
Medical use and misuse of psychoactive prescription medications among US youth and young adults
2021-04-06 08:50IsraelAgakuSatomiOdaniJantelNelson
Israel Agaku, Satomi Odani, Jantel Nelson
ABSTRACT
lNTRODUCTlON
National efforts to stem psychoactive prescription medication misuse in recent times have focused largely on the opioid epidemic, which kills nearly 50 000 Amer—icans every year from overdose.1For this paper, misuse is defined as the use of any prescription medicine that is not prescribed to the individual or taken as instructed by the prescribing doctor/nurse practitioner.2The number of emergency room visits involving the misuse of prescription medication more than doubled between 2004 and 2008.3Alarmingly, in the USA in 2017, drug overdose deaths were a leading cause of ‘unintentional injury death’.14Most, but not all these drug overdose incidents involve opioid analgesics, making it imperative to monitor other ‘lesser known’ psychoactive prescrip—tion medication misuse behaviours, to prevent another epidemic. Boyd et al found that 12% of their respondents had engaged in non— medical use of opioid pain medica—tions in the past year: 3% for sleeping, 2% as a sedative and/or for anxiety, and 2% as stimulants.5In 2017, the occurrences of first— time misuse for stimulants, tranquil—lisers and sedatives combined (2.8 million), surpassed that for prescription opioids (2.0 million) among persons aged ≥12 years old.2While evidence shows that stimulant medication therapy for attention— deficit hyperactivity disorder in early childhood does not increase subse—quent risk for non— medical use of prescription stimulants or other substance use behaviours,67there is basis for concern with misuse of prescription stimulants among youth.8Prescription drug monitoring programmes can help identify chronic prescription medication ‘shoppers’ such as adults. Their utility in detecting misuse or diver—sion among adolescents may be somewhat limited though because most youth and young adults who misuse psycho—active prescription medications obtain them from family and friends.2910Other measures such as psychoactive drug education programmes, changes in the Centers for Disease Control and Prevention (CDC) and US Food and Drug Administration (FDA)’s guidelines for prescribing opioids, and alternative medication options have also aided in the decrease of prescribing opioids. Parents/caregivers/guardians, pharmacists and clinicians there—fore need to be alert for behavioural markers of psycho—active prescription medication misuse. However, there are very little data on other psychoactive prescription medications besides opioids, for example, the extent of overlap in the behavioural characteristics of youth and young adults who misuse prescription opioids versus other psychoactive prescription medications, or those who misuse multiple psychoactive prescription medica—tions simultaneously, is poorly understood.
While opioid— specific studies can still offer valu—able clinical insights regarding misuse of psychoactive prescription medications in general, the populations from which several existing studies of youths and young adults were drawn may limit their generalisability. Two of the commonly analysed national surveillance systems in relation to psychoactive prescription medication misuse are school— based surveys, which are not generalisable to all school— aged youth and young adults. These surveys are, Monitoring the Future (eighth, tenth and twelfth graders),11and the Youth Risk Behaviour Survey (eighth graders to twelfth graders).12Besides non— inclusion of middle school students under eighth grade, these surveys also exclude groups (eg, school dropouts) or schools (eg, special education schools, alternative schools and Department of Defence operated schools) whose members may have elevated risk of substance use.12Recent and generalisable data on youth and young adults are needed across the diversity of psychoactive prescrip—tion medications.
Using a nationally representative, household— based sample of US youth and young adults aged 12—25 years during 2015—2017, this study had two objectives: (1) assess prevalence and weighted population counts describing use, misuse, dependence and abuse for prescription opioids, sedatives, tranquillisers, stimulants, as well as at least two psychoactive prescription medications. (2) compare behavioural and demographic profiles of youth and young adults reporting medical use versus misuse of the different psychoactive prescription medications assessed.
METHODS
Data source
Data were from the National Survey of Drug Use and Health (NSDUH). The survey participants were indi—viduals from households, non— institutional group quar—ters (eg, college dormitories) and civilians living on military bases.13To increase privacy, questionnaires are completed by the individuals themselves using audio, computer— assisted self— interview methods. The analyses in this report were restricted to youth aged 12—17 years and young adults aged 18—25 years. We pooled data across the 2015—2018 waves to increase sample size; pooled sample size was n=54 866 for youth aged 12—17 years and 55 690 for young adults aged 18—25 years, average response rate=67.4%.
Measures
Psychoactive prescription medications
Past— year use of four psychoactive prescription medi—cations was assessed: opioids, stimulants, tranquillisers and sedatives. Respondents were asked to answer when they used the respective medications last time. We used recoded dichotomous variables provided in NSDUH to assess past— year use. We also created an aggregate measure of any (ie, at least one) and multiple (ie, at least two) use of psychoactive prescription medications.
Medical use and misuse of psychoactive prescription medications
Past— year medical use and misuse were defined as to be mutually exclusive within our analyses. Misuse was defined as a report by the respondent that they had used the psychoactive prescription medications in the past year in any way not directed or prescribed, including (1) use without a prescription of the respondent’s own; (2) use in greater amounts, more often, or longer than the respon—dent was told to take them; or (3) use in any other way a doctor did not direct the respondent to use them. Respon—dents were classified as having an indication of medical use if they reported using the psychoactive prescription medications in the past year but reported no misuse for that specific medication. It should be noted that NSDUH did not distinguish between intentional misuse (eg, diver—sion, with overdose) versus non— intentional misuse (eg, medication errors). Some misclassification may therefore exist.
Substance use disorder of psychoactive prescription medications
Within our analysis, substance use disorder was defined as having symptoms of abuse and/or dependence on the psychoactive prescription medications in the past year. The questions were asked based on the Diagnostic and Statistical Manual of Mental Disorders fourth edition (DSM— IV) criteria.1314To be classified as having depen—dence, at least three criteria had to be met from the following: (1) spent a lot of time engaged in activities related to drug use, (2) used drug in greater amounts or for longer period than intended, (3) developed toler—ance, (4) unsuccessfully tried to cut down, (5) continued drug use despite physical or emotional problems associ—ated with use, (6) reduced or stopped participating in other activities because of drug use, and (7) had with—drawal symptoms after reducing or stopping drug use. Individuals were classified as having abuse if they did not meet the dependence criteria for that drug and reported at least one of the following: (1) experienced problems at work/home/school because of drug use; (2) engaged in something physically dangerous following regular drug use; (3) had repeated trouble with the law because of drug use; and (4) continued drug use despite problems with family/friends.
Non-prescription substance use
Past—30— day and past— year use was assessed for the following non— prescription substances: alcohol; tobacco (cigarettes and cigars); marijuana; cocaine; heroin; inhalants; and hallucinogens. Variables describing recency of use for each substance were created with the following four cate—gories: never user, last used within the past 30 days (≤30 days), 31 days to 12 months (≤12 months) or used more than 12 months ago (>12 months). An aggregate measure was also created, with never users defined as persons who had never used any of the assessed substances; classifi—cation into other categories (≤30 days, ≤12 months, >12 months) was based on using at least one substance within the specified time window, conditional on not meeting the criteria for a more recent period. We also created two separate variables that tallied total number of non— prescription substances used for either the past 30 days or the past 12 months.
Other covariates
Demographic variables assessed were sex, age, race/ethnicity, educational attainment, poverty status, health insurance and metro status (whether the respondent lived in a metropolitan statistical area delineated by the Office of Management and Budget). We also assessed presence of serious psychological distress in the past year among young adults.15This information was available only for adult respondents aged ≥18 years and measured using the Kessler—6 Psychological Distress Scale (range 0—24). As recommended by previous assessment, scores 13 or above were classified as having serious psychological distress in NSDUH.
