
Therapeutic efficacy of moxibustion plus medicine in the treatment of infertility due to polycystic ovary syndrome and its effect on serum immune inflammatory factors
2020-08-29 02:49YeTiejun叶铁君ChengHongxia程红霞
关键词:红霞
Ye Tie-jun (叶铁君), Cheng Hong-xia (程红霞)
People’s Hospital of Kaihua, Zhejiang 324300, China
Abstract
Keywords: Moxibustion Therapy; Heat-sensitive Moxibustion; Polycystic Ovary Syndrome; Gonadal Steroid Hormones; Tumor Necrosis Factor-α; NF-kappa B; Infertility, Female
Polycystic ovary syndrome (PCOS) is a refractory endocrine disease with excessive androgen and insulin resistance as the pathological basis, and clinically characterized by menstrual disorders, anovulation, obesity, hirsutism and acne, and it is more common in adolescent and childbearing period women[1-2]. PCOS is an important factor causing ovulatory dysfunction. Infertility due to PCOS accounts for about 75% of ovulatory dysfunction infertility[3]. For infertility due to PCOS, clomifene citrate capsules and letrozol tablets are mainly used for ovulation induction in clinic, combined with oral contraceptives (diane-35) and insulin sensitizer (metformin hydrochloride tablets) to reduce the androgen level and improve insulin resistance[4]. However, Western medicine treatment has obvious limitations. Besides the high incidence of adverse reactions, it is easy to cause adverse pregnancy outcomes such as low pregnancy rate and high miscarriage rate[5].
PCOS belongs to the category of infertility and primary infertility in Chinese medicine. Traditional Chinese medicine (TCM) therapy has unique advantages of syndrome differentiation and holism concept. When applied in the treatment of infertility due to PCOS with different syndromes, in can produce certain efficacy[6-7]. As an important part of external treatment of TCM, moxibustion has the effects of warming-unblocking and warming-reinforcing, and is suitable for syndromes such as deficiency, cold and blood stasis. Clinical study suggested that moxibustion had a certain effect of ovulation promotion[8]. In this study, we used heat-sensitive moxibustion plus clomifene citrate capsules to treat infertility due to PCOS, and observed the clinical efficacy and its influence on the levels of serum immune inflammatory factors, so as to reveal the mechanism of moxibustion for infertility due to PCOS.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria of Western medicine
The diagnostic criteria of PCOS referred to the criteria for PCOS revised by the European Society of Human Reproduction and Embryology (ESHRE) and American Society of Reproductive Medicine (ASRM) in 2003[9]: oligo-ovulation or anovulation; clinical manifestation of excessive androgen or hyperandrogenism; polycystic ovarian changes seen under ultrasound; met 2 of the above 3 items, and excluded other causes of excessive androgen.
The diagnostic criteria of infertility[10]: those who had normal sexual life, without contraception for one year but failed to be pregnant.
1.1.2 Criteria for syndrome differentiation of TCM
Criteria for syndrome differentiation of TCM referred to the criteria for the syndrome of kidney deficiency and blood stasis in theGuiding Principles for Clinical Study of New Chinese Medicines[11]. Primary manifestations: oligomenorrhea or amenorrhea, or menstrual cycle disorder, infertility after long marriage, hyposexuality. Secondary manifestations: soreness and weakness in the waist and knees, dizziness and tinnitus, stabbing pain in lower abdomen, a dark tongue or petechia on the tongue, sunken and stagnant pulse or slow pulse.
1.2 Inclusion criteria
Those who met the above diagnostic criteria for PCOS and infertility of Western medicine; met the syndrome of kidney deficiency and blood stasis for syndrome differentiation of TCM; aged 20-35 years; agreed to participate in this trial and signed informed consent.
1.3 Exclusion criteria
Patients with hyperthecosis, ovarian tumor, disorders of hormone levels caused by adrenal cortical hyperplasia; combined with severe diseases of cardiovascular system, lung, liver or kidney; those who were allergic to clomiphene; those had skin lesions or infections around the points; who were unconscious or unable to cooperate with the trial.
1.4 Dropout and elimination criteria
Those who dropped out during the treatment; got worse in the disease condition; those presenting with severe adverse reactions; or those with incomplete materials or data.
