Infrabrow excision to correct upper eyelid dermatochalasis in middle-aged and elderly patients
2020-08-06 03:12WeiWeiZhangXiaoXiaRen2DongRunTangTongWuFengYuanSun
国际眼科杂志 2020年8期
Wei-Wei Zhang,2, Xiao-Xia Ren2, Dong-Run Tang, Tong Wu, Feng-Yuan Sun
Abstract
•KEYWORDS:infrabrow skin excision; dermatochalasis; curative effect; blepharoplasty
INTRODUCTION
Upper eyelid blepharochalasis is common in middle-aged and elderly people of Asian ancestry.It is usually accompanied by other symptoms of periocular aging, such as eyebrow ptosis, volüme loss and periorbital hollowing, crow’s feet, prolapse of periorbital fat, abnormal "triangle" eyelid fissure caused by lateral can thus prolapse, the compensatory deepening of frontal wrinkles, and widening of the distance between brow and lids and so on.These changes are not conducive for a youthful appearance and show fatigue, which can have a negative impact on the psychological and social activities of the patients.In addition, severe cases of flabby, loose skin can block the optical axis, leading to a narrow field of vision[1].Furthermore, mechanical pressure of the skin can lead to entropion, resulting in irritation in some patients.Therefore, treating upper eyelid laxity in the elderly is of great clinical importance.This laxity can simultaneously present problems in both appearance and function.Thus, its treatment should improve function while making the appearance more youthful.
The traditional surgical method for upper eyelid blepharochalasis entails the removal of excess skin by classic blepharoplasty alone.However, although this method can effectively solve the problem of skin redundancy, there are still shortcomings that are inherent to a standard upper blepharoplasty owing to the removal of excess eyelid skin alone.These shortcomings include the exacerbation of periorbital wrinkles and eyebrow droop, and elongation of scar tissue caused by excessive skin removal, which further aggravates crow’s feet[2].Moreover, classical blepharoplasty neglects the position and shape of the eyebrows, which makes the overall appearance of the eyelids inharmonious after the operation.In recent years, with the continuous development of plastic surgery technology, scholars have been paying more attention to the brow-eye as a continuum in surgical design[3].Hence, eyebrow surgery is gradually being applied as a novel surgical method to correct upper eyelid skin redundancy.Because of the obvious scars caused by an upper eyebrow incision and the limited amount of skin removal possible, sub-eyebrow incisions are mostly used at present.
This article documents the application of the infrabrow skin excision in the treatment of upper eyelid skin redundancy in middle-aged and elderly Chinese women, including its advantages, disadvantages, and indications.
SUBJECTS AND METHODS
PatientsA retrospective analysis was conducted of 30 patients (60 lids) with upper eyelid blepharochalasis admitted to Shanxi Eye Hospital from January 2018 to June 2018.All patients underwent the infrabrow skin excision procedure.Their ages ranged from 40 to 64 years, with an average age of 53.20±7.10 years.All patients were female.The study protocol was in accordance with the principles of the Declaration of Helsinki.
Preoperative evaluation was conducted from the following aspects.Firstly, a routine preoperative general examination was performed.Secondly, eyelid and eyebrow evaluation were determined by the following: position and symmetry of eyebrow, brow curvature or arch, degree of skin laxity, function of the levator palpebrae muscle, vertical eyelid fissure, situation of the eyelid margin, size and position of the lacrimal gland, as well as the presence or absence of any scars, infection, eyelid masses, upper eyelid depression, or incomplete eyelid closure.Lastly, global eye examination determined visual acuity and corrected visual acuity, eye movement, and whether exophthalmos was present.In addition, the fundus was observed with a slit lamp.The Schirmer’s test was used to determine whether the eyes were dry.The inclusion criteria of the surgical procedure included the following: the presence of upper lid dermatochalasis with lateral hooding; patients who wished to modify the eyebrow contour or who had failed tattoos; patients whowished to retain the original shape of the eyelid; patients who could not accept a lengthy lateral upper eyelid scar; and patients who remained with skin relaxation after eyelid incision surgery.
