暴食症的影响因素及其机制*
2016-02-01 02:32
心理科学进展 2016年1期
(西南大学心理学部,重庆 400715)
1 前言
“今天你暴了吗?”逐渐成为暴食症群体打招呼的一种方式,“暴食症”也逐渐为人们所熟知。美国精神学会(American Psychiatric Association, APA)把暴食症(binge eating disorder,BED)定义为反复发作的暴食症状并伴随强烈的沮丧感,个体在进食时通常感觉失去控制,进食大量食物,但与神经性贪食症(bulimia nervosa)不同,暴食者不会采取不恰当补偿措施以防止体重增加,如呕吐、使用导泻剂、过度运动等(APA,2013;张衍,席居哲,2011)。同时暴食症还有其他特点,如进食速度比平时快得多、一直吃到感觉不舒服为止、当生理上觉得不饿时也会进食大量食物、因为吃得多,觉得难堪而单独进食、暴食之后,会厌恶自己,表现出抑郁、内疚和明显的悲痛。根据《诊断与统计手册:精神障碍》第五版(DSM-V)的诊断标准,平均来说,暴食发作的频率为一周至少一次,且持续3个月。此外除了暴食发作的平均频率达不到一周一次或者持续时间少于3个月,而其他都符合暴食症的诊断标准,这种暴食行为被划分为其他特定的进食障碍(other specified feeding or eating disorder)。
世界健康组织(World Health Organization)对14个国家的调查发现,暴食症在全球的发生率约为1.4%(0.8%~1.9%),发病的平均年龄约为23岁(Kessler et al.,2013)。在西方,暴食症是一种常见的进食障碍,一般人群的终身患病率(lifetime prevalence)接近3%(Hudson,Hiripi,Pope,&Kessler,2007)。国内以2103名青少年为样本的进食障碍调查研究发现,0.7%的青少年符合暴食症诊断标准(Chen &Jackson,2008)。暴食症多发生在年轻的成年人群、女性群体、大学生群体以及受过大学教育的人群中(Kessler et al.,2013)。虽然男性和女性的暴食发作频率相似,但男性较少为之苦恼,因此达不到暴食症的诊断标准(Lewinsohn,Seeley,Moerk, &Striegel-Moore,2002)。
2 暴食的影响因素
近几年的研究发现,影响暴食症的因素多种多样,概括起来主要有以下几类:应激、人格特质、社会文化以及家庭因素。
2.1 应激因素
研究发现,压力或应激(stress)是暴食症发作的风险因素。有暴食行为的个体报告了更多的生活事件压力,更多的把日常生活困难评价为压力(Crowther,Sanftner,Bonifazi,&Shepherd,2001; Wolff,Crosby,Roberts,&Wittrock,2000),同样,感知到高水平压力的个体表现出较严重的暴食行为(Mason&Lewis,2015;Zhu et al.,2015)。一项研究中,研究者让暴食者完成特里尔社会应激测试(trier social stress test,TSST),其中包含一个自由演讲任务和一个心算任务,然后食用巧克力布丁。研究结果发现,与非暴食者相比,暴食者有较高的摄食率,压力增加了暴食者的进食(Laessle& Schulz,2009)。此外有研究用冷压痛任务(cold pressor task,CPT)诱导应激,结果发现完成任务后,暴食者个体的皮质醇(cortisol)水平升高,但是与控制组比较没有显著差异(Schulz,Laessle,& Hellhammer,2011)。这种不一致的结果可能是研究方法不同带来的,特里尔社会应激任务带来的压力主要属于社会性压力,而冷压痛任务带来的更多的是身体上的压力。急性事件导致的压力与日常困扰产生的压力不同,应对方式也不一样,它们对暴食者进食行为的影响也会不同。探讨压力与进食在暴食者身上的关系时,要考虑压力或应激的性质差异。
研究者很早就发现,负性情绪影响暴食行为。暴食症个体报告了更多的悲痛,对负性情绪有较低水平的耐受力(Kenardy,Arnow,&Agras, 1996),更有可能用进食的方式来应对负性情绪(Eldredge&Agras,1996)。一部分研究发现,暴食前个体有较高水平的负性情绪,总体的负性情绪和内疚感较高,但是暴食行为发生后,这些负性情绪就会下降(Berg et al.,2015)。对肥胖的暴食个体来说,在负性情绪水平高或增加的时候,会有更多的暴食行为(Berg et al.,2014)。暴食症个体在正常的进食后,负性情绪和总体的情绪紊乱也会下降(Anderson,Crow,&Peterson,2014)。而一项元分析研究发现,有非特定暴食行为(unspecified binge eating)的个体在暴食后对负性情绪的评价比暴食前的评价更高(Haedt-Matt&Keel,2011)。负性情绪与暴食的关系不是简单的因果关系,两者可能会相互影响。个体在体验的负性情绪后,可能会采用大量进食的暴食行为来缓解消极情绪,但暴食行为并不能真正解决负性情绪背后的问题事件,而暴食行为本身也可能引起负性情绪,因此,在发生暴食行为后,一些个体可能会陷入更强的负性情绪中。