Statistical analyses
Since data were being pooled across 3 years, we reca—librated the weights by dividing by three to generate accurate weighted population counts. Among those who reported past— year use, we calculated the weighted percentages of those reporting misuse: group differences were tested with χ2tests. Prevalence estimates with rela—tive standard errors >40% were suppressed because of imprecision. Conceivably, older adolescents and younger adults have more access to medications and less parental oversight than preteens or early adolescents; we therefore analysed age as a tabulation variable, within the catego—ries of 12—13; 14—15; 16—17; 18—20; or 21—25 years (which were the smallest age classification available in NSDUH). As part of descriptive analyses, we calculated three specific estimates for each psychoactive prescription medication assessed: (1) any use, regardless of whether it was medical or non— medical use (2) medical use (3) misuse use; the last two measures were mutually exclusive of each other and were the main focus of this paper. For each of the four psychoactive prescription medications, exploratory Poisson regression analyses were performed to compute prevalence ratios and compare characteristics of indi—viduals reporting medical use versus misuse. Variables assessed included sex, race/ethnicity, education, poverty status, health insurance, metro status, psychological distress and recency of any non— prescription substance use. Separate Poisson regression models were further fitted to measure the relationships between psychoac—tive prescription medication misuse and recency of each non— prescription substance use and number of non— prescription substances used, adjusting for sex, age, race/ethnicity, education, poverty status, health insurance, metro status and psychological distress. We compared the performance of the past—30— day tally versus the past— year tally as a behavioural marker of psychoactive prescrip—tion medication misuse. Variance inflation factors (VIFs) were computed to examine multicollinearity for each of the models fitted, and confirmed VIF for each indepen—dent variable did not exceed 5. Poisson regression anal—yses were restricted to respondents aged 18—25 years as psychological distress was assessed for this age group only. All data were weighted and analysed with R V.3.5.3.
RESULTS
Prevalence of use, misuse and substance use disorder of psychoactive prescription medications among youth aged 12-17 years
Among US youth aged 12—17 years, 25.0% reported use of any psychoactive prescription medication assessed, and 5.7% reported using at least two psychoactive prescription medications in the past year (table 1). Among those who used any psychoactive prescription medication, 20.9% (1.3 million) reported misuse; 3.4% were classified as having substance use disorder. Among those who used at least two psychoactive prescription medications in the past year, 46.1% reported misuse of any psychoactive prescription medication and 62.1% reported concurrent use of a non— prescription substance (data not shown in table).
Past— year use of each psychoactive prescription medica—tion was as follows: opioids (19.0%), stimulants (7.2%), tranquillisers (4.3%) and sedatives (2.2%) (table 2). Among users of each psychoactive prescription medica—tion, the estimated percentage reporting misuse was as follows: opioids (17.6%, 0.8 million), stimulants (24.2%, 0.4 million), tranquillisers (40,1%, 0.4 million) and seda—tives (14.2%, 80 000). Among users of each psychoactive prescription medication, the estimated percentage having substance use disorder was as follows: opioids 2.6%, stim—ulants 3.0%, tranquillisers 7.0% and sedatives 3.6% (data not shown in table). Stratified estimates of past— year use, misuse and at least two product use are presented in tables 1 and 2 for some demographic characteristics.
Prevalence of use, misuse and substance use disorder of psychoactive prescription medications among young adults
Among US young adults aged 18—25 years, 41.0% reported use of any psychoactive prescription medication assessed, and 13.4% reported using at least two psychoac—tive prescription medications in the past year (table 3). Among those who used any psychoactive prescription medication, 34.7% (4.9 million) reported misuse; 4.2% were classified as having substance use disorder. Among those who used at least two psychoactive prescription medications in the past year, 60.7% reported misuse of any psychoactive prescription medication and 93.6% reported concurrent use of a non— prescription substance (data not shown in table).
Past— year use of each psychoactive prescription medica—tion was as follows: opioids (30.2%), stimulants (14.1%), tranquillisers (11.5%) and sedatives (3.5%) (table 4). Among users of each psychoactive prescription medica—tion, the estimated percentage reporting misuse was as follows: opioids (23.3%, 2.4 million), stimulants (51.3%, 2.5 million), tranquillisers (45.1%, 1.8 million) and seda—tives (19.0%, 0.2 million). Among users of each psycho—active prescription medication, the estimated percentage having substance use disorder was as follows: opioids 3.0%, stimulants 3.7%, tranquillisers 5.6% and sedatives 1.6% (data not shown in table).
Contrasting demographic profiles associated with medical versus non-medical use (misuse)
Among young adults aged 18—25 years, psychological distress and recency of any non— prescription substance use was strongly associated with both medical use and misuse of psychoactive prescription medications (table 5). Those who had serious psychological distress constantly showed increased likelihood of medical use, ranging from adjusted prevalence ratio (APR) =1.12 for opioids to APR=2.89 for sedatives; and misuse, ranging from APR=1.60 for stimulants to APR=3.06 for sedatives. Asso—ciation between recency of non— prescription substance use and misuse is further discussed in a later section.
For opioids, men had lower likelihood of opioid medical use (APR=0.70, 95% CI 0.67 to 0.73), but greater likeli—hood for reporting misuse than women (APR=1.22, 95% CI 1.13 to 1.32) (table 5). Compared with whites, Asians and Hispanics had lower likelihood for both medical use and misuse of opioids: blacks did not differ from whites for medical use but had lower likelihood for misuse (APR=0.82, 95% CI 0.73 to 0.93). Although Medicaid insurees and Medicare insurees had higher likelihood of reporting opioid medical use compared with uninsured persons (APR=1.32 and 1.45, respectively), they did not differ significantly for misuse.
For stimulants, both medical use and misuse were higher among men than women (APR=1.23 and 1.30, respec—tively). Likelihood of medical use and misuse of stimulants were both significantly lower among all non— white race/ethnic groups compared with whites. Whereas poverty status was not associated with medical use, it was however associ—ated with misuse, with lower likelihood of misusing stimu—lants seen among individuals living above the poverty line. Compared with those living in poverty, adjusted prevalence of medical use of stimulants was lower by 29% (APR=0.71) among those living at up to twice the poverty level, and by 22% (APR=0.78) among those living at more than twice the poverty level. Individuals with private insurance had signifi—cantly higher likelihood of medical use (APR=1.37, 95% CI 1.18 to 1.58) and misuse (APR=1.44, 95% CI 1.25 to 1.67) relative to those uninsured. The likelihood of medical use and misuse were both significantly lower among those in non— metropolitan than metropolitan areas (APR=0.88 and 0.80, respectively).
For tranquillisers, men were less likely to report medical use (APR=0.66, 95% CI 0.60 to 0.72), but more likely to report misuse (APR=1.15, 95% CI 1.05 to 1.26). Compared with whites, the likelihood of both medical use and misuse of tranquilliser were lower among non— white groups, except non— Hispanic other race for misuse that showed no signifi—cant difference. Whereas no difference in metropolitan status was observed for medical use of stimulants, the likelihood of misuse was significantly lower among those in non— metro than metropolitan areas (APR=0.87, 95% CI 0.76 to 0.99).
For sedatives, the likelihood of medical use was lower among: men than women (APR=0.84, 95% CI 0.73 to 0.96); blacks (APR=0.55, 95% CI 0.44 to 0.69), Asians (APR=0.35, 95% CI 0.23 to 0.54), Hispanics (APR=0.61, 95% CI 0.50 to 0.74); and non— metropolitan than metro—politan dwellers (APR=0.80, 95% CI 0.68 to 0.95). These groups did not differ from their referent categories for misuse of sedative, except non— Hispanic blacks and Hispanics for which the likelihood of misuse was also significantly lower than whites (APR=0.39 and 0,63, respectively).
