
Prevalence of Acne Inversa (Hidradenitis Suppurativa) in China: A Nationwide Cross-Sectional Epidemiological Study
2022-04-15 04:08ZhongShuaiWangJingLiQiangJuWeiLaiSongMeiGengXiaoJingKangXianJiangHongZhongJinHongFuXieQingSunHangLiShanShanLiChenYuanLiHeHongFangGangWangJuanTaoXingHuaGaoYanWuYouKunLinYuZhenLiJunGuYanYanBaoxiWang
国际皮肤性病学杂志 2022年1期
Zhong-Shuai Wang, Jing Li, Qiang Ju, Wei Lai, Song-Mei Geng, Xiao-Jing Kang, Xian Jiang,Hong-Zhong Jin, Hong-Fu Xie, Qing Sun, Hang Li, Shan-Shan Li, Chen Yuan, Li He,Hong Fang, Gang Wang, Juan Tao, Xing-Hua Gao, Yan Wu, You-Kun Lin, Yu-Zhen Li,Jun Gu, Yan Yan,∗, Baoxi Wang,∗
1Department of Dermatology, Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100144, China; 2Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College,Nanjing, Jiangsu 210042, China; 3Department of Dermatology, Renji Hospital, Shanghai Jiaotong University School of Medicine,Shanghai 200127, China; 4Department of Dermatology, The Third Affiliated Hospital, Sun Yat-Sen University, Guangzhou,Guangdong 510630, China; 5Department of Dermatology, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an,Shaanxi 710004, China; 6Department of Dermatology, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, Xinjiang 830001, China; 7Department of Dermatology, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, China;8Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100730, China; 9Department of Dermatology, Xiangya Hospital, Central South University, Changsha,Hunan 410008, China; 10Department of Dermatology, Qilu Hospital of Shandong University, Jinan, Shandong 250012, China;11Department of Dermatology, Peking University First Hospital, Beijing 100034, China; 12Department of Dermatology, the First Bethune Hospital of Jilin University, Changchun, Jilin 130021, China; 13Department of Dermatology, First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan 650032, China; 14Department of Dermatology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang 310003, China; 15Department of Dermatology, Xijing Hospital, Air Force Medical University of PLA, Xi’an, Shaanxi 710032, China; 16Department of Dermatology, Union Hospital, Tongji Medical College,Huazhong University of Science and Technology, Wuhan, Hubei 430022, China; 17Department of Dermatology, the First Hospital of China Medical University, Shenyang, Liaoning 110001, China; 18Department of Dermatology, the First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi 530021, China; 19Department of Dermatology, the 2nd Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang 150001, China; 20Department of Dermatology, Shanghai Tenth People’s Hospital, Tenth People’s Hospital of Tongji University, Shanghai 200072, China.
Abstract
Keywords: acne inversa/hidradenitis suppurativa, epidemiology, China
Introduction
Acne inversa(OMIM 142690),also known as hidradenitis suppurativa (HS), is a chronic inflammatory skin disease characterized by recurrent abscesses with draining sinuses and subsequent progressive scars affecting apocrine glandbearing areas of the body.1Patients with HS experience chronic and debilitating pain, and HS has a considerable impact on patients’ quality of life that often exceeds the impact of other chronic skin diseases.2Furthermore,several comorbidities have been reported in patients with HS, including metabolic syndrome, inflammatory bowel disease, and other inflammatory conditions.3-4
The estimated prevalence of HS varies greatly, ranging from 0.00033% to 4.1%; a prevalence of 0.7% to 1.2%was recently reported in United States and European populations.1,5–9Several studies in Western countries have revealed that HS is most prevalent among young adults and more common in women than men.9–13However, such epidemiological data regarding Asian populations remain scarce.A study using national health insurance claims data in Korea revealed a prevalence of 0.06%, which is much lower than that reported in Western countries.14Contrary to the sex ratio reported in Western countries,a remarkable male predisposition was found in Korea and Japan.14–15
To our knowledge,no data on the epidemiology of HS in the Chinese population are available. Therefore, we conducted a multicenter clinic-based cross-sectional study to estimate the prevalence of HS in the Chinese population.We also gathered demographic and clinical features of patients with HS in China to examine sex-related differences and establish risk factors for HS severity.These data will provide a fundamental picture of HS in the Chinese population and help to broaden our understanding of HS.