2.2 人格特质
暴食症的一个显著特征是在进食过程中失去控制感(APA,2013)。在暴食的发作和维持中,冲动性(impulsivity)是一个非常重要的因素(Meule& Platte,2015;Schag,Teufel,et al.,2013)。一般认为,冲动性是一种人格特质,由两部分组成,一是奖赏敏感性(reward sensitivity),力求欲望或奖赏刺激;另一部分是自发冲动行为(rash-spontaneous behavior),行动不计后果,抑制控制能力差(Dawe &Loxton,2004)。研究发现,暴食个体有较高的奖赏敏感性(Schienle,Schäfer,Hermann,&Vaitl, 2009)和较高的冲动行为(Schag,Teufel,et al.,2013; Wu et al.,2013)。一项针对暴食行为的元分析研究发现,暴食者具有较高的食物相关的冲动性(Schag,Schönleber,Teufel,Zipfel,&Giel,2013)。
实验室的研究也发现了,冲动性在暴食中发挥着重要的作用。在一项实验研究中,研究者使用自由探索范式(free exploration paradigm)研究了暴食症个体的奖赏敏感性。在实验中,24对食物与非食物图片随机呈现,志愿者自由观看出现的图片,同时用眼动仪记录其眼动轨迹。研究结果发现,肥胖的暴食个体对食物图片的总注视时间要显著长于肥胖的非暴食个体和正常体重的非暴食个体(Schag,Teufel,et al.,2013),这种总注视时间代表了意识和持续注意,表明对刺激的偏好和大脑奖赏系统的激活(Castellanos et al.,2009;Giel et al.,2011)。研究者还使用了修改的反向眼跳范式(modified antisaccade paradigm)来研究暴食症个体的自发冲动行为。食物图片或非食物图片随机出现在电脑屏幕的左侧或右侧,要求志愿者避开图片刺激,尽可能快地观看图片刺激的另一侧。实验结果发现,与肥胖的非暴食个体和正常体重的非暴食个体相比,在第一次眼跳时,肥胖的暴食个体较难抑制对食物图片和非食物图片的眼跳,在第二次眼跳时,肥胖的暴食个体对食物图片的眼跳抑制更加困难(Schag,Teufel,et al., 2013)。研究结果证明了在面对食物刺激时,暴食症个体的奖赏敏感性和自发冲动行为增加。在一项功能核磁共振成像(functional magnetic resonance imaging,fMRI)研究中,研究者用颜色Stroop任务考察了暴食症个体在抑制控制时的神经机制(Balodis et al.,2013),研究结果发现,在Stroop任务中,与肥胖的非暴食个体和正常体重的非暴食个体相比,肥胖的暴食个体的腹内侧前额叶皮层(ventromedial prefrontal cortex,vmPFC)、额下回(inferior frontal gyrus,IFG)和脑岛(insula)有更多的激活,这些区域主要涉及自我调节(self-regulation)和冲动控制(Balodis et al.,2013)。
2.3 社会文化因素
近些年来,源于欧美的“瘦”文化开始在全球流行。大众传媒,如电视、电影、电台和报纸等,是社会文化的主要传播载体。电视机作为普遍使用的大众传播媒介,会影响个体的进食习惯,增加高热量食物的摄入(Pearson&Biddle,2011)。研究显示,每周观看电视的总时间与暴食症状显著正相关,即观看电视时间越长,暴食症状越严重(Burmeister&Carels,2014)。在社会大众媒体“以瘦为美”的压力下,越来越多的年轻女性会产生身体不满意(body dissatisfaction),即对自己的身体外貌产生负面的评价(Sonneville et al.,2012)。已有研究发现,身体不满意与暴食行为有很强的相关(Johnson&Wardle,2005)。身体不满意水平较高的个体会报告更多的暴食行为(Gordon,Holm-Denoma,Troop-Gordon,&Sand,2012)。Andrés和Saldaña考察了身体不满意与暴食的关系,他们发现身体不满意可以引起限制性进食(dietary restraint),进而引起暴食 (Andrés&Saldaña,2014)。同时,在这种“瘦”文化的影响下,女性也会进行节食或限制性进食,即限制热量摄入,以保持体身材和体重。有研究数据显示,限制性进食是暴食的一个显著性预测因子(Holmes,Fuller-Tyszkiewicz, Skouteris,&Broadbent,2014;Jacobi,Hayward,de Zwaan,Kraemer,&Agras,2004;Racine,Burt,Iacono, McGue,&Klump,2011;Woods,Racine,&Klump, 2010)。同时在双生子的研究上发现,在限制性进食水平高的情况下,暴食的基因和非共享环境(non-shared environmental)因素作用增加了(Racine et al.,2011)。对具有暴食遗传基因的个体来说,限制性进食是一个很重要的风险因素。由社会文化因素带来的对体重和体型的不满意以及节食行为,往往不是单独发生的。它们的共同作用大大提高了暴食症发生的风险。