Patients with severe scars or infections of the upper eyelid and eyebrow were excluded, in addition to those withany kinds of ptosis (including congenital or acquired), severe coagulation disorders or systemic disease affecting the safety of the operation, and lactating, pregnant, and menstruating women.Patients with severely dry eyes were also excluded, to prevent more serious complications after the operation[4].
No eyebrow surgery was performed in any patient.Informed consent forms were signed before the operations, which were all performed by the same surgeon.
SurgicalTechniqueThe surgeon used a fine-tip marker and small calipers to mark patients who were in the supine position.The upper margin of the incision, which is usually above the margin of the brow to minimize scarring, was drawn first.Toothless forceps were used to pinch excess skin and patients were instructed to open and close their eyes to determine the amount of skin to be removed and facilitate the design of the lower edge of the incision (Figures 1A, 1B).The widest area of the skin excision should be enough to correct lateral drooping of the skin.The amount of skin removed depended on the severity of each patient’s dermatochalasis.However, the distance between the eyebrow and eyelid margin must be greater than or equal to 20 mm to prevent lagophthalmos after the operation[5].
All procedures were performed under local anesthesia, by injecting 2% lidocaine containing 1100,000 epinephrine.A No.11 or 15 blade was used to make an incision to the depth of the subcutaneous fat layer.The infrabrow incision was at an angle of approximately 30° to the skin surface to prevent damage to the hair follicles (Figure 1C).Another incision was made in the lower margin of the marking.The excess skin was excised from the layer above the orbicularis oculi.Hemostasis was achieved by bipolar electrocoagulation before wound closure (Figure 1D).Prolapsed fat was easily resected appropriately, whereas lateral fat was transplanted to the sunken site in patients with upper eyelid depression.
In patients with eyebrow droop, the orbicularis oculi muscle was also incised.If the correction was not satisfactory, the eyebrow fat pad was fixed to the superior periosteum of the eyebrow arch at the eyebrow peak.The orbicularis oculi of the lower skin incision was pulled upward and sutured to the orbicularis oculi of the upper skin incision using 6-0 absorbable sutures, while adjusting to the symmetry of both eyes and natural eyelid shape.The 6-0 absorbable suture was used to intermittently suture subcutaneous tissue of the incision to reduce tension (Figure 1E).The infrabrow skin was closed with continuous 7-0 non-absorbable sutures (Figure 1F).All patients were treated with cold compresses within 48h postoperatively, and the incision wound dressing was changed daily.Sutures were removed 7d after the operation.
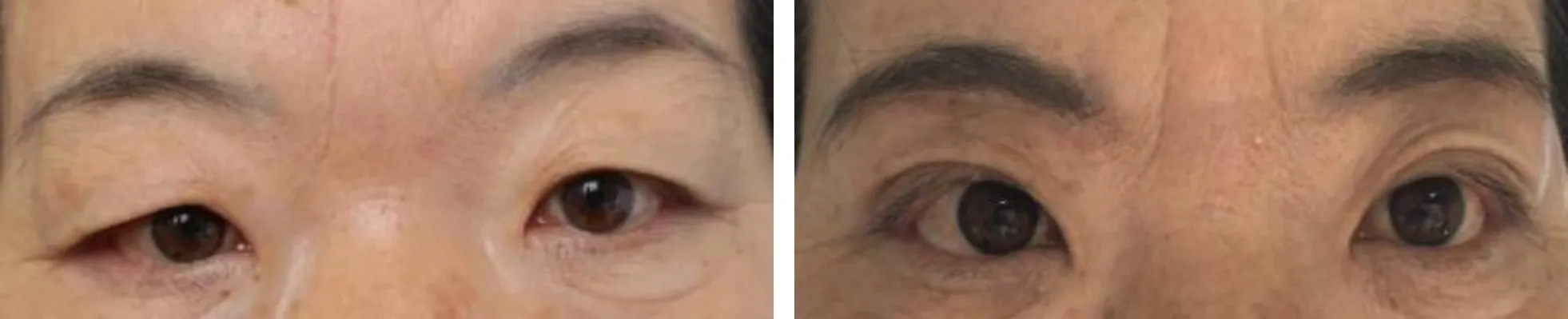
Figure 4 A 56-year-old woman, preoperative and 6mo postoperatively.