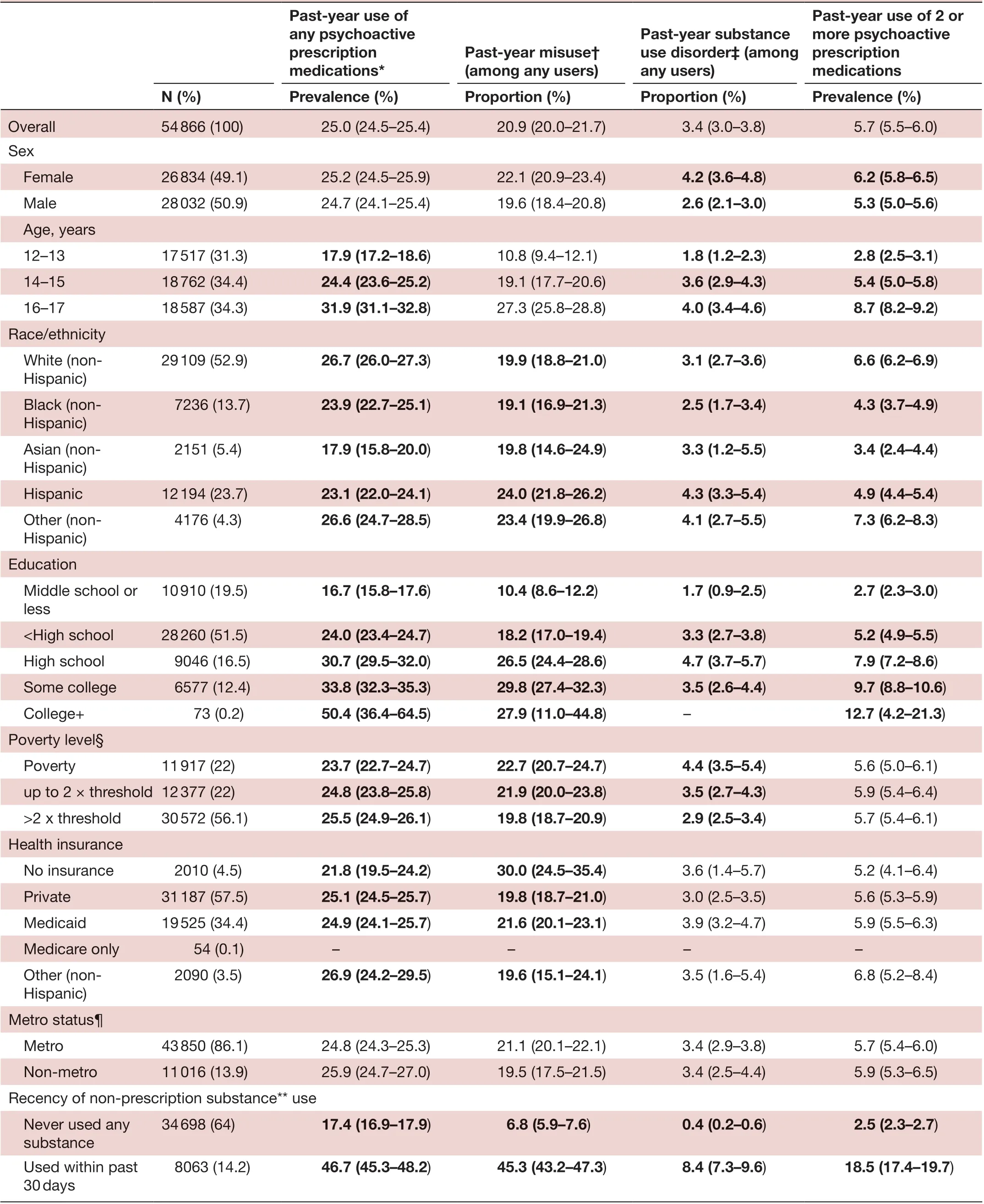
Table 1 Demographic characteristics and usage patterns of any psychoactive prescription medications among US youth aged 12-17 years, National Survey of Drug Use and Health, 2015-2018
Continued
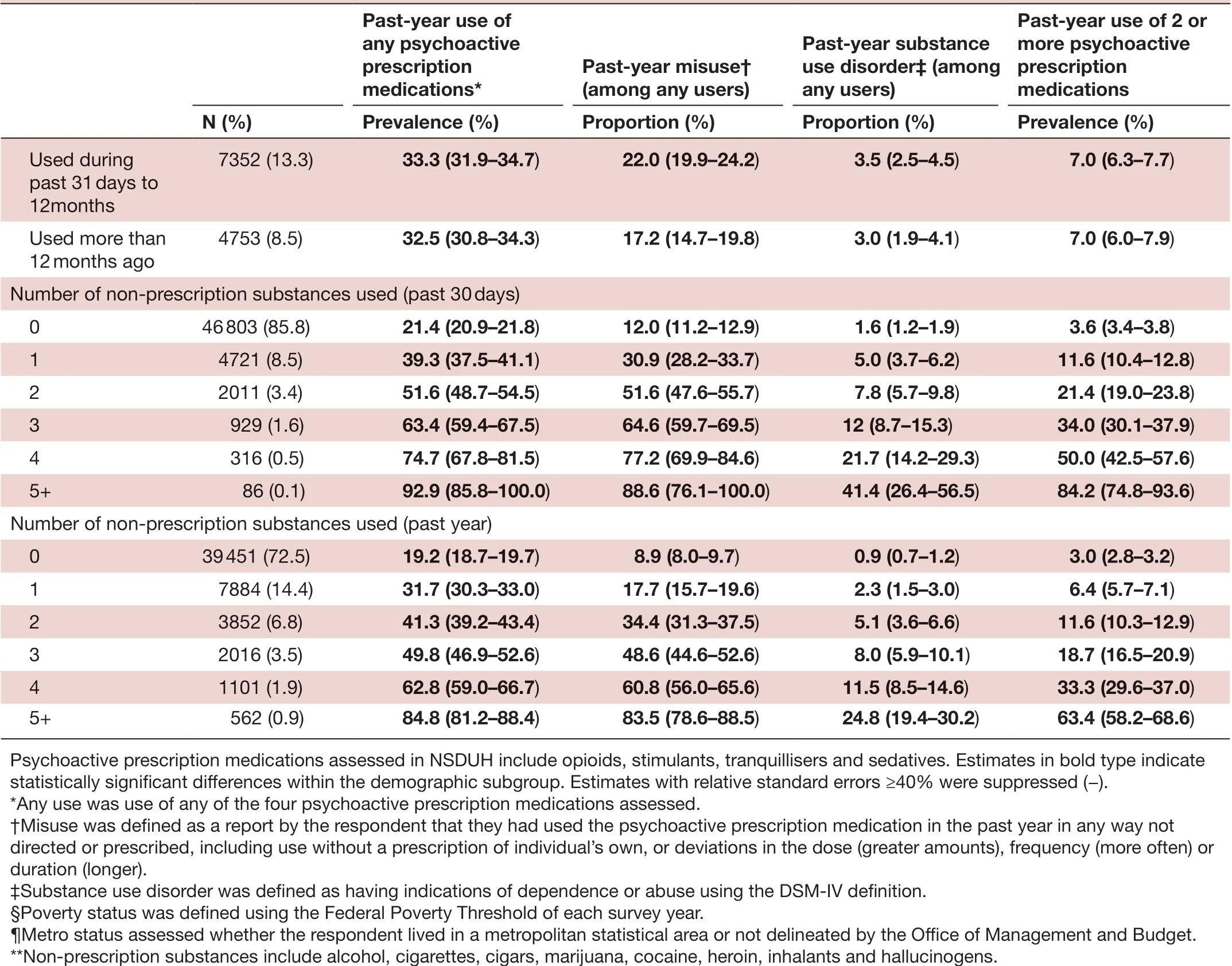
Table 1 Continued
Factors associated with concurrent use of multiple prescription medications
The likelihood of using at least two psychotherapeutics was lower among: men than women (APR=0.95, 95% CI 0.90 to 0.99), each race/ethnic group compared with whites, and non— metropolitan than metropolitan dwellers (APR=0.93, 95% CI 0.86 to 0.99) (table 5). The likelihood of using at least two psychoactive prescrip—tion medications was higher among Medicaid insurees than uninsured persons (APR=1.15, 95% CI 1.04 to 1.27). Individuals with serious psychological distress had over twice the adjusted prevalence of using at least two psychotherapeutics than those without the condition (APR=2.01, 95% CI 1.90 to 2.12). Those who reported use of non— prescription substances also had higher likelihood of using at least two psychotherapeu—tics than those who did not (APR=4.55, 1.92 and 1.76 among past ≤30— day, ≤12— month and >12— month users, respectively).