人际关系也是影响暴食症的因素。横断研究发现,人际关系问题与进食障碍有关,其中包括暴食(Ambwani&Hopwood,2009;Jackson,Weiss, Lunquist,&Soderlind,2005)。一项研究考察了肥胖个体的人际关系问题与暴食之间的关系,研究结果发现,充满敌意的人际关系与暴食行为和低自尊相关显著,其中,低自尊还是敌意人际关系与暴食行为之间的中介变量(Lo Coco,Gullo, Salerno,&Iacoponelli,2011)。除了肥胖的暴食个体更容易愤怒外,也可能是由于人际关系问题导致低自尊,进而引起暴食行为。人际关系问题更多的是由于个体缺乏必要的社会交往技巧造成的。有一项研究调查了肥胖暴食者的社交技能,结果发现,那些不自信、情感表达能力不足、与陌生人打交道能力差、不能站在他人角度理解问题以及悲痛(distress)水平高的肥胖女性更有可能被诊断为暴食症患者(Duchesne et al.,2012)。缺乏社交能力的个体在人际交往中容易产生挫折,导致自尊下降,进而用暴食行为来缓解人际交往中产生的负性情绪。
2.4 家庭环境
在家庭环境中,父母的喂养方式也会影响子女的进食问题。当子女表现出正确的行为时,父母会用食物给予子女奖励,相反则用剥夺食物作为错误行为的惩罚,这就是所谓的工具性喂养(instrumental feeding)(Rodgers et al.,2013)。有研究已经发现,在儿童期被父母采用过工具性喂养方式的成年人有更多的暴食行为(Puhl&Schwartz, 2003)。最近的一项研究调查了父母的工具性喂养方式、负性情绪以及暴食之间的关系。研究结果发现,高强度的工具性喂养方式增强了负性情绪与暴食之间的关系,同时,当负性情绪较低时,个体报告较少的暴食行为,且与父母的工具性喂养方式无关(Mason,2015)。这表明当父母采用工具性喂养方式时,子女更有可能采用暴食的方式来应对负性情绪。父母长期采用工具性喂养方式,会使子女形成“进食可以作为一种处理问题的方式”的观念。当遇到实际问题产生负面情绪时,子女就很可能采用同样的方式来应对问题。
除了父母的喂养方式外,父母的进食行为也会对子女产生影响。一项在青少年群体中的研究显示,女孩的暴食行为与父亲的暴食行为显著相关(Goldschmidt et al.,2014)。也有以大学生为样本的研究发现,和与父母共同居住的大学生相比,离家独自生活的大学生报告的暴食症状是前者的3倍(Barker&Galambos,2007)。暴食往往是单独进行的,父母的陪伴和监督会减少子女的暴食行为。父母对子女进食行为的影响是双重的。当父母采用不恰当的喂养方式或自身具有进食问题时,子女往往也会表现出较多的进食问题。同时父母也可以监督子女的进食,为其提供正确的处理问题的方式,帮助处理应对消极情绪。
3 暴食症的理论机制
对于暴食行为,研究者提出了多个理论模型来解释这种现象产生和维持的原因和过程,主要有情感调节模型、食物成瘾模型,人际关系理论以及完美主义模型。
3.1 情感调节模型
情感调节模型(affect regulation model)认为,负性情绪的增加引起暴食发作,暴食则通过食物安慰和转移注意来减轻负性情绪(Hawkins& Clement,1984)。在应付负性情绪上,暴食变成了一种条件反射,并通过负性强化加以维持。该理论有两个基本假设:1)负性情绪的增加是暴食的前兆;2)暴食后负性情绪会立即下降。问卷调查研究发现,在开放性问卷中,当问到为什么出现暴食行为时,69%~100%的神经性贪食者和暴食者报告说是负性情绪引起暴食行为(Lynch,Everingham, Dubitzky,Hartman,&Kasser,2000)。实验研究也发现,启动负性情绪或应激,可以增加暴食症个体随后的进食或增加其暴食发作的可能性(Laessle&Schulz,2009)。与中性条件相比,负性情绪条件下的被试体验到更多的暴食发作(Agras &Telch,1998),支持了该理论的第一个假设。而对第二条假设,研究结论却不一致。一些回顾性研究发现,50%~60%的神经性贪食者报告说,暴食后消极情绪减少(Hsu,1990),而也有研究发现, 80%~100%的个体在暴食后负性情绪状态增加(Tachi,Murakami,Murotsu,&Washizuka,2001)。一项元分析研究发现,相对于平均情绪和正常饮食之前的情绪,暴食个体在暴食发作之前有较大的消极情绪,但是也发现,随着暴食发作,负性情绪也会增加(Haedt-Matt&Keel,2011),这与情感调节理论并不一致。暴食个体暴食后负性情绪增加可能是因为暴食后觉得不能控制自己,产生了羞愧体验。关于暴食的情感调节理论还需要进一步完善。
3.2 食物成瘾模型