1.5 Statistical methods
All data were statistically analyzed by the SPSS version 20.0 statistical software. Chi-square test was applied to the comparisons of counting data. Measurement data in normal distribution and homogeneous variance were expressed as mean ± standard deviation (±s). Pairedt-test was used for intra-group comparisons before and after treatment, and groupt-test was used for comparisons between the groups. If data did not meet the normal distribution or homogeneous variance, non-parametric test was applied.P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
A total of 70 PCOS patients were enrolled from the People’s Hospital of Kaihua, between January 2016 and April 2018. All the patients were randomly divided into a control group and an observation group by the random number table method, with 35 cases in each group. There was no dropout case in the control group during the trial, while 2 cases in the observation group dropped out because of interruption of business trip. A total of 68 patients finished the study, with 35 cases in the control group and 33 in the observation group. The patients in the control group were aged between 21 and 33 years old, with the shortest duration of 2 years and the longest of 7 years, and the body mass index (BMI) between 19.25 kg/m2and 29.45 kg/m2. The patients in the observation group were aged between 20 and 34 years old, with the shortest duration of 2 years and the longest of 8 years, and the BMI between 19.29 kg/m2and 29.32 kg/m2. There were no significant differences in the data of average age, average duration of disease and average BMI between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).
Table 1. Comparison of the general data between the two groups (±s)

Table 1. Comparison of the general data between the two groups (±s)
Group n Average age (year) Average duration (year) Average BMI (kg/m2) Observation 33 26.3±3.9 4.9±1.9 23.64±2.84 Control 35 27.1±3.2 4.7±1.8 23.69±3.03
2 Treatment Methods
2.1 Control group
The control group received oral clomifene citrate capsules (National Drug Registration Number: H31021107, Shanghai Hengshan Pharmaceutical Co., Ltd., China), 50 mg/time, once a day, for 5 consecutive days from the 5th day of every menstruation. The treatment continued for 6 consecutive menstrual cycles.
2.2 Observation group
On the basis of the same medication in the control group, heat-sensitive moxibustion was added in the observation group.
Points: Guanyuan (CV 4) and bilateral Zigong (EX-CA 1), Xuehai (SP 10) and Shenshu (BL 23).
Moxa stick specifications: Hwato brand pure moxa sticks of 1.8 cm in diameter and 20 cm in length were used for moxibustion (Nanyang Wolong Chinese Medicine Moxa Factory, China).
Methods: The patient took a supine position at first, with local skin exposed. After receiving moxibustion at Zigong (EX-CA 1) and Xuehai (SP 10), the patient then took a prone position and received moxibustion at Shenshu (BL 23). The physician sought heat-sensitive points first, which was to apply circling moxibustion to the points with an ignited moxa stick 3-5 cm away from the skin around. When patient felt heat-sensitive phenomena such as heat penetration, heat expansion and heat transmission, it would be the heat-sensitive point. Then the physician continued to perform mild moxibustion to this heat-sensitive point, about 10 min for each point, till the disappearance of the heat sensitization[12]. The physician repeated the above steps until the selected points were completed for moxibustion in turn. The heat-sensitive moxibustion was performed every other day, for 6 consecutive menstrual cycles.
3 Observation of Curative Efficacy
3.1 Observation items
3.1.1 Endometrium thickness and ovarian volume
Transvaginal color Doppler ultrasound examination was performed in both groups before treatment, and on the 5th day of the first menstruation cycle after treatment. And the endometrium thickness and ovarian volume of the patients were measured.
3.1.2 Conception rate
Follow-up was performed for 1 year after treatment, and the pregnancy rates in the two groups were compared.
3.1.3 Sex hormone levels
The fasting venous blood was collected in early morning before treatment, and on the 5th day of the first menstrual cycle after treatment. The serum levels of testosterone (T), luteinizing hormone (LH) and estradiol (E2) were measured by chemiluminescence immunoassay (CLIA).
3.1.4 Levels of immune inflammatory factors
The fasting venous blood was collected in early morning before treatment, and on the 5th day of the first menstrual cycle after treatment. The tumor necrosis factor-α (TNF-α) and nuclear factor-κB (NF-κB) were measured by enzyme-linked immunosorbent assay (ELISA).
3.2 Results
3.2.1 Comparisons of endometrial thickness and ovarian volume
There were no significant differences in the endometrium thickness and ovarian volume between the two groups before treatment (bothP>0.05). After treatment, the endometrial thickness in both groups increased (bothP<0.05), while the ovarian volume decreased significantly (bothP<0.05). The endometrium of the patients in the observation group was thicker than that in the control group, and the ovarian volume was less than that in the control group, and the differences between the groups were statistically significant (bothP<0.05), (Table 2).