Non-prescription substance use as a behavioural marker for misuse of psychoactive prescription medications
Measures of recency (never, ≤30 days, ≤12 months or >12 months) of non— prescription substance use and the number of substances used (none, 1,2, 3, 4 or 5+) both were strongly associated with misuse of psycho—active prescription medications. Compared with never users of any non— prescription substance, corresponding prevalence ratios for past ≤30 days, ≤12 months, >12 months were as follows for misuse of opioids (APRs=8.26, 2.75 and 2.41 (all statistically significant)), stimulants (APRs=34.42, 6.11 and 1.83 (first two statistically signif—icant, last not significant)), tranquillisers (APRs=27.42, 5.66 and 2.93 (all statistically significant)) and sedatives (APRs=5.79, 1.62 and 1.52 (first statistically significant, last two not significant)) (table 5). When examined by individual substances and adjusting for all other assessed products, the strongest determinant of prescription opioid misuse was heroin use (APRs=6.17, 7.21 and 1.48) (table 6). Marijuana use had the strongest associationwith every other psychoactive prescription medication misuse, including stimulants (APRs=5.37, 5.10 and 2.74), tranquillisers (APRs=5.81, 4.61 and 2.75) and sedatives (APRs=5.25, 3.14 and 2.85).
百里柳江奔流向东,两岸的风光决胜千里,壮族的歌,侗族的楼,苗族的舞,瑶族的节,柳州的民族风情四绝沿着柳江展开,满载的货物沿着柳江款款而来,一曲歌声悠扬,一派彩衣霓裳。
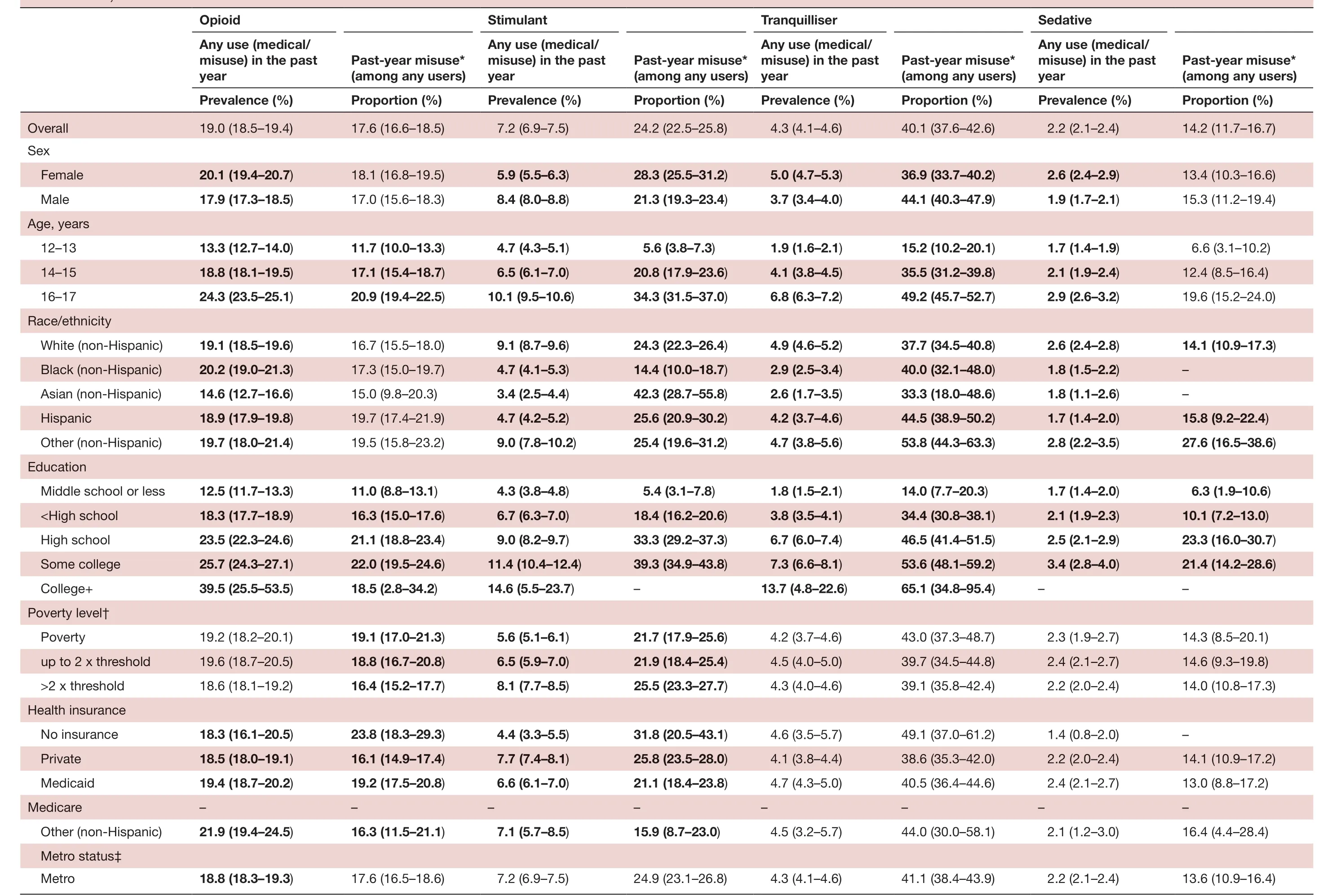
Table 2 Prevalence of use and percentage of misuse by medication and demographic characteristics among US youth aged 12-17 years, National Survey of Drug Use and Health, 2015-2018
Continued
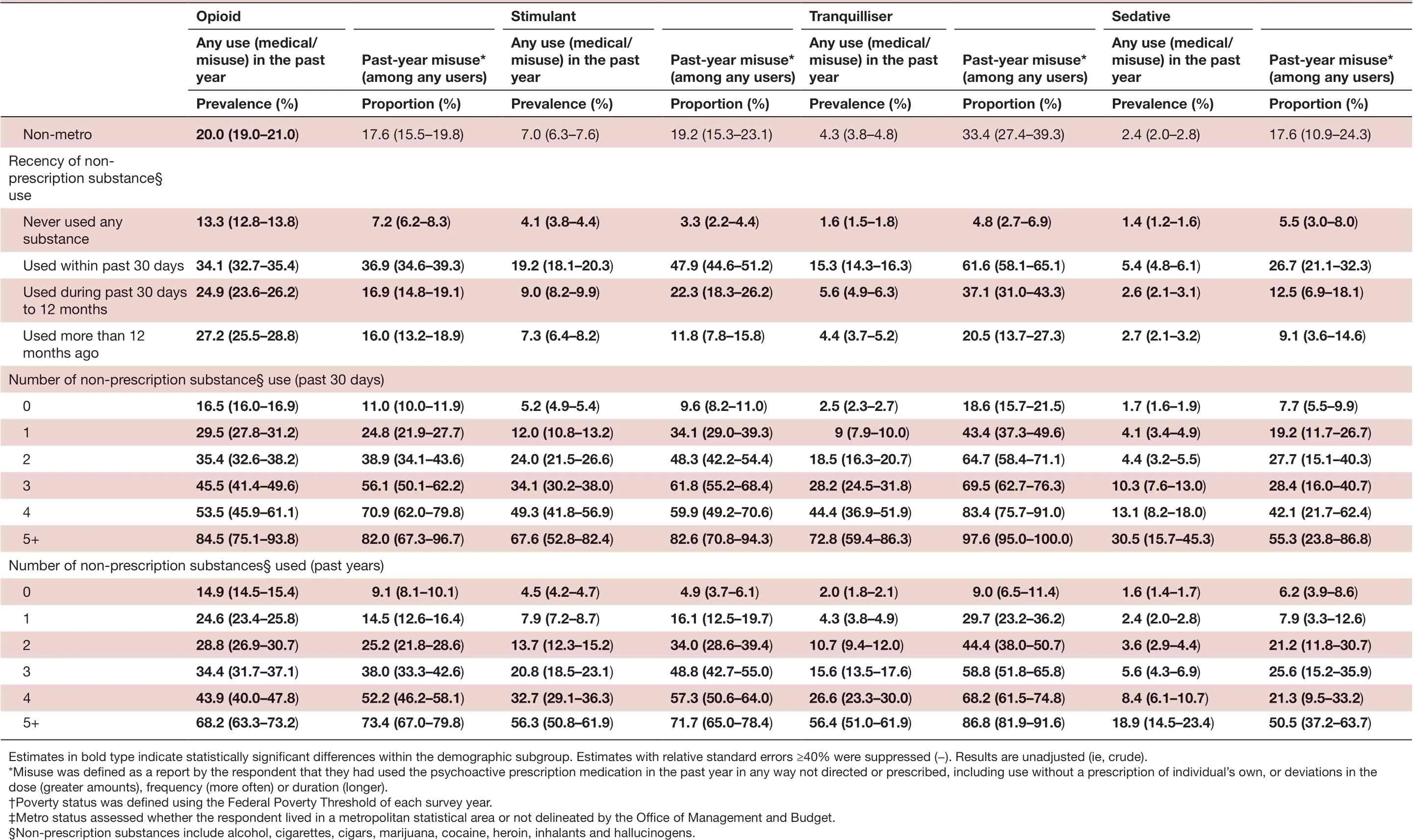
Table 2 Continued
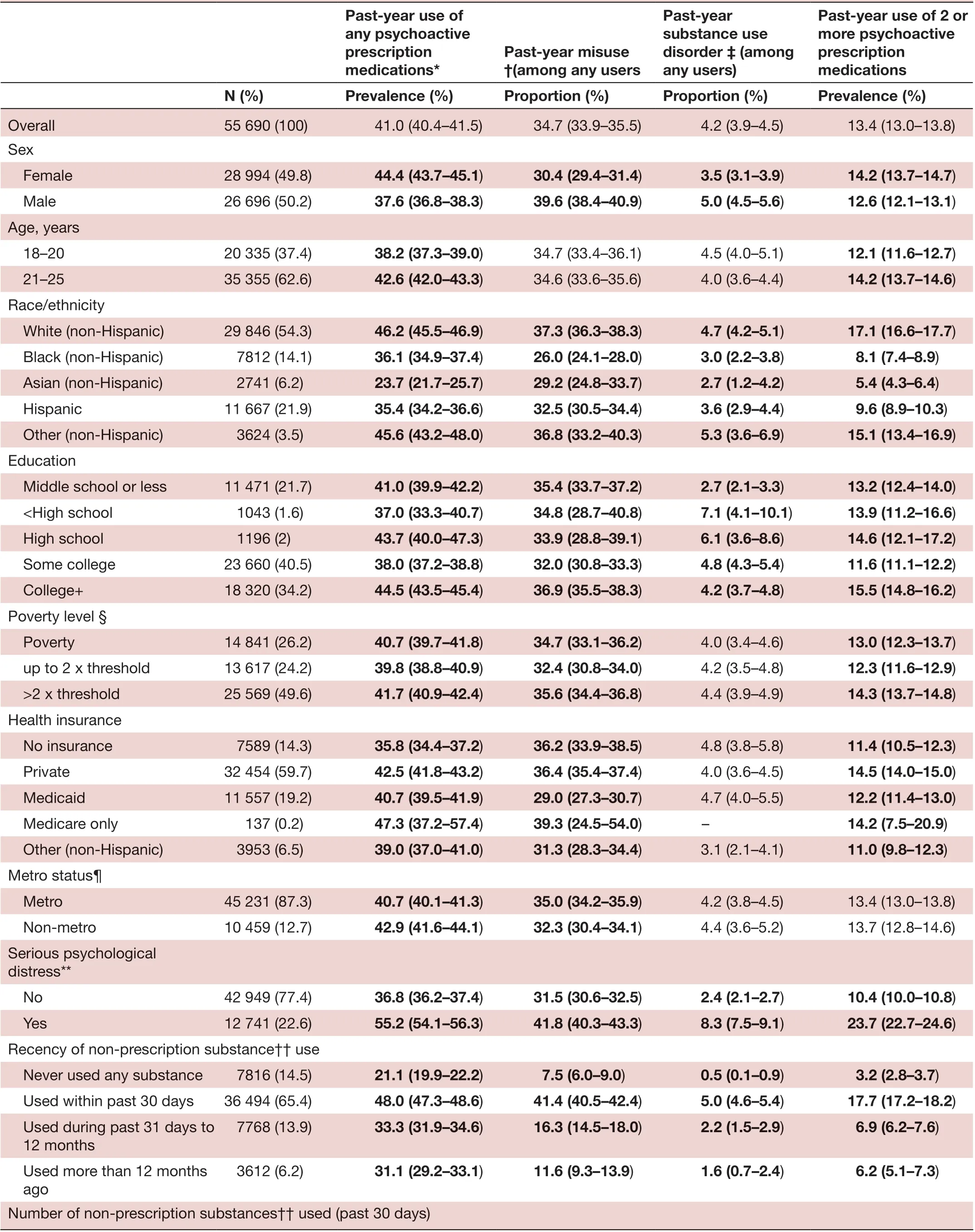
Table 3 Demographic characteristics and usage patterns of any psychoactive prescription medications among US young adults aged 18-25 years, National Survey of Drug Use and Health, 2015-2018
Continued
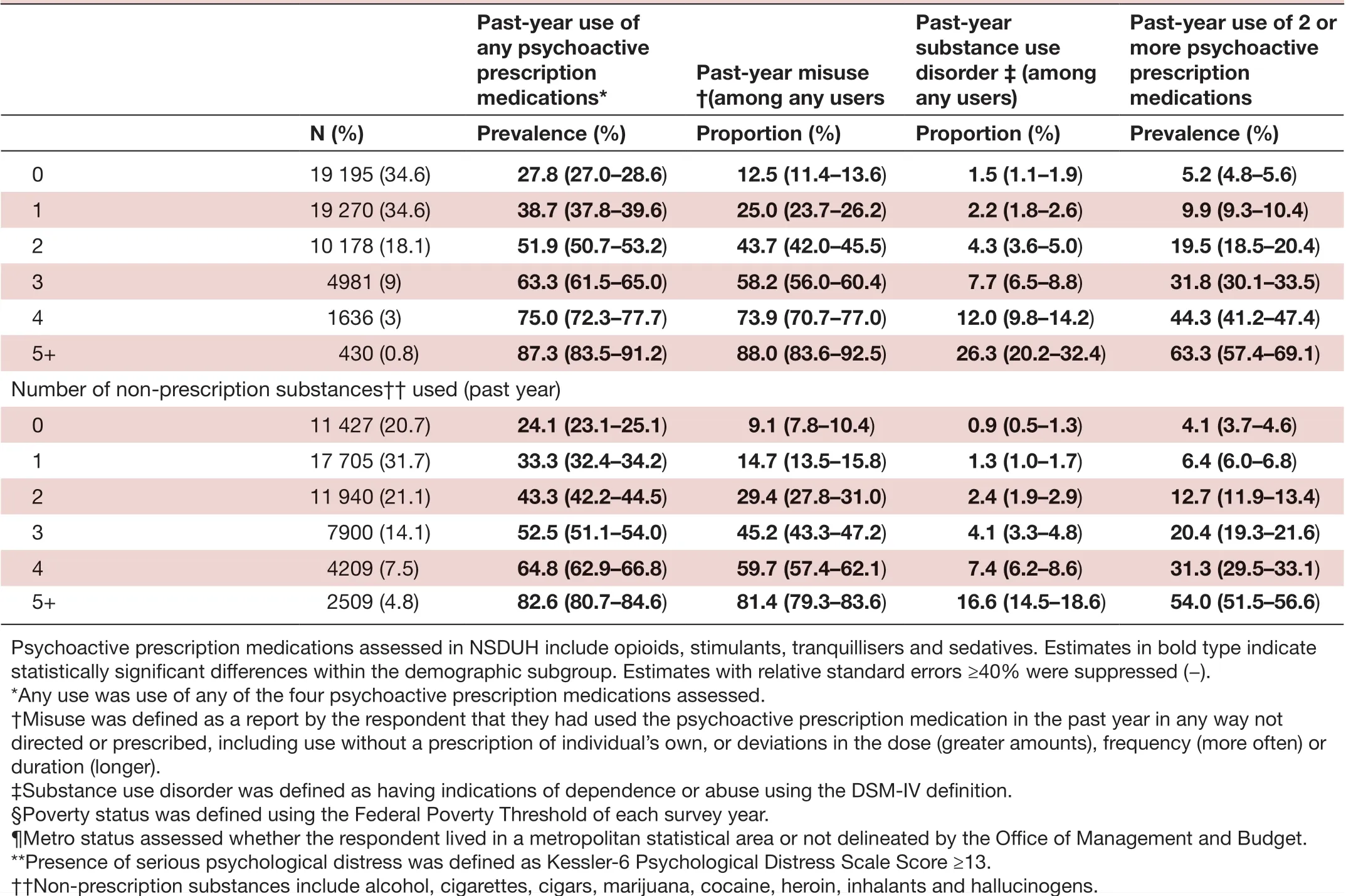
Table 3 Continued