食物成瘾模型(food addiction model)借鉴了药物成瘾的概念,从成瘾的角度解释暴食发生的原因(Gearhardt et al.,2012;Gearhardt,White,& Potenza,2011;Smith&Robbins,2013)。在该理论中,由于基底多巴胺水平(basal dopamine level)的降低,有药物滥用及肥胖风险的个体可能对奖赏有过高的期望,导致奖赏缺乏状态(Smith& Robbins,2013)。这种状态,无论是意识还是潜意识层面上,都会增加个体药物滥用或美味食物自我治疗(self-medicate)的风险。然而,长期食用糖类/脂肪或者长期服用药物延长了对多巴胺受体的刺激,使这些受体下调(down regulation),引起对多巴胺敏感性的降低,也可能降低对奖赏刺激的反应(Bello,Lucas,&Hajnal,2002)。和药物使用者类似,肥胖个体也可能表现出对食物奖赏的耐受性。无论是药物还是食物,长期食用之后个体都要求更大程度的暴露于奖赏刺激,以得到与之前体验过的相同水平的快乐,导致进食量的增加(Ifland et al.,2009)。这样就可能形成一个恶性循环,需要更大的进食量以抵消增加的耐受性,得到最初由饮食或药物使用体验到的快乐(Smith& Robbins,2013)(图1)。
与成瘾模型相似的刺激敏化理论(incentivesensitization theory)也认为,在特定的环境中,易感个体反复暴露于成瘾物质可以持久地改变大脑细胞和回路,使这些细胞和回路不能正常对刺激的突出性进行调节。这些“神经适应”的特性是补偿大脑回路的高度敏感,这就在病理性水平上导致对药物与药物相关线索的敏感,形成刺激敏化(Robinson&Berridge,2008)。有研究者认为,有过量进食问题的肥胖个体,如暴食,成瘾机制可能在其中起着重要作用(Davis&Carter,2009),敏化意味着药物或其他刺激可以引起大脑异常高水平的活动。高热量食物刺激频繁地与奖赏配对,将会导致多巴胺(dopamine)奖赏系统的刺激敏化,由此造成的结果就是,当个体面对这些刺激时,就会激活奖赏系统,引起生理唤醒,最终导致暴食发生(Schmitz,Naumann,Trentowska,&Svaldi,2014)。
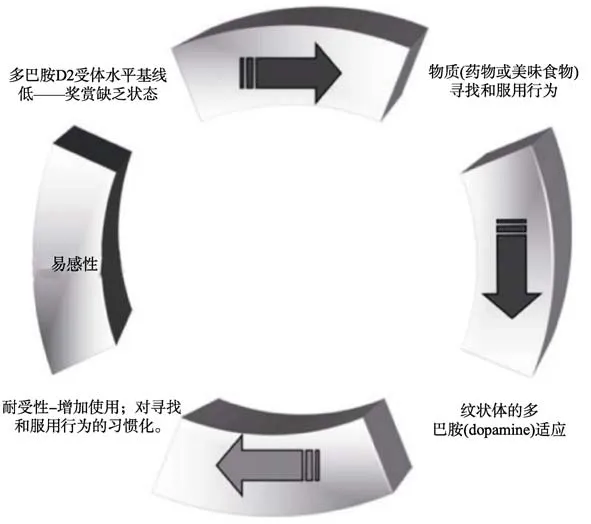
图1 食物成瘾模型(资料来源:Smith&Robbins,2013)
在食物成瘾模型的理论中,戒断(withdrawal)是一个重要的概念。戒断反应是药物依赖的个体复发的一个主要诱因,这些戒断症状是对抗早期高潮体验的生理和心理反应,激发药物使用者服用更多的药物来缓解不愉快症状。通过药物剥夺或对纹状体(striatum)使用阿片受体拮抗剂(opioid receptor antagonists)就会产生戒断反应(Bozarth& Wise,1984),这两种操纵都会使多巴胺(dopamine)减少,乙酰胆碱(acetylcholine)增加,引起抽搐,流汗,呕吐,快感缺乏及消极情感等反应。在动物研究中发现,让大鼠对蔗糖产生暴食后,当取走蔗糖或给大鼠注射阿片受体拮抗剂时,大鼠也会产生类似戒断的症状(Avena,Bocarsly,Rada,Kim,& Hoebel,2008;Cottone,Sabino,Steardo,&Zorrilla, 2008),这与鸦片类物质依赖反应类似。药物依赖者首次接触药物后,随着耐受性的建立,会逐渐增加剂量,最后服用更多的药物。个体以暴食的方式进食,这与药物依赖者的行为一致(Smith& Robbins,2013)。当美味食物可以间歇得到时,尤其是在禁食之后,动物表现出了相似的行为倾向,在一个小时之内,进食量高达日常卡路里的58%(Avena,Rada,&Hoebel,2008;Berner,Avena, &Hoebel,2008)。
有研究使用耶鲁食物成瘾量表(yale food addiction scale,YFAS)测量了暴食者的精神病理。研究结果发现,57%的暴食者被诊断为“食物成瘾”,并且这些人有较高的抑郁、负性情绪、情绪失调以及较低的自尊,YFAS分数比其他测量方式可以更好的预测暴食频率(Gearhardt et al.,2012)。在实验研究中,研究者使用了动物实验中常用的实验范式:过早反应任务(premature responding task)。在实验中,当志愿者在触摸屏幕上看到4个空盒子时,需要按住空格键,随后一个绿色圆圈(目标)会出现在其中的一个空盒子中,志愿者需要松开空格键,然后触摸有目标的盒子。通过测量目标出现到松开空格键之间的时间作为过早反应的指标。研究结果发现,与健康的志愿者相比,酒精依赖者、脱氧麻黄碱(methamphetamine)依赖者和大麻(cannabis)使用者的过早反应较长,但是有暴食症的肥胖者和无暴食症的肥胖者与健康志愿者差异不显著(Voon et al.,2014)。这个研究结果并不支持把暴食症归为食物成瘾的观点。但是也有研究者发现,与控制组相比,暴食症个体对食物刺激存在注意警觉(attentional vigilance),即对食物刺激产生了敏化,这在一定程度上支持了食物成瘾理论(Schmitz et al.,2014)。关于暴食症的食物成瘾理论还需要更多的证据。
3.3 人际关系理论