Figure 3 A 61-year-old woman, preoperative and 6mo postoperatively.

Figure 2 A 57-year-old woman, preoperation and 6mo postoperatively.

Figure 1 The procedure of surgery
OutcomeAssessmentandFollow-upThe degree of skin surplus on both upper eyelids was evaluated using a five-point grading scale (0-4)[6]: 0: no skin surplus; 1: minimal skin surplus; 2: moderate skin surplus, not reaching the eyelashes; 3: evident skin surplus, reaching the eyelashes; 4: severe skin surplus, beyond the eyelashes.The results of postoperative skin surplus were graded as good, fair, and poor.Good results referred to a score of 0-1, fair results referred to a score of 2, and poor results referred to a score of 3-4.
An objective grading system was used to evaluate the cosmetic surgical results[7].The evaluation system consisted of five parameters: malposition, distortion, asymmetry, contour deformity, and scarring.Each parameter was graded and scored for severity as follows: perfect (0 points); noticeable (1 point); obvious (5 points); and obvious and deforming (15 points).The total number of points was added for the final score.A perfect result had a total score of 0.Scores of 1-4 were considered good results; 5-14 were considered mediocre; and 15 or greater were considered poor.
Each evaluation was performed by two surgeons.If there was any difference in opinions between the two observers, the senior surgeon made the final decision.
RESULTS
Thirty patients (60 lids) were treated with the infrabrow skin excision, and the degree of skin surplus was obviously improved in all patients.One month after the operation, 52 lids (86.67%) showed good results, eight lids (13.33%) showed fair results, and no poor results were observed.Preoperative unsatisfactory position and shape of the eyebrows were improved, and crow’s feet and frontal lines were reduced.Patients complain the visual field of patients was improved, and opening of the eyes became easier.Thirty patients of our series demostrated excellent aesthetic results and improved vision.Patients expressed a high degree of overall satisfaction.The preoperative and postoperative degrees of skin surplus among the patients is presented in Table 1.
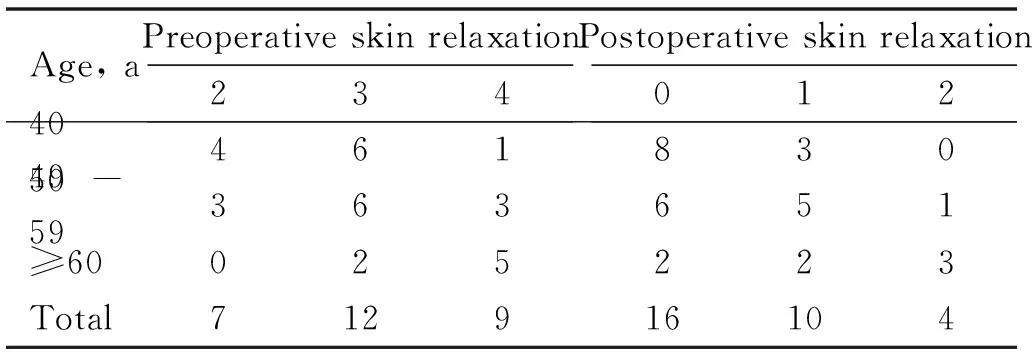
Table 1 Summary of preoperative and postoperative skin relaxation scores (n)
The objective Strasser system was used to evaluate surgical results at 1mo and 6mo.One month after the operation, all patients scored 1 for scarring and 0 for the other parameters.However, the scarring was acceptable because it was concealed in the eyebrow and inconspicuous.Moreover, no patient required subsequent corrective surgery.Some patients required scar removal gel.Six months after the operation, there were still two patients with scar scores of 1 and both continued to use scar removal gel.All patients had scores between 0 and 1 point, indicating good results.