The number of non— prescription substances used was also a significant determinant of psychoactive prescrip—tion medication misuse, regardless of whether tallied within the past 30 days or 12 months. By a past—30— day tally, compared with non— users, likelihood of psychoactive prescription medication misuse among those who used 1, 2, 3, 4 or 5+ non— prescription substances was as follows: opioid misuse (APRs=1.69, 3.44, 6.82, 10.60 and 20.60), stimulants (APRs=4.87, 16.97, 31.44, 58.15 and 104.25), tranquilliser misuse (APRs=2.72, 7.90, 19.25, 35.75 and 80,98) and sedatives (APR=1.20, 2.24, 5.41, 9.04 and 23.03 (first not statistically significant, last four signifi—cant)). Similar results were obtained for a past— year tally.
DlSCUSSlON
Overall, 35.1% of persons aged 12—25 years reported past— year use of a psychoactive prescription medication, and of these, 31.0% reported misusing it. Possible conse—quences of such misuse, especially when co— occurring with multiple psychoactive prescription medications or other non— prescription substances include altered brain development, substance/medication— induced mental disorders, a potential for lifelong addiction, a ‘downward drift’ (ie, a descending social migration and/or loss of social status) and various substance— related diseases.16Individuals with mood and anxiety disorders may engage in drug use to self— medicate or as a mechanism to cope with their mental health disorder.17Misuse of psychoac—tive prescription medications may however make youth and young adults more susceptible to other substance use problems, a phenomenon called the ‘gateway’ effect.18—20It is however also possible that individuals are taking psychoactive prescription medications to manage their anxiety and depression and for some this falls into use and for others into misuse as they actively manage their symptoms rather than strictly sticking to the duration, frequency and quantity as prescribed.
While reported past— year use was highest for prescrip—tion opioids, the estimated percentage reporting misuse was highest for stimulants (44.8%) and tranquillisers (44.4%). The largely overlapping population demo—graphics for medical use versus misuse for each psycho—active prescription medication indicate the high abuse liability of these substances. Over 1 in 10 youth and young adults used at least two psychoactive prescription medi—cations, with a majority of those misusing a psychoactiveprescription medication (57.7%) and a