暴食症的人际关系模型(interpersonal model)最初是针对抑郁提出来的,该理论认为社会交往问题会对进食产生负面影响并会引起暴食(Wilfley et al.,1993,2002)。处理人际关系能力较差的个体有较低的自尊,可能会学会依靠暴食去应对人际交往所产生的苦恼,或者通过暴食来逃避负性情绪(Ansell,Grilo,&White,2012;Ivanova et al.,2015),即在面对人际关系困难时,暴食症个体用食物作为一种处理悲伤情绪的手段(图2)。
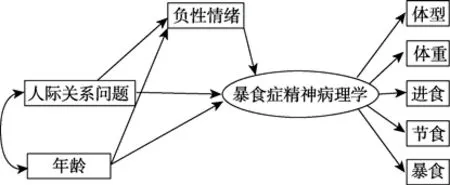
图2 人际关系模型(资料来源:Ivanova et al.,2015)
一些研究结果支持这一模型。Elliott等(2010)在儿童和青少年群体中发现,负性情感调节着社会问题和进食失控(loss of control eating)之间的关系(Elliott et al.,2010)。Ansell等(2012)也在350名青年女性的样本上发现,负性情感可以作为人际问题和暴食症状之间的中介变量。最近一项研究直接检验了人际关系模型在暴食症群体上的适用性。研究结果发现,高水平的人际问题与较高的负性情感相关,而较高的负性情感与高频率的暴食症状有关。人际间的问题可能直接导致了暴食症状(Ivanova et al.,2015)。此外,有研究发现,针对改善人际关系的心理疗法可以有效的治疗成年人的暴食症(Wilson,Wilfley,Agras,&Bryson, 2010),这就支持了人际关系模型。
3.4 完美主义模型
完美主义模型(perfectionism model)是解释完美主义和暴食行为之间关系的综合模型。该模型认为,社会导向的完美主义,即个体知觉到他人要求自己完美,带来了暴食的风险。根据完美主义模型,暴食的因素主要包括4个方面:人际差异(interpersonal discrepancies),低人际自尊(low interpersonal esteem),抑郁情感和限制性进食(Sherry&Hall,2009;Sherry et al.,2014)。具有高社会导向完美主义的个体认为他人要求自己做到绝对完美,致使他们倾向于 认为自己达不到别人的期望。同时,他们的人际自尊也较低,因为他们的社会价值感来自于满足他人提出的不能实现的期望。研究认为人际差异和低人际自尊会引起暴食(Heatherton&Baumeister,1991)。个体在暴食前常常出现抑郁情感(Skinner,Haines,Austin,& Field,2012),而限制性进食也是影响暴食的因素(Racine et al.,2011)。同时该模型也指出了暴食帮助社会导向的完美主义者摆脱厌恶状态,减少或平复抑郁情绪,补偿限制性进食引起的能量不足(Sherry et al.,2014)(图3)。
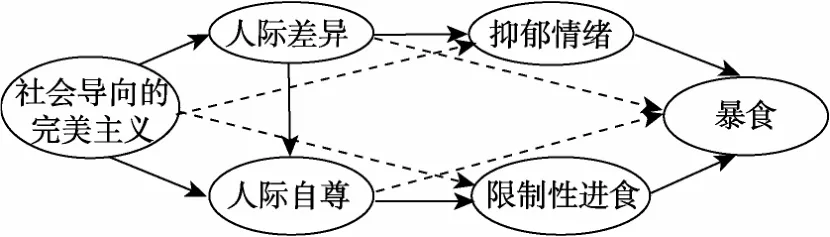
图3 完美主义模型 (资料来源:Sherry&Hall,2009)
Sherry等人(2014)检测了该模型的适用性,他们发现,抑郁情绪可以预测暴食,而焦虑则不可以预测,每个暴食因素都可以单独的促成暴食。除了限制性进食外,其他的因素都可以调节社会导向的完美主义与暴食之间的关系,支持了暴食的完美主义模型(Sherry et al.,2014)。
4 总结与展望
关于暴食症的研究,从最初的访谈、问卷开始,到现在的脑机制研究,在理论和临床应用上都取得了大量成果,但是仍然存在一些尚待解决的问题和需要进一步完善之处,未来的研究可以针对以下几个方面进行深入探讨:
首先,应该继续研究影响暴食症的因素。目前采用的问卷调查研究并没有理清负性情绪与暴食症之间的关系。未来可以采用实验研究方法来探讨它们之间的关系。在对暴食个体的人格研究中,目前主要集中在其冲动性特质上,暴食行为还与其他人格因素有关。纵向研究和横向研究都发现,低自尊是暴食症的一个预测因子(Goldschmidt,Wall, Loth,Le Grange,&Neumark-Sztainer,2012;Grilo, White,&Masheb,2012)。研究者使用内隐联想测验(implicit association test,IAT)也发现,与控制组相比,暴食症个体的外显自尊和内隐自尊都较低(Brauhardt,Rudolph,&Hilbert,2014)。在一项双生子研究中发现,暴食发作与神经质(neuroticism)、经验的开放性(openness to experience)、控制/冲动呈显著正相关,与外向性(extraversion)、宜人性(agreeableness)、责任心(conscientiousness)呈负相关,其中神经质、责任心与暴食发作的相关最强(Koren et al.,2014)。在进食障碍的发展过程中,人格特质可能有着独特作用。加大对暴食症与人格关系的研究,有利于早期识别暴食症的潜在人群。
第二,要完善关于暴食症的理论模型。情感调节模型、人际关系模型以及完美主义模型虽然从不同的角度解释了暴食症发生的原因,同时它们共同强调了负性情绪在暴食的发生与维持上充当着重要的角色。食物成瘾模型则是从“成瘾”的角度来解释暴食症发生的原因,认为高热量美味食物具有“成瘾物质”类似的特性,会使易感人群形成依赖,最后形成食物成瘾。所以未来的理论模型构建可以充分考虑“负性情绪”、“成瘾物质”以及“易感特质”这三方面的特性,构建更全面的理论模型。