Material and methods
This study protocol was reviewed and approved by the Ethics Committee of Plastic Surgery Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (Beijing, China), and the ethics committees of all participating hospitals.
Study design
Given the extremely low prevalence rate revealed by population studies in other Asian countries,we decided to employ a multicenter clinic-based cross-sectional survey design. During the study period of September to October of 2020, each visitor at participating dermatology clinics was screened for HS to minimize the number of missed cases.The prevalence of HS was calculated by the number of patients diagnosed with HS as the numerator and the number of unduplicated visitors at all participating dermatology clinics during the same period(obtained from the hospital information system within each hospital) as the denominator. The age and sex distribution of all visitors at participating dermatology clinics were obtained to calculate the age-and sex-specific prevalence of HS.The patients diagnosed with HS were then asked to take part in another questionnaire survey to collect information on the characteristics of HS in the Chinese population.
Study sites and sample size
To increase geographic coverage,the study sites comprised 19 hospitals located in two municipalities(Beijing and Shanghai)and 13 provincial capital cities across all regions of China.Because no data were available on the prevalence of HS in China,the population prevalence of HS in Korea(0.06%)was used as a reference for the sample size calculation.Moreover,the clinic-based prevalence is usually higher than the prevalence in the general population. An estimate of 0.1%was therefore used to calculate the sample size for this study.With a relative error of 0.25,type I error of 0.05,and design effect of 2, the total sample size required was estimated to be 125,000 patients.
Patient recruitment and eligibility criteria
From September to October 2020 at participating dermatology clinics, doctors screened every visitor for their history of HS,presence of cystic acne,and presence of dissecting cellulitis of the scalp.Any patients who possibly had HS were referred to two trained dermatologists,who then independently ascertained the diagnosis of HS. A discussion or consultation with a third dermatologist was performed to resolve any discrepancies and achieve consensus. Inclusion criteria are as follows: (1) patients who meet the diagnosis of HS16; (2) patients who were aged >12 years. The patients who meet the inclusion criteria and provided written consent were enrolled in the study. The study procedure is shown in Figure 1.

Figure 1. Identification and enrollment of patients with HS at dermatological clinics. HS: Hidradenitis suppurativa.
Data collection and management
All participants were interviewed using a structured questionnaire that included several sections covering demographic characteristics, lifestyle factors, historical and clinical features of HS,comorbidities,and impacts on quality of life. All interviews were assisted by a smart phone application with computerized questionnaires incorporating conditional skips and logic checks.
The locally collected data were encrypted and electronically sent to the study team. All paper-based data were double-entered using EpiData software version 3.1(EpiData Association,Odense,Denmark)and checked for errors.
Quality control
A manual of procedures was developed for all components of the study.Each clinic assigned two designated dermatologists for case ascertainment, enrollment, and questionnaire-based interviews. The two dermatologists were trained and certified by the central study team.They served as the master trainers for other doctors and staff regarding the HS diagnostic and screening criteria at each participating clinic. The study staff at local sites were trained on interview skills and the use of standardized protocols and questionnaires for data collection.The survey questionnaire was pretested and revised accordingly before implementation.All questionnaires were checked for completeness and errors before finishing the interviews.Site monitoring was conductedregularlytoensurequality.Informationobtained from the hospital information system was based on unique individuals;that is,duplicates were removed.
Statistical analysis
The primary analysis was performed to calculate the prevalence of HS, which was extrapolated from the percentage of patients with HS among all visitors at participating clinics during the study period regardless of whether they consented to the questionnaire survey. The total,age-specific,and sex-specific prevalence was reported as a percentage with 95% confidence interval (CI). The demographic and clinical features of patients with HS were described using data from the questionnaire survey.Factors associated with disease severity, comorbidities, and Dermatology Life Quality Index questionnaire (DLQI) scores were assessed using the chi-square test.A two-sided P value of<0.05 was considered statistically significant.