non— prescription substance (86.7%). Individuals with co— occurring substance use disorders have been shown to be more likely to have major depressive episodes in comparison to those with a single substance use disorder.2122Use of multiple substances may also make youth and young adults more dependent, and more difficult for them to quit.2324
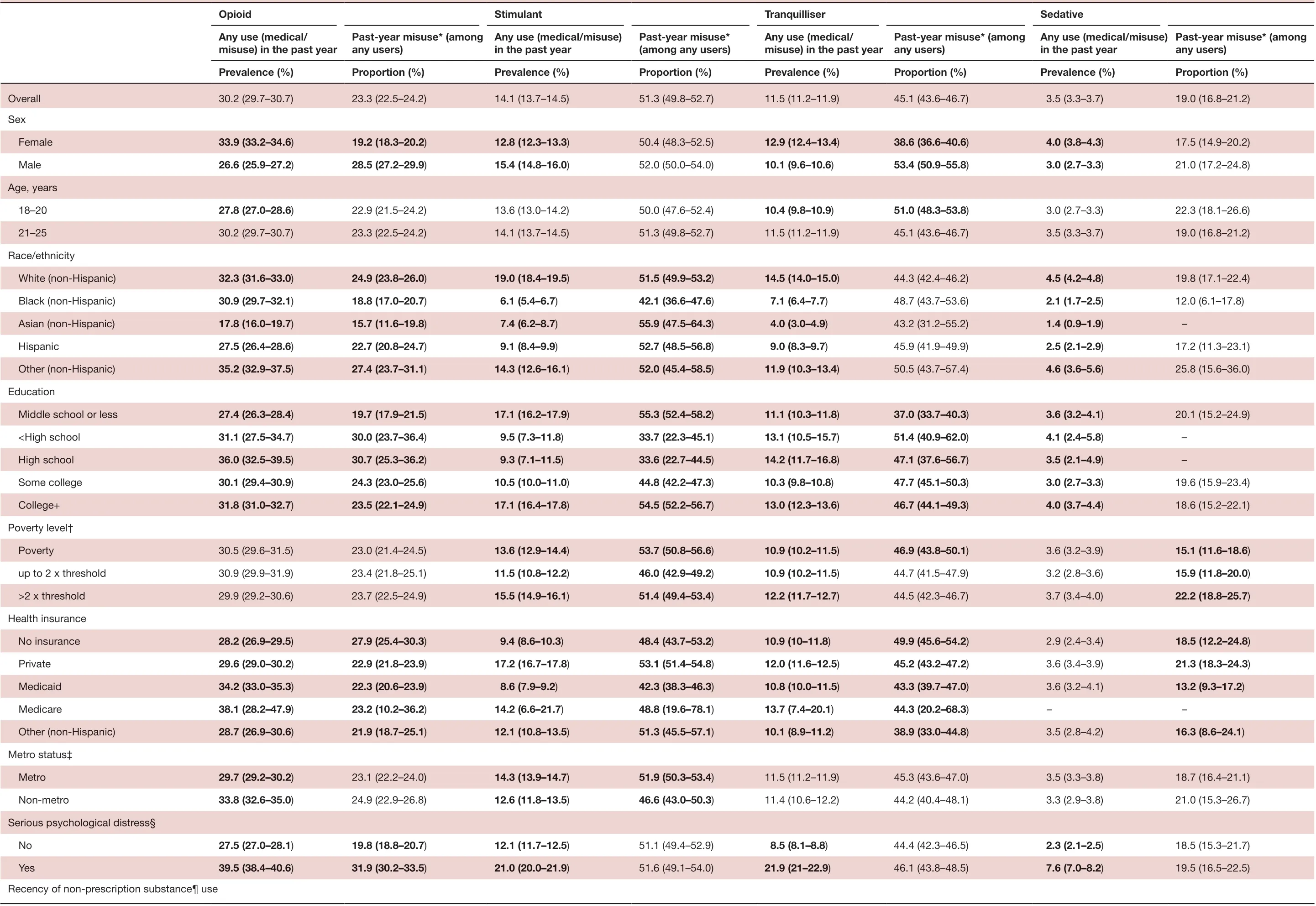
Table 4 Prevalence of use and percentage of misuse by medication and demographic characteristics among US young adults aged 18-25 years, National Survey of Drug Use and Health, 2015-2018
Continued
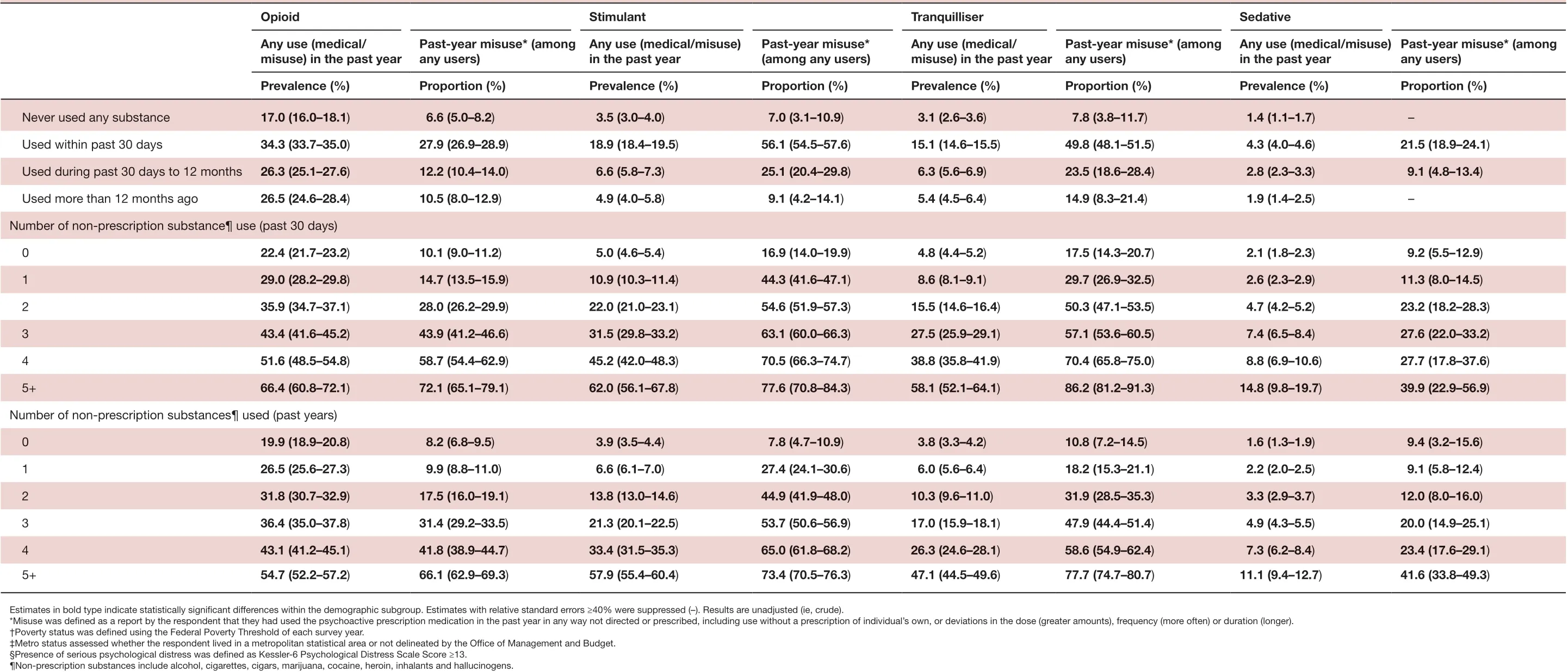
Table 4 Continued

Table 5 Correlates of medical use and misuse of psychoactive prescription medications among US young adults aged 18-25 years, National Survey of Drug Use and Health, 2015-2018
Continued

Use of 2 or more PMs APR (95%CI)Ref.Misuse*APR (95%CI)Ref.Sedatives Medical use*APR (95%CI)Ref.1.19 (0.82 to 1.71) 1.52 (0.33 to 7.05) 1.76 (1.41 to 2.21)Misuse*APR (95%CI)Ref.Tranquilizers Medical use*APR (95%CI)Ref.2.21 (1.85 to 2.64) 27.42 (16.2 to 46.41) 2.03 (1.59 to 2.60) 5.79 (2.42 to 13.84) 4.55 (3.91 to 5.30)1.53 (1.25 to 1.88) 5.66 (3.18 to 10.07) 1.71 (1.28 to 2.28) 1.62 (0.59 to 4.41) 1.92 (1.61 to 2.30)1.52 (1.18 to 1.96) 2.93 (1.41 to 6.08)Misuse*APR (95%CI)Ref.63.06)Stimulants Medical use*APR (95%CI)Ref.Misuse*APR (95%CI)Ref.8.26 (6.37 to 10.71) 2.06 (1.75 to 2.41) 34.42 (18.79 to 2.75 (2.04 to 3.72) 1.41 (1.16 to 1.72) 6.11 (3.22 to 11.62)2.41 (1.69 to 3.42) 1.34 (1.05 to 1.72) 1.86 (0.81 to 4.28)Opioids Medical use*APR (95%CI)Ref.1.42 (1.30 to 1.54) Never used Used in the past 30 days 1.54 (1.44 to 1.66) Used in the past 31 days to 12 months Used in the >12 months 1.46 (1.32 to 1.62) Estimates in bold type indicate statistically significant differences within the demographic subgroup. Results are adjusted for all covariates shown in table.*Misuse was defined as a report by the respondent that they had used the psychoactive prescription medication in the past year in any way not directed or prescribed, including use without a prescription of individual’s own, or deviations in the dose (greater amounts), frequency (more often) or duration (longer). Medical use was defined as having used the psychoactive prescription medication in the past year with no accompanying report of misuse.