第三,要借助先进仪器研究暴食的认知神经机制。研究者使用功能核磁共振(fMRI)技术研究发现,与超重和较瘦的非暴食者相比,肥胖的暴食者面对食物线索时,与奖赏有关的眶额叶皮层(orbitofrontal cortex,OFC)活动增强(Schienle et al., 2009)。在Stroop任务中,暴食个体更多的抑制与自我调节和冲动控制有关的区域,如额下回和脑岛等(Balodis et al.,2013)。基于体素的形态学研究(voxel-based morphometry,VBM)发现,暴食者的眶额叶皮层灰质体积较大(Schäfer,Vaitl,& Schienle,2010),这可能是造成个体暴食的原因,但是目前还缺少直接的证据。未来进一步研究应该采用多种技术手段,如fMRI和事件相关电位(ERP),深入研究暴食个体的脑机制,不仅要加强脑功能的研究,也要包括脑结构的研究,这样有助于对暴食症个体的诊断和治疗。
最后,对暴食行为的研究还要从预防和干预的角度展开,为暴食症患者提供具体的指导和帮助。在暴食症的干预治疗研究中,常见的方法有自助式认知行为疗法(cognitive behavioral guided self-help,CBTgsh)和动机性访谈疗法(motivational interviewing,MI)。自助式认知行为疗法是一种基于认知?行为疗法(cognitive-behavioral therapy)的治疗方法(Wilson et al.,2010;Zendegui,West,& Zandberg,2014)。研究发现,CBTgsh在治疗暴食症上,暴食个体的节制比率为28%到58%,在贪食症上的节制比率为11%到44%(Zendegui et al., 2014)。动机性访谈疗法是一种以临床为中心的心理疗法,它通过使用共情和指导技术,增加个体的内部动机达到改变的目的(Vella-Zarb,Mills, Westra,Carter,&Keating,2015)。有研究考察了MI治疗暴食症的效果,研究结果发现,与控制组相比,MI组的暴食个体报告了更高的自我效能(self-efficacy),在暴食症状、情绪、自尊和生活质量上也有显著提高(Cassin,von Ranson,Heng, Brar,&Wojtowicz,2008)。但是最近的一项实验研究却发现,MI可以增加动机和自我效能,但是在治疗暴食症上效果不显著(Zendegui et al.,2014)。动机性访谈疗法还需要进一步的改进,以提升其治疗暴食症的效果。此外基于冥想(mindfulness)的疗法,在减少暴食症的冲动进食、解决一些行为和情绪失调上也有很好的临床治疗效果(Kristeller, Wolever,&Sheets,2014;Svaldi&Naumann,2014)。研究者虽然在暴食症的治疗上取得了一些成果,但在暴食症的早期发现和预防上研究较少。未来应该在暴食症的早期发现、干预和治疗上开展进一步的研究。
张衍,席居哲.(2011).暴食症的诊断、治疗及其疗效.心理科学,34(6),1508–1511.
Agras,W.S.,&Telch,C.F.(1998).The effects of caloric deprivation and negative affect on binge eating in obese binge-eating disordered women.Behavior Therapy,29(3), 491–503.
Ambwani,S.,&Hopwood,C.J.(2009).The utility of considering interpersonal problems in the assessment of bulimic features.Eating Behaviors,10(4),247–253.
Anderson,L.M.,Crow,S.J.,&Peterson,C.B.(2014).The impact of meal consumption on emotion among individualswith eating disorders.EatingandWeight Disorders-StudiesonAnorexia,BulimiaandObesity, 19(3),347–354.
Andrés,A.,&Saldaña,C.(2014).Body dissatisfaction and dietary restraint influence binge eating behavior.Nutrition Research,34(11),944–950.
Ansell,E.B.,Grilo,C.M.,&White,M.A.(2012). Examining the interpersonal model of binge eating and lossofcontrolovereating in women.International Journal of Eating Disorders,45(1),43–50.