Results
HS Prevalence
Among 274,742 patients who presented to the 19 participating dermatology clinics during the study period,113 patients were suspected to have HS,and the diagnosis was confirmed in 92. The latter number was used as the numerator to calculate the crude prevalence of HS. Of these 92 patients,87 gave their consent to take part in the questionnaire survey and were included in the full analysis set (Fig. 2).
The prevalence of HS among dermatology clinic visitors was 33.49(95%CI,26.64–40.32)per 100,000 population.The prevalence rate in southern China was slightly higher than that in northern China, but the difference was not statistically significant(P>0.05).The prevalence was 65.14(95%CI,49.78–80.51)per 100,000 among male patients and 13.76 (95% CI, 7.87–19.64) per 100,000 among female patients,and the female:male ratio was 1.0:4.7.The highest prevalence was found in the 16- to 19-year age group(62.72 per 100,000)followed by 20-to 29-year age group (60.09 per 100,000). The prevalence declined with age(Table 1).
Demographic characteristics and lifestyle
Most of the 87 patients with HS were male(77.0%)and of Han Chinese ethnicity(86.2%).Their median age was 27 years[interquartile range(IQR),22–32years].Their mean body mass index was 26.0kg/m2(IQR,22.4–29.2kg/m2),and60.9%ofthepatientswereoverweightorobese.Almost half(49.4%)were current or past smokers(Table 2).
The median age at disease onset was 18years(IQR,15–23years; range, 11–40years). The median duration between onset and diagnosis was 6years(IQR,2–10years).
Twelve (13.8%) patients reported a positive family history in first-degree relatives, four (4.6%) reported a positive family history in second-degree relatives,and two(2.3%) reported a positive family history in third-degree relatives. More than 70% of patients claimed that no relative had a history of HS.

Figure 2. Patients attending participating clinics during the study period.
The median improvement in the Sartorius score was 27.0 points (IQR, 15–52 points), and the median visual analog scale score for pain was 4(IQR,2–6).Most patients had Hurley stage II disease (n=52, 59.8%). The most common comorbidity was overweight/obesity (n=53,60.9%); other comorbidities included spondyloarthropathy or pain, enteritis or chronic abdominal pain and diarrhea, and polycystic ovarian syndrome (female patients only). The median number of affected areas was 3 (IQR, 2–4), and the most prevalent site was the axillae(64.4%),followed by the groin(39.1%),buttocks(39.1%), and face (35.6%) (Table 3).

Table 1 Descriptive characteristics of the study population.

Table 2 Demographic characteristics and lifestyles of patients with hidradenitis suppurativa.
Eighty patients reported a recurrent history of HS and a current or previous HS-related medication history. The most frequently reported causes of recurrence or exacerbation of HS were food(60.0%),seasons(57.5%)(38.8%of patients reported disease aggravation in summer),mental factors(52.5%),local pressure or friction(35.0%),and menstruation(female patients only,40.0%).The most common types of therapy were topical (n=59, 73.8%),systemic (n=57, 71.3%), and non-pharmaceutical treatments(n=43,53.8%), including drilling or debridement,laser therapy, photodynamic therapy, and surgery.
Quality of life
The overall impact of HS on patients’ quality of life was evaluated by the DLQI score. Almost half of the patients(43.6%) reported a very large or extremely large effect(DLQI score of >10) of HS, and the median DLQI score was 9.0 (IQR, 6–15; range, 0–27). The responses to the Patient Health Questionnaire-2 indicated that 23.0% of patients had a depression score of 3 to 6, indicating that further screening for depression was required. A small number of patients (n=11, 12.64%) reported that the disease-related costs had a significant financial impact on their family (Table 4).
We found a statistically significant association between the Hurley stage and patients’ quality of life, suggesting that as the Hurley stage increased, significantly more patients claimed great impacts on their quality of life(DLQI score of>10).No significant difference was foundin quality of life among patients of different ages, sexes,body mass indexes, and comorbidities (Table 5).