†Poverty status was defined using the Federal Poverty Threshold of each survey year.‡Metro status assessed whether the respondent lived in a metropolitan statistical area or not delineated by the Office of Management and Budget.§Serious Psychological Distress was assessed with the Kessler Psychological Distress Scale among respondents aged 18-25 years.¶Non- prescription substances include alcohol, cigarettes, cigars, marijuana, cocaine, heroin, inhalants and hallucinogens.
The potential accessibility and affordability of these or similar substances are serious public health issues. In our study, with only a few exceptions, the likelihood of using psychoactive prescription medications and using multiple psychoactive prescription medications was not different by educational attainment and poverty status; or not different among those uninsured versus those with private insurance, suggesting wide accessibility and affordability of psychoactive prescription medications among the public. Recent studies also indicate that youth and young adults could access psychoactive prescription medications without a prescription: during 2017, over half (53.1%) of those who misused prescription opioids obtained them from a friend or relative.2910Taken together with this, efforts to restrict access to prescription medications within clinical settings should be combined with interven—tions that change social norms, and the perceived accept—ability of substance misuse. Such interventions aimed at the entire population, not just youth and young adults, may benefit public health given that most youth and young adults access abuse substances from social contacts, including family members and friends. Consequently, both the youth and young adults who have access and the family members/friends who provide access (regardless of whether they are aware that they are providing access) could benefit from such a social norms intervention. For example, older patients who are prescribed these medi—cations could be encouraged to take more responsibility to keep them locked and out of the hands of youth and young adults.