American Psychiatric Association.(2013).Diagnostic and statistical manual of mental disorders:DSM-5.Washington, DC:American Psychiatric Publishing.
Avena,N.M.,Bocarsly,M.E.,Rada,P.,Kim,A.,&Hoebel, B.G.(2008).After daily bingeing on a sucrose solution, food deprivation induces anxiety and accumbens dopamine/acetylcholine imbalance.Physiology&Behavior, 94(3),309–315.
Avena,N.M.,Rada,P.,&Hoebel,B.G.(2008).Evidence for sugar addiction:Behavioral and neurochemical effects of intermittent,excessive sugar intake.Neuroscience& Biobehavioral Reviews,32(1),20–39.
Balodis,I.M.,Molina,N.D.,Kober,H.,Worhunsky,P.D., White,M.A.,Sinha,R.,...Potenza,M.N.(2013). Divergent neural substrates of inhibitory control in binge eating disorder relative to other manifestations of obesity.Obesity,21(2),367–377.
Barker,E.T.,&Galambos,N.L.(2007).Body dissatisfaction, living away from parents,and poor social adjustment predict binge eating symptoms in young women making the transition to university.JournalofYouthand Adolescence,36(7),904–911.
Bello,N.T.,Lucas,L.R.,&Hajnal,A.(2002).Repeated sucrose access influences dopamine D2 receptor density in the striatum.Neuroreport,13(12),1575–1578.
Berg,K.C.,Crosby,R.D.,Cao,L.,Crow,S.J.,Engel,S.G., Wonderlich,S.A.,&Peterson,C.B.(2015).Negative affect prior to and following overeating-only,loss of control eating-only,and binge eating episodes in obese adults.International Journal of Eating Disorders,48(6), 641–653.
Berg,K.C.,Peterson,C.B.,Crosby,R.D.,Cao,L.,Crow,S. J.,Engel,S.G.,&Wonderlich,S.A.(2014).Relationship between daily affect and overeating-only,loss of control eating-only,and binge eating episodes in obese adults.Psychiatry Research,215(1),185–191.
Berner,L.A.,Avena,N.M.,&Hoebel,B.G.(2008). Bingeing,self-restriction,and increased body weight in rats with limited access to a sweet-fat diet.Obesity,16(9), 1998–2002.
Bozarth,M.A.,&Wise,R.A.(1984).Anatomically distinct opiate receptor fields mediate reward and physical dependence.Science,224(4648),516–517.
Brauhardt,A.,Rudolph,A.,&Hilbert,A.(2014).Implicit cognitive processes in binge-eating disorder and obesity.Journal of Behavior Therapy and Experimental Psychiatry, 45(2),285–290.
Burmeister,J.M.,&Carels,R.A.(2014).Television use and binge eating in adults seeking weight loss treatment.Eating Behaviors,15(1),83–86.
Cassin,S.E.,von Ranson,K.M.,Heng,K.,Brar,J.,& Wojtowicz,A.E.(2008).Adapted motivational interviewing for women with binge eating disorder:A randomized controlled trial.Psychology of Addictive Behaviors,22(3), 417–425.
Castellanos,E.H.,Charboneau,E.,Dietrich,M.S.,Park,S., Bradley,B.P.,Mogg,K.,&Cowan,R.L.(2009).Obese adults have visual attention bias for food cue images: Evidence for altered reward system function.International Journal of Obesity,33(9),1063–1073.
Chen,H.,&Jackson,T.(2008).Prevalence and sociodemographic correlates of eating disorder endorsements among adolescents and young adults from China.European Eating Disorders Review,16(5),375–385.
Lo Coco,G.,Gullo,S.,Salerno,L.,&Iacoponelli,R.(2011). Theassociation among interpersonalproblems,binge behaviors,and self-esteem,in the assessment of obese individuals.Comprehensive Psychiatry,52(2),164–170.
Cottone,P.,Sabino,V.,Steardo,L.,&Zorrilla,E.P.(2008). Opioid-dependent anticipatory negative contrast and binge-like eating in rats with limited access to highly preferred food.Neuropsychopharmacology,33(3),524–535.
Crowther,J.H.,Sanftner,J.,Bonifazi,D.Z.,&Shepherd,K. L.(2001).The role of daily hassles in binge eating.International Journal of Eating Disorders,29(4),449–454.
Davis,C.,&Carter,J.C.(2009).Compulsive overeating as an addiction disorder.A review of theory and evidence.Appetite,53(1),1–8.
Dawe,S.,&Loxton,N.J.(2004).The role of impulsivity in the development of substance use and eating disorders.Neuroscience&Biobehavioral Reviews,28(3),343–351.
Duchesne,M.,de Oliveira Falcone,E.M.,de Freitas,S.R., D'Augustin,J.F.,Marinho,V.,&Appolinario,J.C.(2012). Assessment of interpersonal skills in obese women with binge eating disorder.Journal of Health Psychology,17(7), 1065–1075.
Eldredge,K.L.,&Agras,W.S.(1996).Weight and shape overconcern and emotional eating in binge eating disorder.International Journal of Eating Disorders,19(1),73–82.