3.2.2 Comparisons of the sex hormone levels between the two groups
There were no significant differences in the serum T, LH and E2levels between the two groups before treatment (allP>0.05). After treatment, the serum T and LH levels in both groups decreased significantly (allP<0.05), while the serum E2levels increased significantly (bothP<0.05). The serum T and LH levels in the observation group were lower than those in the control group, the serum E2level was higher than that in the control group, and the differences between the groups were statistically significant (allP<0.05), (Table 3).
Table 2. Comparisons of endometrium thickness and ovarian volume between the two groups (±s)

Table 2. Comparisons of endometrium thickness and ovarian volume between the two groups (±s)
Note: BT=Before treatment; AT=After treatment; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Endometrium thickness (mm) Ovarian volume (mm3) Observation 33 BT 6.23±0.36 14.03±1.14 AT 9.65±0.821)2) 9.70±1.151)2) Control 35 BT 6.19±0.39 13.79±1.12 AT 7.74±0.621) 11.73±0.881)
Table 3. Comparisons of the sex hormone levels between the two groups (±s)

Table 3. Comparisons of the sex hormone levels between the two groups (±s)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time T (pmol/L) LH (IU/L) E2 (pg/mL) Observation 33 Before treatment 2.86±0.56 16.29±2.13 142.79±9.97 After treatment 1.03±0.341)2) 9.54±1.411)2) 191.89±16.511)2) Control 35 Before treatment 3.02±0.51 15.91±2.17 144.14±10.85 After treatment 2.11±0.451) 11.82±1.931) 167.89±15.221)
3.2.3 Comparisons of the immune inflammatory factor levels between the two groups
There were no significant differences in the serum TNF-α and NF-κB levels between the two groups before treatment (bothP>0.05). After treatment, the serum TNF-α and NF-κB levels in both groups decreased significantly, and the intra-group differences were statistically significant (allP<0.05). The serum TNF-α and NF-κB levels in the observation group were significantly lower than those in the control group, and the differences between the groups were statistically significant (bothP<0.05), (Table 4).
3.2.4 Comparison of the conception rate
After 1 year of follow-up, there were 7 cases of pregnancy in the control group, and the pregnancy rate was 20.0%. There were 17 cases of pregnancy in the observation group, and the pregnancy rate was 51.5%. The pregnancy rate in the observation group was significantly higher than that in the control group, and the difference was statistically significant (χ2=6.07,P<0.05).
3.2.5 Safety evaluation
During the treatment period, no obvious adverse reactions occurred in the two groups. After the treatment, the routine tests of blood, urine and feces, and liver and kidney functions of the patients in both groups showed no obvious abnormalities.
Table 4. Comparisons of the immune inflammatory factor levels between the two groups (±s)
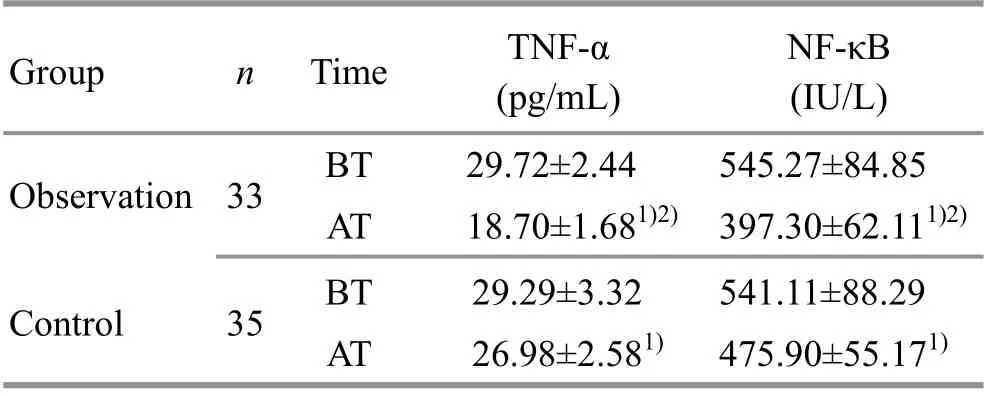
Table 4. Comparisons of the immune inflammatory factor levels between the two groups (±s)
Note: BT=Before treatment; AT=After treatment; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time TNF-α (pg/mL) NF-κB (IU/L) Observation 33 BT 29.72±2.44 545.27±84.85 AT 18.70±1.681)2) 397.30±62.111)2) Control 35 BT 29.29±3.32 541.11±88.29 AT 26.98±2.581) 475.90±55.171)
4 Discussion
Modern medicine believes that infertility due to PCOS is the result of a combination of various pathogenic factors and is closely related to genetic, obesity, environmental and social psychological factors[13]. The pathophysiological factors of PCOS are changeable and interact with each other. Therefore, the pathogenesis of this disease is still unclear. According to the characteristics of excessive androgen and high insulin in PCOS, doctors have proposed several mainstream hypotheses, such as female hypothalamic- pituitary-ovarian (HPO) axis dysfunction, insulin resistance, hyperandrogenism and adrenal dysfunction, which still fail to explain the pathological characteristics of infertility due to PCOS very well[14]. With the development of molecular biology research in recent years, the role of immune inflammatory factors such as TNF-α and NF-κB in the pathogenesis of infertility due to PCOS has got widespread concern.