Table 3 Clinical characteristics of patients with hidradenitis suppurativa.
Discussion
Given the reported very low prevalence of HS in other Asian countries, it was a great challenge financially and logistically to survey a large representative sample of the general population in China. Due to resource limitations,we conducted a clinic-based cross-sectional study at 19 dermatology clinics located in 15 cities across all regions in China. To the best of our knowledge, this is the first epidemiological study on the prevalence of HS in China,which was found to be lower than that reported in Western countries and even some Asian countries like South Korea.Since clinic care-seekers are only a small fraction of the general population and usually symptomatic, the prevalence of HS among clinic-based populations should be higher than that among general population. It suggests that the prevalence of HS in China should be lower than 33.49/100,000 (0.03349%) found in our study.
As with other studies of Asian populations,we found a trend toward male predominance of HS in China. The female:male ratio was in contrast to that in Western countries, where it was about 2:1 to 3:1.1,10,13The predisposition among male patients in China(male:female ratio of 4.7:1.0)was consistent with the male:female ratioof 1.4:1.0 to 5.2:1.0 reported in East and Southeast Asian populations,including the Korean,Japanese,Singaporean,and Malaysian populations14-15,17–19(Table 6). The discrepant sex ratios between Asian and Western populations might be explained by the racial differences and genetic backgrounds. Sex-specific differences in smoking habits might also play an essential role becausethe smoking rates are much higher in the male than female Asian population.20–23

Table 4 Quality of life of patients with hidradenitis suppurativa.
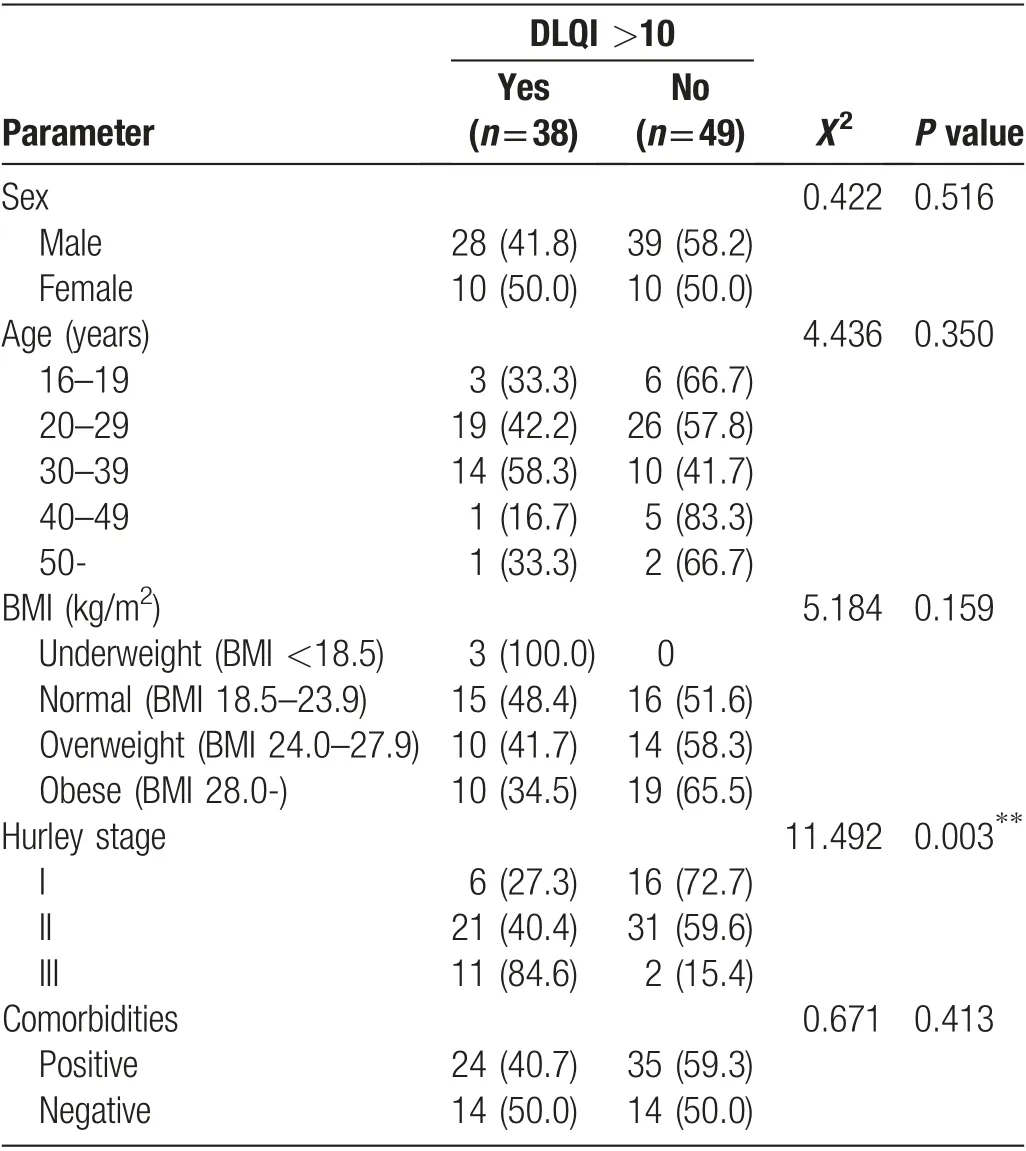
Table 5 Correlation analysis of life quality of patients with hidradenitis suppurativa.

Table 6 Epidemiologic differences among China, East Asia, Southeast Asia, and Western countries.
The anatomical distribution of HS lesions commonly includes the axillae, groin, buttocks, and perineal and perianal regions as reported in previous Western and Asian studies.However,the most frequently affected area differs according to the geographical population. In Western countries,the most prevalent sites are in the order of groin,axillae, and perineal and perianal regions.24-25However,in Korean and Japanese patients, the buttocks are most frequently involved.14,17In our study of the Chinese population, the most frequently affected site was the axillary region followed by the groin and buttocks,similar to some studies in Southeast Asia.18-19
