclerotium hydrophilum. Arch Virol 2017, 162: 2913–2917.
17. Johnson WE, Li C, Rabinovic A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8: 118–127.
18. Du P, Kibbe WA, Lin SM. lumi: a pipeline for processing Illumina microarray. Bioinformatics 2008, 24: 1547–1548.
19. Parker HS, Leek JT, Favorov AV, et alPreserving biological heterogeneity with a permuted surrogate variable analysis for genomics batch correction. Bioinformatics 2014, 30: 2757–2763.
20. Ji Q, Luo YQ, Wang WH, et alResearch advances in traditional Chinese medicine syndromes in cancer patients. J Integr Med 2016, 14: 12–21.
21. Guo Y, Zou Y, Xu YF, et alStudy on Chinese medicine syndrome of colorectal carcinoma in perioperative period. Chin J Integr Med 2015, 21: 183–187.
22. Chen P, Ni W, Xie T, et alMeta-Analysis of 5-Fluorouracil-Based Chemotherapy Combined With Traditional Chinese Medicines for Colorectal Cancer Treatment. Integr Cancer Ther 2019, 18: 1534735419828824.
23. Zhai B, Zhang N, Han X, et alMolecular targets of β-elemene, a herbal extract used in traditional Chinese medicine, and its potential role in cancer therapy: A review. Biomed Pharmacother 2019, 114: 108812.
24. Chen S, Zhang Z, Zhang X, et alTCM therapies combined with chemotherapy for preventing recurrence and metastasis in postoperative II to IIIA NSCLC: A protocol for a systematic review and meta-analysis. Medicine (Baltimore) 2019, 98: e14724.
25. Zhao M, Chen Y, Wang C, et alSystems Pharmacology Dissection of Multi-Scale Mechanisms of Action of Huo-Xiang-Zheng-Qi Formula for the Treatment of Gastrointestinal Diseases. Front Pharmacol 2019, 9: 1448.
26. Ma L, Zheng X, Yang Y, et alEpigenetic differences of chronic hepatitis B in different TCM syndromes: Protocol for a case-control, non-interventional, observational clinical study. Medicine (Baltimore) 2018, 97: e12452.
27. Chen Z, Chen LY, Wang P, et alTumor Microenvironment Varies under Different TCM ZHENG Models and Correlates with Treatment Response to Herbal Medicine. Evid Based Complement Alternat Med 2012, 2012: 635702.
28. Yan Y, Gong Z, Xu Z. Vitamin D supplementation and colorectal cancer prognosis. Med Oncol 2019, 36: 69.
29. Carlini MJ, Recouvreux MS, Simian M, et alGene expression profile and cancer-associated pathways linked to progesterone receptor isoform a (PRA) predominance in transgenic mouse mammary glands. BMC Cancer 2018, 18: 682.
30. Chen G, Gao J, He H, et alIdentification of differentially expressed non-coding RNAs and mRNAs involved in Qi stagnation and blood stasis syndrome. Exp Ther Med 2018, 17: 1206–1223.
31. Cheng XR, Cui XL, Zheng Y, et alA Co-Module Regulated by Therapeutic Drugs in a Molecular Subnetwork of Alzheimer's Disease Identified on the Basis of Traditional Chinese Medicine and SAMP8 Mice. Curr Alzheimer Res 2015, 12: 870–885.
32. Tao F, Lu P, Xu C,et alMetabolomics Analysis for Defining Serum Biochemical Markers in Colorectal Cancer Patients with Qi Deficiency Syndrome or Yin Deficiency Syndrome. Evid Based Complement Alternat Med 2017, 2017: 7382752.
33. Hu XQ, Wei B, Song YN, et alPlasma metabolic profiling on postoperative colorectal cancer patients with different traditional Chinese medicine syndromes. Complement Ther Med 2018, 36: 14–19.
34. Wang FJ, Wang P, Chen LY, et alTAM Infiltration Differences in "Tumor-First" and " ZHENG-First" Models and the Underlying Inflammatory Molecular Mechanism in Pancreatic Cancer. Integr Cancer Ther 2018, 17: 707–716.
35. Elkamhawy A, Hassan AHE, Paik S, et alEGFR inhibitors from cancer to inflammation: Discovery of 4-fluoro-N-(4-(3-(trifluoromethyl) phenoxy)pyrimidin-5-yl)benzamide as a novel anti-inflammatory EGFR inhibitor. Bioorg Chem 2019, 86: 112–118.
36. Chandler RL, Damrauer JS, Raab JR, et alCoexistent ARID1A-PIK3CA mutations promote ovarian clear-cell tumorigenesis through pro-tumorigenic inflammatory cytokine signalling. Nat Commun 2015, 6: 6118.
#Li-Jun Jin and Ying Liu are the co-first authors of this paper.
:
This research was supported by grants from National Natural Science Foundation of China (grant No. 81874380, 81672932, 81730108 and 81973635), Zhejiang Provincial Natural Science Foundation of China for Distinguished Young Scholars (grant No. LR18H160001), Zhejiang Province Science and Technology Project of TCM (grant No. 2019ZZ016), Zhejiang Province Medical Science and Technology Project (grant No. 2017RC007), Talent Project of Zhejiang Association for Science and Technology (grant No. 2017YCGC002), Key Project of Hangzhou Ministry of Science and Technology (grant No. 20162013A07), Zhejiang Provincial Project for the Key Discipline of Traditional Chinese Medicine (grant No. 2017-XK-A09), the Open Project Program of Jiangsu Key Laboratory for Pharmacology and Safety Evaluation of Chinese Materia Medica (No. JKLPSE201807) and the Project of the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
:
CRC, colorectal cancer; TCM, traditional Chinese medicine; CEA, carcinoembryonic antigen; LDH, lactate dehydrogenase; PBMCs, peripheral blood mononuclear cells.
:
The authors declare that there is no conflict of interest. None of the contents of this manuscript has been previously published or is under consideration elsewhere. All the authors read and approve the final version of the manuscript prior to submission.
:
Li-Jun Jin, Ying Liu, Ming-Ming Zhang, et al. Clinical distribution and molecular profiling on postoperative colorectal cancer patients with different traditional Chinese medicine syndromes.Traditional Medicine Research 2020, 5 (1): 44–52.
:Nuo-Xi Pi.
:8 August 2019,
10 September 2019,
:21 September 2019.
Tian Xie, Email: drxiet@aliyun.com; Xin-Bing Sui, Email: hzzju@zju.edu.cn. Holistic Integrative Pharmacy Institutes and Comprehensive Cancer Diagnosis and Treatment Center, the Affiliated Hospital of Hangzhou Normal University, College of Medicine, Hangzhou Normal University, 2318 Yuhangtang Road, Yuhang District, Hangzhou, China.
 Traditional Medicine Research2020年1期
Traditional Medicine Research2020年1期
- Traditional Medicine Research的其它文章
- Frequent attacks on health workers in China: social changes or historical origins?
- Research hotspot and frontier progress of cancer under the background of precision medicine
- Application of nanoparticles in the early diagnosis and treatment of tumors: current status and progress
- Complementary and alternative medicine applications in cancer medicine
- Editor-in-Chief of Special Issue on Integrative Oncology
- Astragalus injection as an adjuvant treatment for colorectal cancer: a meta-analysis