Our finding that the total number of distinct non— prescription substances used correlated stronger with misuse of psychoactive prescription medications than any individual non— prescription substance use behaviour, could be used as a behavioural marker to identify at— risk youth and young adults. Rather than asking only about cigarette smoking, paediatric practitioners should screen for different commonly used substances, including ‘social use’. Specifically asking youth and young adults if they have used certain substances, including occasional use, is important as those who use such substances infrequently or only occasionally may not self— identify as users if asked in generic terms.25
There is urgent need to address psychological distress among youth and young adults. In our study, 11.5% of persons aged 18—25 years reported having serious psycho—logical distress, and this was a strong determinant of misuse of every prescription substance assessed. Increasing patient motivation and establishing a strong collaborative treatment team are key. Previous research suggests need for integrated treatment (social workers, psychologists,psychiatrists, medical doctors) and treatment plans being individually tailored to simultaneously addressing substance use and mental health symptoms, since the two conditions interact with each other.2627Possible psychological treatment options include behavioural interventions, establishing and identifying social support, utilisation of assessment tools, increase in self— advocacy training, and counselling services (individual, group, family and conjoint) addressing psychoeducation and coping skills.1928Being released after detoxification without ongoing care was found to put patients at an increased risk of relapse and overdose.29In addition to clinical interventions, there is also need for approaches that change social perceptions (including stigma) regarding substance use treatment.1928Due to a lack of substance use education in schools, there are growing misconceptions about substance use, one of the largest being that substance use problems are a result of moral problems and not behavioural problems.30This view places the entirety of the blame on the individual when there could be other extenuating factors.
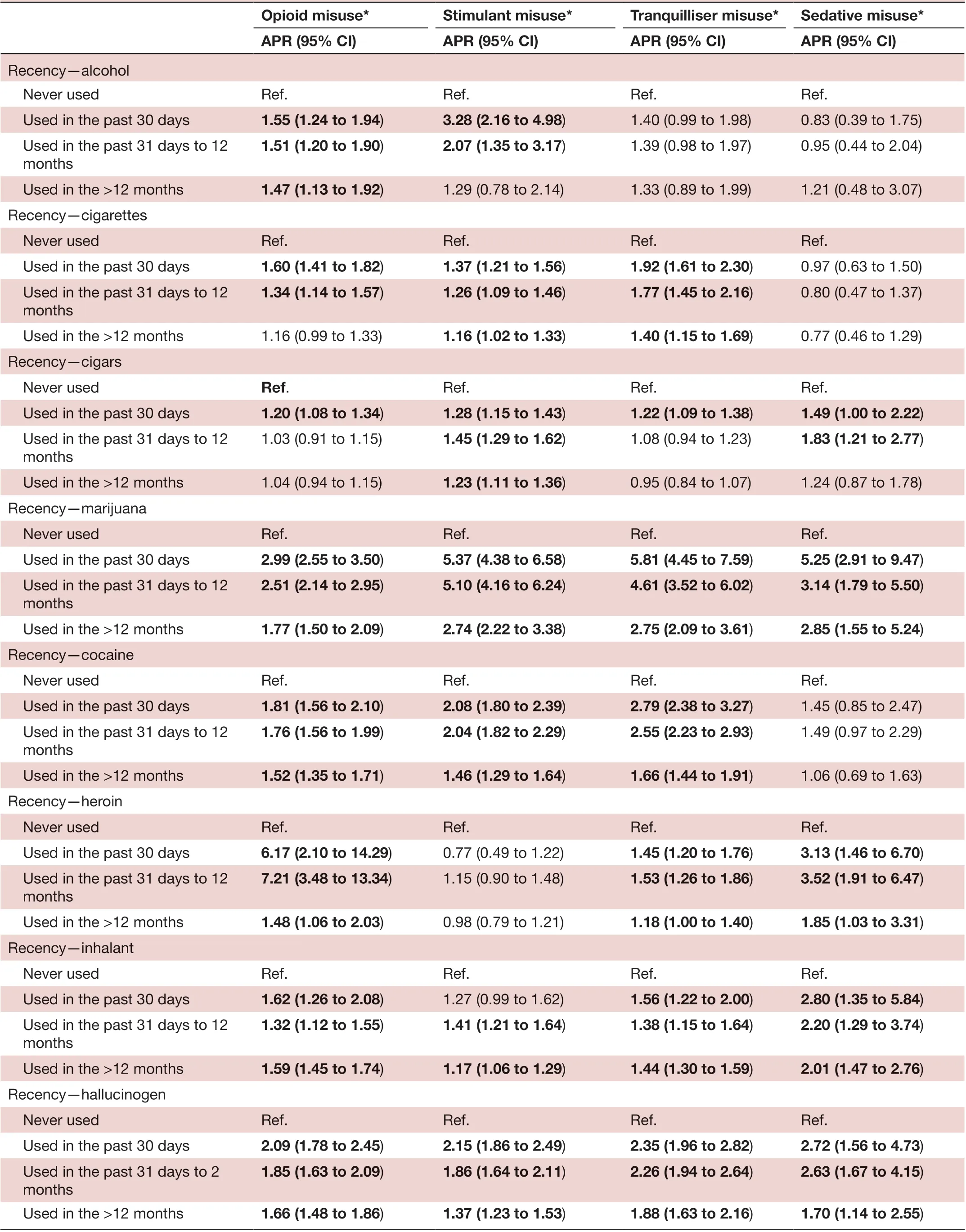
Table 6 Associations between misuse of prescription medications and use of non- prescription substances among US young adults aged 18-25 years, National Survey of Drug Use and Health, 2015-2018
Continued

Table 6 Continued
The findings in this study are subject to certain limita—tions. First, the cross— sectional design and self— reported measures limit inferences to only associations. Second, while accurate, the term misuse is very broad. Those cate—gorised as misusing may be using a psychoactive prescrip—tion medication for legitimate reasons (slight variations from how a psychoactive prescription medication was prescribed) rather than to get high. Third, there was some discrepancy in the time frame for which certain vari—ables were measured. For example, psychological distress was only reported over the last 30 days whereas certain substance use behaviours were measured within the past year. This leads to issues of temporal order in the concur—rent associations (ie, depression could have occurred in the past 30 days but psychoactive prescription medication use 11 months ago).
Conclusion
Over 1 in 10 youth and young adults aged 12—25 years used two or more psychoactive prescription medications concurrently. While reported past— year use was highest for prescription opioids, the estimated percentage of users who reported misuse was highest for stimulants (44.8%) and tranquillisers (44.4%). The largely overlap—ping population profiles for medical use versus misuse indicates the high abuse liability of these prescription substances. Having serious psychological distress was consistently associated with misuse of every assessed psychoactive prescription medication. Mental health and medical providers would benefit from using a team approach and having open communication with other healthcare providers to ensure evidence— based guidelines are used when assessing for and treating mental health and substance use difficulties.
ContributorsIA conceptualised and designed the study and drafted the initial manuscript. SO and JN helped conceptualise the study, assisted in the statistical analyses, and critically reviewed and revised the manuscript. All authors approve the final manuscript as submitted and agree to be accountable for all aspects of the work.
FundingThis survey is sponsored by the Substance Abuse and Mental Health Services Administration.
Competing interestsNone declared.
Patient consent for publicationNot required.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Data availability statementData are available in a public, open access repository. Publicly available secondary data came from the National Survey on Drug Use and Health. All data files are publicly and freely available for download at their website at https://www. datafiles. samhsa. gov/ study- series/ national- survey- drug- use- and- health- nsduh- nid13517.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
猜你喜欢
雪豆月读·中年级(2021年6期)2021-07-29
文史春秋(2019年11期)2020-01-15
创新作文(小学版)(2019年7期)2019-10-12
创新作文(1-2年级)(2019年3期)2019-09-03
戏剧之家(2017年7期)2017-05-12
民族大家庭(2016年3期)2016-03-20
小资CHIC!ELEGANCE(2016年2期)2016-03-11
小学生作文·小学低年级适用(2016年2期)2016-03-07
学苑创造·A版(2009年6期)2009-12-07
 Family Medicine and Community Health2021年1期
Family Medicine and Community Health2021年1期
- Family Medicine and Community Health的其它文章
- Are we Athens or Florence? COVID-19 in historical context
- Comparison of self- report and objective measures of male sexual dysfunction in a Japanese primary care setting: a cross- sectional, self- administered mixed methods survey
- Utilisation of smoking cessation aids among South African adult smokers: findings from a national survey of 18 208 South African adults