TNF-α is a marked immune inflammatory factor, which plays an important role in the regulation of follicular development, corpus luteum formation, and steroid hormone production, and is closely related to insulin resistance. TNF-α may cause hyperplasia or apoptosis of follicular theca-interstitial cell in different stages of follicular development, leading to excessive hyperplasia of follicular theca and interstitial portion and the increase of ovarian volume. High level of TNF-α expression can inhibit the activity of insulin growth factor-1 in ovarian granular cells, affect lipid metabolism in follicular fluid, thereby affecting the normal development of follicles and reducing the quality of follicles[15]. When the serum TNF-α level increases, it inhibits the luteal function and promotes the corpus luteum degradation, resulting in a decrease in progesterone synthesis[16]. TNF-α can also reduce adipocyte differentiation, enhance steatolysis, increase the level of free fatty acids, impair insulin signal transduction, inhibit glucose transport after insulin stimulation, and reduce the expression of glucose carrier protein-4, resulting in insulin resistance[17]. Bi H,et al[18]measured the TNF-α level in the patients with PCOS before and after treatment, and found that TNF-α had an obvious high expression in PCOS patients, and the serum TNF-α level significantly reduced after the treatment of diane-35 combined with metformin. This also confirmed the correlation between TNF-α and PCOS.
NF-κB is an important nuclear transcription factor and has a certain relation with insulin resistance. Activated NF-κB promotes effector cells to release large amounts of proinflammatory cytokines, such as TNF-α, leaving the body in a chronic inflammatory state[19]. In addition, the NF-κB inhibitory protein kinase complex activates the NF-κB signaling pathway to secrete inflammatory factors, phosphorylates insulin receptor substrate-1, interferes with insulin signal transduction, leads to the decrease of the expression of insulin-sensitive transporters, and aggravates insulin resistance[20]. Liu MM,et al[21]measured the serum NF-κB level in PCOS patients and healthy volunteers, then found that the NF-κB level in the PCOS patients was significantly higher than that in healthy volunteers, and the NF-κB level in patients with PCOS accompanied by insulin resistance was higher than that in the patients without insulin resistance. The correlation analysis showed that NF-κ B was negatively correlated with insulin sensitivity index and positively correlated with insulin resistance index.
The location of PCOS is in uterus and is closely related to kidney, liver and spleen. Among them, the essence of kidney has a leading role in human reproductive function. In the ‘kidney-Tiangui (congenital kidney essence)-Thoroughfare and Conception Vessels-uterus’ axis, the fullness of kidney qi, the arrival of Tiangui (congenital kidney essence) and the Thoroughfare and Conception Vessels being filled with qi and blood can promote the maturity of the reproductive essence in the uterus. Therefore, kidney deficiency is the basic pathogenesis of this disease. If kidney qi is insufficient, blood will be inadequate and qi will be deficient, and the blood circulation will be stagnant. If kidney yang is deficient, the vital gate fire will decline, resulting in cold congelation and blood stasis. If kidney yin is deficient, then deficient heat will cause the impairment of fluid, then blood will be thicker, resulting in blood stasis. Therefore, syndrome of kidney deficiency and blood stasis is one of the most common syndromes in this disease[22]. The treatment should be based on tonifying the kidney, promoting blood circulation and regulating menstruation.