It should be noted that this study was conducted among dermatology clinic visitors, which cannot represent the general population in China. However, this is the first epidemiological study to shed light on the prevalence of HS in China. The study included a large number of leading dermatology clinics across China with the capacity to diagnose HS. Thus, the study provides valuable information on the state of HS in China and calls for further research.The study was conducted in autumn rather than summer, and some patients may have been in remission and not sought healthcare.Moreover,because of the travel restrictions due to the COVID-19 pandemic,patients with mild symptoms may have chosen not to seek healthcare.Both situations may have influenced the prevalence rate found in our study.
Previous large case series of HS showed that more than one-third of patients with HS had a family history in Europe.26–28However, studies of Korean and Japanese populations revealed that only 1.5% to 4.0% of patients with HS had a positive family history.15–17A total of 13.8% of the patients in the present study had a family history, which was lower than that in the European population.The prevalence of patients with HS who have a family history is relatively low in China given that familial HS is related to gamma-secretase gene mutation.29Further studies are required to understand the genetic pathogenesis of the disease.
Acknowledgment
This work was supported by the CAMS Innovation Fund for Medical Sciences(CIFMS)(No.2016-I2M-1-003)and partly by Staidson (Beijing) Biopharmaceuticals Co., Ltd.The authors appreciate the research performed by all the participating dermatologists from the 19 clinics. The authors also thank all the patients for their participation in this study.

- 国际皮肤性病学杂志的其它文章
- Cutaneous Manifestations of HIV/AIDS in the Era of Highly Active Antiretroviral Therapy:Evidence from Bangladesh
- Epidemiology of Pemphigus: A Single Center Experience in Morocco
- Evaluation of Depression and Quality of Life in Patients With Psoriasis
- Nail Psoriasis: Treatment Options and Management Strategies in Special Patient Populations
- Concurrence of Merkel Cell Carcinoma and Squamous Cell Carcinoma in A Patient with Generalized Actinic Keratosis: A Case Report
- Bowen’s Disease on the Left Fifth Finger Successfully Treated with Photodynamic Therapy: A Case Report