
Pleomorphic rhabdomyosarcoma of the spermatic cord and a secondary hydrocele testis:A case report
2020-09-15 08:58
World Journal of Clinical Cases 2020年12期
Xin Chen,Ci Zou,Chao Yang,Liang-Kuan Bi,Dong-Dong Xie,De-Xin Yu,Department of Urology,The Second Hospital of Anhui Medical University,Hefei 230032,Anhui Province,China
Liang Gao,Center of Experimental Orthopaedics,Saarland University Medical Center,Homburg 66421,Germany
Abstract
Key words:Pleomorphic rhabdomyosarcoma;Spermatic cord;Secondary hydrocele testis;Case report
INTRODUCTION
Rhabdomyosarcoma (RMS) is a highly malignant sarcoma originating from immature striated muscle,which mostly occurs in children[1,2].Paratesticular RMS accounts for about 7% of all the rhabdomyosarcomas[3].More than 200 cases of paratesticular RMS have been reported,including tumors of the testis,epididymis,and spermatic cord[2-7].Although the therapeutic outcome of paratesticular RMS has been remarkably improved,it still depends on the tumor grade,distant disease,and tumor cell histology[4,5].The 5-year overall survival rate of confined paratesticular RMS after combined therapeutic arms including surgery,radiotherapy,and chemotherapy was 94.6%[6].
Pleomorphic RMS of the spermatic cord is one of the rarest histological types of paratesticular RMS and develops commonly in adults.Currently,only case reports with limited patient numbers and expert opinion are available for therapeutic instruction.The diagnosis of pleomorphic RMS of the spermatic cord is based on histological and specific immunohistochemistry features of the tumors.The imagological diagnosis of pleomorphic RMS of the spermatic cord is still challenging if the mass is not confined to paratesticular tissue,and is especially mislead by a concomitant secondary hydrocele.
We herein report a case of pleomorphic RMS of the spermatic cord with a secondary hydrocele testis,treated by radical orchiectomy,high ligation of the spermatic cord,radiotherapy,and immunotherapy.An up-to-date literature review of pleomorphic RMS of the spermatic cord was also performed.
CASE PRESENTATION
Chief complaints
A 79-year-old man presented to our clinic and complained of a 1-mo history of painless scrotal swelling.
History of present illness
A previous computed tomography (CT) scan at a local hospital identified a left 3 cm ×2 cm × 3 cm inguinal mass.The patient did not receive any treatment before he visited our clinic.His sleep and diet were not disturbed in the past 3 mo.
History of past illness
The patient was in good health in the past and only received an appendectomy 40 years ago.
Personal and family history
The patient reported no perceptible personal conditions related to the present clinical manifestation.Family history was also not noticeable.
Physical examination upon admission
Physical examination revealed approximately a left 15 cm × 10 cm × 5 cm inguinal mass with limited mobility (Figure1).The scrotum was irreducible,the left testicle was not palpable,and transillumination test was positive.

Figure1 Physical examination.A left scrotal mass measuring 15 cm was noted.
Laboratory examinations
Laboratory tests showed elevated serum β-human chorionic gonadotropin (β-HCG;240.70 mIU/mL) and squamous cell carcinoma antigen (3.20 ng/mL).Contrastenhanced magnetic resonance imaging (MRI) showed a hydrocele testis,several enlarged inguinal lymph nodes,and a heterogeneously enhanced lesion (15 cm × 10 cm × 6 cm) with a relatively well-defined margin in the left inguinal region (Figure2A and B).
FINAL DIAGNOSIS
The final diagnosis of the presented case was pleomorphic RMS of the spermatic cord and a secondary hydrocele testis.