The heat-sensitive moxibustion is a moxibustion therapy that emphasizes the sensation of moxibustion, proposed by Professor Chen Ri-xin. It uses ignited moxa stick to apply suspended moxibustion to heat-sensitized points. It provokes the meridian transmission of the sensation of heat-sensitive moxibustion, with the individualized saturation dose signaled by the disappearance of the heat sensitization, so as to achieve the effect of ‘small stimulation to heat-sensitized points causing great response of the body’. Also, the heat-sensitive moxibustion has the effects and characteristics of the traditional moxibustion: ‘warming for unblocking, warming for reinforcing, and mutual play of unblocking-reinforcing’. It can strengthen vital qi and warmly unblock the meridians, and thus is suitable for infertility due to PCOS with syndrome of kidney deficiency and blood stasis. Zigong (EX-CA 1), Guanyuan (CV 4), Xuehai (SP 10) and Shenshu (BL 23) were selected in this study. Zigong (EX-CA 1) is located at 4 cun below and 3 cun away from umbilicus. It is effective for gynecologic diseases. Heat-sensitive moxibustion at Zigong (EX-CA 1) has the effects of activating blood flow and benefiting qi, warming uterus for regulating menstruation[23]. Guanyuan (CV 4) is the crossing point of the Spleen Meridian, Kidney Meridian, Liver Meridian and Conception Vessel. It is where the Yuan-Primordial qi stays, and the root of human, with the effects of invigorating and reinforcing Yuan- Primordial qi, consolidating the constitution and benefiting kidney[24]. Xuehai (SP 10) can activate blood flow and resolve stasis, replenish and nourish blood, combine unblocking with tonifying. It is the key point for all kinds of blood syndromes[25-26]. The Back-Shu point can reflect the disease, and also treat the disease, with the property of more for replenishing. Shenshu (BL 23) is the Back-Shu point of the kidney. Heat- sensitive moxibustion at Shenshu (BL 23) can reinforce kidney qi[27-28]. The above points together produced the effects of reinforcing kidney qi, promoting blood circulation and regulating menstruation.
In this study, the results suggested that the endometrium of the patients in both groups was significantly thickened after treatment (bothP<0.05), and the ovarian volume was significantly reduced (bothP<0.05). The endometrium of the patients in the observation group was thicker than that in the control group, and the ovarian volume of the patients in the observation group was less than that in the control group, and the differences between the groups were statistically significant (bothP<0.05). After 1 year of follow-up, the pregnancy rate in the observation group was significantly higher than that in the control group (P<0.05). After treatment, the levels of serum T and LH in both groups decreased, while the level of E2increased (allP<0.05). The levels of serum T and LH in the observation group were lower than those in the control group, and the E2level in the observation group was higher than that in the control group, and the differences between the groups were statistically significant (allP<0.05). After treatment, the serum TNF-α and NF-κB levels of the patients in both groups decreased (allP<0.05). The levels of serum TNF-α and NF-κB in the observation group were significantly lower than those in the control group (bothP<0.05). The above results indicated that heat-sensitive moxibustion plus clomifene citrate capsules can increase the endometrial thickness, reduce the ovarian volume, significantly improve the serum sex hormone levels, and increase the conception rate in patients with infertility due to PCOS, which may be related to the adjustment of the levels of immune inflammatory factors such as serum TNF-α and NF-κB.
Conflict of Interest
The authors declare that there is no conflict of interest in this article.
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 28 November 2019/Accepted: 24 December 2019
猜你喜欢
Chinese Physics B(2022年7期)2022-08-01
小学生作文(低年级适用)(2022年6期)2022-06-23
小学生作文(低年级适用)(2022年5期)2022-05-26
新高考·英语基础(高一)(2022年3期)2022-04-29
小学生作文·小学低年级适用(2022年4期)2022-04-27
Chinese Physics B(2022年4期)2022-04-12
作文周刊·小学一年级版(2020年40期)2020-10-19
中学生数理化·八年级物理人教版(2015年10期)2016-01-04
中国火炬(2014年7期)2014-07-24
 Journal of Acupuncture and Tuina Science2020年4期
Journal of Acupuncture and Tuina Science2020年4期
- Journal of Acupuncture and Tuina Science的其它文章
- Effect of electroacupuncture at Lower He-Sea points including Yanglingquan (GB 34) on nuclear factor-κB and interleukin-1β in guinea pigs with acute cholecystitis
- Study on the differences between moxibustion at different points in the effects on the anti-fatigue ability of rats undergoing one-time exhaustive swimming
- Clinical observation on herb-partitioned spreading moxibustion at Baliao points plus climen for diminished ovarian reserve
- Clinical study on auricular point sticking plus Western medicine for moderate gastric cancer pain
- Clinical observation on filiform fire-needling plus continuous passive motion therapy for frozen shoulder
- Electronic moxibustion apparatus and traditional moxibustion in treating knee osteoarthritis: a randomized controlled trial