Two patients had mild hematomas on the first day after the operation.They were both treated with cold compresses and pressure bandages.After one week, the hematomas improved obviously and returned to normal in two weeks.No serious complications, such as retrobulbar hemorrhage, lagophthalmos, wound dehiscence, entropion or ectropion, obvious asymmetry, eyelid deformity, visual impairment, or diplopia, were observed.
DISCUSSION
In this study, 30 patients have achieved a high level of satisfaction regarding functional results and the final aesthetic result.All patients reported subjective improvement in superior visual field.The technique not only preserved the original eyelid shape of patients, but also improved the relaxation of the upper eyelid which also made the compensatory frontal lines obviously reduced.The distance between the brows and lids decreased and a preoperative unsatisfactory eyebrow shape and position was improved, which made periorbital more harmonious and youthful but without a noticeable change, met the needs of patients for micro-plastic surgery.Surprisingly, the crow’s feet also improved.Although the scars existed in different degrees 1mo after surgery, it was hidden in eyebrow and had no obvious effect on appearance.No appearance problems such as malposition, distortion, asymmetry, contour deformity and no serious complications were found in all patients.
The periorbital region is often the first facial area to show signs of aging[8], especially obvious lateral relaxation of the upper eyelid caused by Gravity and the weaker function of the levator muscle in the outer 1/3 of the upper eyelid.As a result of the weakness of the lateral frontal muscle and the role of the depressor orbicularis lateralis, eyebrow droop occurs earlier and more frequently laterally than medially[9-11].The drooping lateral eyebrow will aggravate a bloated upper eyelid and can lead to deeper wrinkles of the glabellum and temples, making the loosening of the upper eyelid more obvious.Furthermore, compensatory eyebrow elevation in patients with upper eyelid relaxation may also mask true eyebrow droop.Consequently, when designing surgery for upper eyelid relaxation, the relationship of the upper eyelids relative to the eyebrows should be analyzed in continuity.The approach of ignoring the link between the two structures, and considering them instead in isolation, will not achieve a smooth, esthetically pleasing postoperative result[12-14].Conventional upper eyelid blepharoplasty without considering the location and shape of the eyebrows can even cause eyebrow droop in some patients.In addition, due to the differences in skin thickness between the upper and lower incisions, the appearance of the bloated upper eyelid is more obvious after conventional upper eyelid blepharoplasty[15].
The infrabrow skin excision introduced in this study can solve many problems of the eyebrow and eyelid simultaneously, and therefore has obvious advantages over the traditional upper eyelid blepharoplasty.For example, the position of the eyebrow can be raised through the incision under the eyebrow to treat the droop of the eyebrow.In addition, an unsatisfactory preoperative shape of the eyebrow can be redesigned, and failed tattooed eyebrows can be removed.Although some surgeons complete the correction of eyebrow droop through an eyelid incision[16-17], it is crucial that the dissection proceeds in a preseptal plane up to the orbital rim.This operation is complex, the operative field is not clear, and the injury can be greater.Furthermore, the procedure is not suitable for Asians, probably because Asians have broader lid-brow spacing than Caucasians, which is not conducive to the direction in which dissection proceeds.However, the correction of eyebrow droop can be completed through the incision under the eyebrow, and maintain clear operative vision with little injury.
Another important advantage of the infrabrow skin excision is the retention of the original shape of the eyelid.Owing to their unique anatomical characteristics, the eyelids of approximately 40%-60% of Asians lack an eyelid crease[18].For some elderly patients, male patients, or patients with a good eyelid shape before surgery, too obvious eyelids changes are not desirable.They believe that excessive changes in eyelid morphology after the operation will have an adverse effect on their social activities.The infrabrow skin excision can meet the needs of these patients to a greater extent than the traditional eyelid incision.