TREATMENT
The patient received a wide resection of the mass,an inguinal incision with a high section of the left spermatic cord,and a left radical orchiectomy.Intraoperatively,the encapsulated tumor was found across the spermatic cord and extending into the scrotum,but without invasion to the testis or epididymis (Figure2C).Pathological analysis identified that the mass was composed of sheets of giant atypical and pleomorphic cells with abundant eosinophilic cytoplasm,which led to a diagnosis of pleomorphic RMS (Figure3A).Immunohistochemical examination showed a strong positivity for vimentin and Ki-67 (approximately 40%),as well as a weak positivity for desmin,smooth muscle actin (SMA),and myogenin (Figure3B-F).According to the Intergroup Rhabdomyosarcoma Study Group staging classification,the tumor was in clinical group IIb and clinically staged as T2bN1M0.
OUTCOME AND FOLLOW-UP
The patient experienced local relapse 1 mo postoperatively.With a Karnofsky performance score of 40,the patient received combined radiotherapy and anlotinib hydrochloride-based immunotherapy without additional chemotherapies.Regretfully,the patient died from multiple organ failure 3 mo postoperatively.
DISCUSSION
Spermatic cord RMS originates from mesenchymal components of the spermatic cord,with a poor prognosis[8].It was commonly reported in old men[7],but exceptional cases involved male teenagers[3].Pleomorphic RMS of the spermatic cord is the rarest type of RMS (about 7% of all RMS and about 6% of all paratesticular tumours) with a high metastasis rate and remains a significant challenge for clinical diagnosis and treatment[8,9].
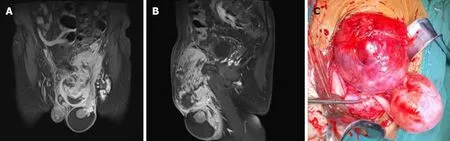
Figure2 Intraoperative finding.A and B:Coronal (A) and sagittal (B) views of contrast-enhanced magnetic resonance imaging showing a hydrocele testis and a heterogeneously enhanced lesion with a relatively well-defined margin;C:Intraoperative finding of the spermatic cord tumor and a secondary hydrocele testis.
MRI may provide significant information of tumor outline and adjacent bordering.The classic MRI feature of pleomorphic RMS of the spermatic cord is a paratesticular heterogeneously enhanced mass with or without compressing the testis.A paratesticular mass may be diagnosed empirically with hernia[10],or hydrocele[11],which potentially leads to a therapeutic delay.An ultrasound scan may echographically distinguish them.Tumors involving the scrotum might be masqueraded as reproductive system tumors.A secondary hydrocele testis occasionally accompanies the spermatic cord mass,which was only reported in less than ten cases since 2007 (Table1)[10-17].To the best of our knowledge,hydrocele testis secondary to pleomorphic RMS of the spermatic cord was not reported previously.Microscopically,the pleomorphic RMS was featured as a pleomorphic architecture of atypical/round rhabdomyoblasts and spindle cells[7].Its determinant diagnosis is largely based on the positive immunostaining for several highly sensitive and specific markers,such as vimentin,desmin,myoglobin,myosin,and SMA[7,18].Serum β-HCG generally tends to be normal in RMS patients,however,elevated β-HCG in our case should be highlighted as a potential diagnostic pitfall and raises the differential diagnosis from other germ cell tumors[19].
Most of therapeutic information on pleomorphic RMS was available from some individual institutions[2-4,7].A wide resection of tumor with a radical inguinal orchiectomy,followed by adjuvant therapy (e.g.,chemotherapy or radiotherapy) was the gold standard therapeutic arm for patients with a localized tumor.This is due to the fact that the tumor commonly recurs locally and invades the pelvic cavity through internal inguinal ring.However,the actual prognosis is dependent on the histology and metastatic stage of the tumors[7].Lack of pain in the mass contributed sometimes to therapeutic delays.A wide resection of tumors with radical inguinal orchiectomy followed by VAC (vincristine,actinomycin D,and cyclophosphamide) based chemotherapy is the gold standard treatment for localized tumors[20].The radiotherapy was recommended for controlling tumor local recurrence and remote metastasis[20,21].The combination of these therapeutic arms may increase the overall survival of RMS towards about 70%-90%[4,22].A poor prognosis cannot be avoided for advanced tumors.Since chemotherapy was not recommended for cases with a low Karnofsky performance score (< 70),the present patient received only combined radiotherapy and immunotherapy after the surgery[23].Emerging immunotherapy based on molecular mechanism of RMS is believed to improve the long-term survival of these patients[24].However,more preclinical studies and clinical trials are warranted to identify the optimal interventions for patients in advanced stages of this disease.