The authors observed that the scars in the infrabrow regionare much more inconspicuous than in lids because they can be hidden in the eyebrow.The use of eyebrow makeup and cosmetic cream by women helps to attenuate the scar in this region while the scar is still apparent.Patients could have resumed normal daily or social activities after removal of the stitches within 1wk, without any negative impact.Furthermore, permanent eyebrow tattoos can be performed 6wk after surgery.Infrabrow skin excision scarring becomes almost unperceivable after 6mo.In present study, although two patients had noticeable scars 6mo after operation, it had little effect on their appearance as the scars were hidden by the tattoos.In addition, the authors believe that the tension of the lateral vertical direction of the infrabrow incision is greater, and can reduce crow’s feet, which will be aggravated by an eyelid incision, on extension of the incision.In this study, the crow’s feet of patients were reduced.
Although all patients in the present study were female, theoretically, this procedure is not limited to women.However, during surgical design, attention should be paid to the differences in eyebrow shape between male and female patients, as men tend to have more flattened eyebrows.The inside of the incision should not extend beyond the brow to avoid obvious scarring.In addition, it is not advisable to remove too much tissue, including skin, fat, or the orbicularis muscle.Excessive skin resection will result in lagophthalmos, and excessive removal of the orbicularis oculi muscle and fat will aggravate the sunken upper eyelid and make the appearance more aged.Besides, the authors consider that it is better to preserve the orbicularis muscle in order to avoid unpleasing scars.Moreover, in patients with obvious upper eyelid sagging, it is also necessary to transfer excess fat to the area of depression to make the appearance more youthful.In addition, because of the thickness of the subcutaneous tissue on the upper and lower edges of the incision, an unequal thickness suture technique should be adopted for subcutaneous sutures.In other words, a small amount of the upper margin tissue and a large amount of the lower margin tissue should be sutured together to maintain the balance of the incision and reduce scarring.We found that continuous sutures of the skin incision can also reduce scarring.
The infrabrow skin excision also has its drawbacks.First, the amount of skin removal is relatively limited, and therefore not satisfactory for patients with severe blepharochalasis (e.g.with obscured vision that is not compensated by the head position).Some surgeons advise against the treatment of very serious upper eyelid relaxation by infrabrow skin excision alone[19-20].However, combining the two methods can avoid their respective disadvantages to achieve better results.In addition, the surgery is not suitable for patients who wish to have double eyelids.Thus, it is crucial to reach a consensus with patients before the operation to fully respect their wishes.Another limitation of the technique is that the concurrent ptosis surgery cannot be performed due to compromised exposure.
The incidence of complications was low in the present study.Only two patients had mild hematomas, which could be attributed to the perimenstrual period.More attention should be paid tomenstrual history before the operation.However, this study also has some limitations.Because of the small sample size and relatively short follow-up time, some potential surgical risks and complications could not have been observed.Therefore, a larger sample size and observation and analysis over a longer term are needed to correct the shortcomings of the present study and avoid potential complications.Moreover, this study was limited to middle-aged and elderly women in China and was therefore not representative of the entire population.The application of this technique in other ethnicities and male patients, as well as patients older than 65 years and younger than 40 years needs further research and verification.Besides, absence of quantitative analysis is another drawback in the study.
In summary, infrabrow skin excision is an useful, safe, adjunctive upper eyelid reconstructive procedure for selected patients.The advantages of the procedure include: the removal of redundant skin, especially the thick lateral skin of the upper eyelid while solving many eyebrow problems, reduction of crow’s feet, inconspicuous scarring in the infrabrow region, easy procedure of short duration, fewer complications, shorter recovery time, improved correction of a baggy appearance and blepharochalasis without extreme changes, all of which result in an enhanced, smoother upper eyelid area.Nevertheless, the procedure is not recommended for patients with very severe upper eyelid cutis laxa or those who wish to have double eyelids.