CONCLUSION
Only scarce reports of paratesticular RMS have been reported,mainly in the form of single neoplasia without a secondary hydrocele testis.Although multi-disciplinary approach including surgery,radiotherapy,and chemotherapy/immunotherapy is performed to maximize survival,an early diagnosis should also be confirmed.Physicians need to be aware of the occurrence of pleomorphic RMS in unusual locations,especially when accompanied by a hydrocele testis.
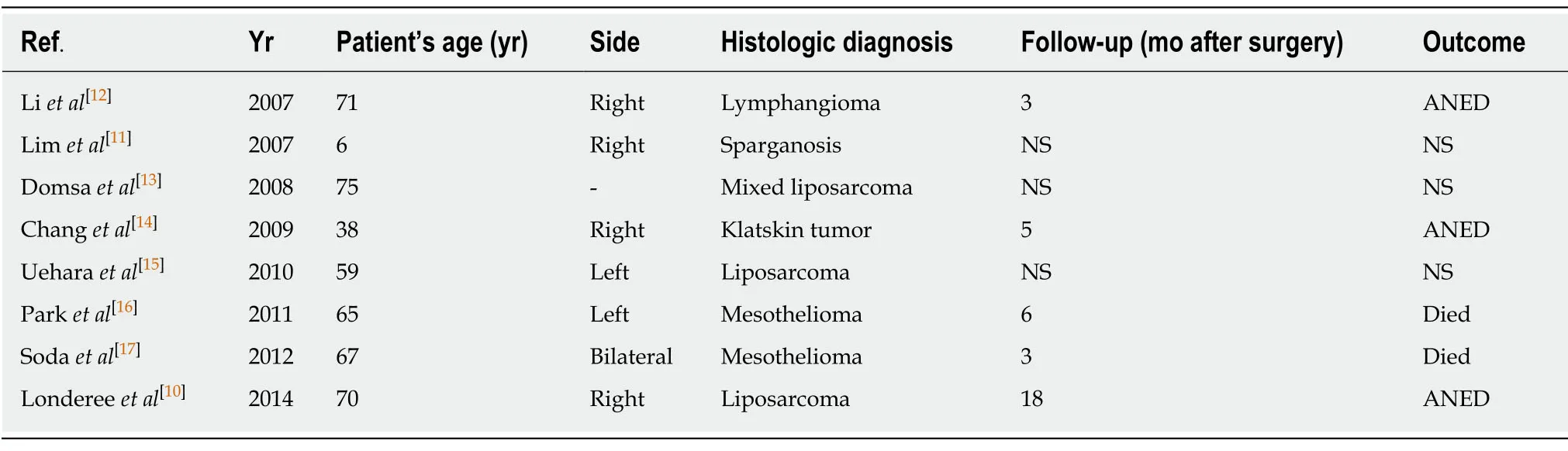
Table1 Spermatic cord mass with a secondary hydrocele (review of the literature from 2007 to 2019)
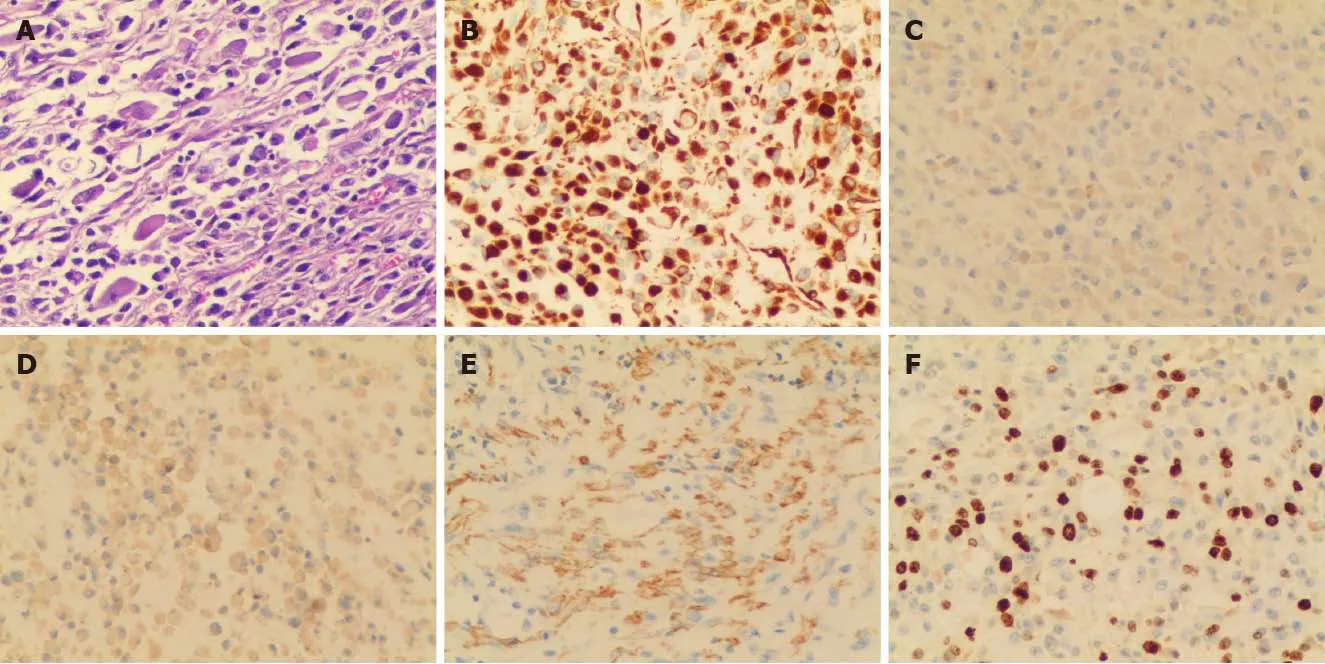
Figure3 Histopathological and immunohistochemical analyses.A:Formalin-fixed paraffin-embedded tumor tissue was stained with hematoxylin and eosin (100×);B:Vimentin (200 ×,cytoplasmic and membranous staining);C:Desmin (200 ×,cytoplasmic staining);D:Myogenin (200 ×,nuclear staining);E:Smooth muscle actin (200 ×,cytoplasmic and membranous staining);F:Ki-67 (200 ×,approximately 40% positivity).
ACKNOWLEDGEMENTS
We thank our colleagues for data processing:Dr.Zhen Hu at Department of Radiology,Dr.Ji-Feng Wu at Department of Pathology,and Dr.Ming-Zhu Gao at Department of Oncology of the Second Hospital of Anhui Medical University,Hefei,China.
 World Journal of Clinical Cases2020年12期
World Journal of Clinical Cases2020年12期
- World Journal of Clinical Cases的其它文章
- Assessment of diaphragmatic function by ultrasonography:Current approach and perspectives
- Computer navigation-assisted minimally invasive percutaneous screw placement for pelvic fractures
- Research on diagnosis-related group grouping of inpatient medical expenditure in colorectal cancer patients based on a decision tree model
- Evaluation of internal and shell stiffness in the differential diagnosis of breast non-mass lesions by shear wave elastography
- Real-time three-dimensional echocardiography predicts cardiotoxicity induced by postoperative chemotherapy in breast cancer patients
- Lenvatinib for large hepatocellular carcinomas with portal trunk invasion:Two case reports