Elliott,C.A.,Tanofsky-Kraff,M.,Shomaker,L.B., Columbo,K.M.,Wolkoff,L.E.,Ranzenhofer,L.M.,& Yanovski, J.A. (2010). An examination of the interpersonal model of loss of control eating in children and adolescents.Behaviour Research and Therapy,48(5), 424–428.
Gearhardt,A.N.,White,M.A.,Masheb,R.M.,Morgan,P. T.,Crosby,R.D.,&Grilo,C.M.(2012).An examination of the food addiction construct in obese patients with binge eating disorder.International Journal of Eating Disorders,45(5),657–663.
Gearhardt,A.N.,White,M.A.,&Potenza,M.N.(2011). Binge eating disorder and food addiction.Current Drug Abuse Reviews,4(3),201–207.
Giel,K.E.,Friederich,H.-C.,Teufel,M.,Hautzinger,M., Enck,P.,&Zipfel,S.(2011).Attentional processing of food pictures in individuals with anorexia nervosa—An eye-tracking study.Biological Psychiatry,69(7),661–667.
Goldschmidt,A.B.,Wall,M.,Loth,K.A.,Le Grange,D.,& Neumark-Sztainer,D.(2012).Which dieters are at risk for the onsetofbinge eating?A prospective study of adolescentsand young adults.JournalofAdolescent Health,51(1),86–92.
Goldschmidt,A.B.,Wall,M.M.,Choo,T.-H.J.,Bruening, M.,Eisenberg,M.E.,&Neumark-Sztainer,D.(2014). Examining associations between adolescent binge eating and binge eating in parents and friends.International Journal of Eating Disorders,47(3),325–328.
Gordon,K.H.,Holm-Denoma,J.M.,Troop-Gordon,W.,& Sand,E.(2012).Rumination and body dissatisfaction interact to predict concurrent binge eating.Body Image, 9(3),352–357.
Grilo,C.M.,White,M.A.,&Masheb,R.M.(2012). Significance of overvaluation of shape and weight in an ethnically diverse sample of obese patients with bingeeating disorderin primary care settings.Behaviour Research and Therapy,50(5),298–303.
Haedt-Matt,A.A.,&Keel,P.K.(2011).Revisiting the affect regulation model of binge eating:A meta-analysis of studies using ecological momentary assessment.Psychological Bulletin,137(4),660–681.
Hawkins,R.C.,&Clement,P.F.(1984).Binge eating: Measurement problems and a conceptual model.InThe binge-purge syndrome(pp.229–251).New York:Springer.
Heatherton,T.F.,&Baumeister,R.F.(1991).Binge eating as escape from self-awareness.Psychological Bulletin, 110(1),86–108.
Holmes,M.,Fuller-Tyszkiewicz,M.,Skouteris,H.,& Broadbent,J.(2014).Improving prediction ofbinge episodes by modelling chronicity of dietary restriction.European Eating Disorders Review,22(6),405–411.
Hsu,L.K.G.(1990).Experiential aspects of bulimia nervosa:Implications for cognitive behavioral therapy.Behavior Modification,14(1),50–65.
Hudson,J.I.,Hiripi,E.,Pope,H.G.,Jr.,&Kessler,R.C. (2007).The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication.Biological Psychiatry,61(3),348–358.
Ifland,J.R.,Preuss,H.G.,Marcus,M.T.,Rourke,K.M., Taylor,W.C.,Burau,K.,...Manso,G.(2009).Refined food addiction:A classic substance use disorder.Medical Hypotheses,72(5),518–526.
Ivanova,I.V.,Tasca,G.A.,Hammond,N.,Balfour,L., Ritchie,K.,Koszycki,D.,&Bissada,H.(2015).Negative affect mediates the relationship between interpersonal problems and binge-eating disorder symptoms and psychopathology ina clinicalsample:A test of the interpersonal model.European Eating Disorders Review, 23(2),133–138.
Jackson,T.,Weiss,K.E.,Lunquist,J.J.,&Soderlind,A. (2005).Sociotropy and perceptions of interpersonal relationships as predictors of eating disturbances among college women:Two prospective studies.The Journal of Genetic Psychology,166(3),346–360.
Jacobi,C.,Hayward,C.,de Zwaan,M.,Kraemer,H.C.,& Agras,W.S.(2004).Coming to terms with risk factors for eating disorders:Application of risk terminology and suggestions for a general taxonomy.Psychological Bulletin,130(1),19–65.
Johnson,F.,&Wardle,J.(2005).Dietary restraint,body dissatisfaction,and psychological distress:A prospective analysis.JournalofAbnormalPsychology,114(1), 119–125.
Kenardy,J.,Arnow,B.,& Agras,W.S.(1996).The aversiveness of specific emotional states associated with binge-eating in obese subjects.AustralianandNew Zealand Journal of Psychiatry,30(6),839–844.
Kessler,R.C.,Berglund,P.A.,Chiu,W.T.,Deitz,A.C., Hudson,J.I.,Shahly,V.,...Benjet,C.(2013).The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys.Biological Psychiatry,73(9),904–914.
Koren,R.,Munn-Chernoff,M.A.,Duncan,A.E.,Bucholz, K.K.,Madden,P.A.F.,Heath,A.C.,&Agrawal,A. (2014).Is the relationship between binge eating episodes and personality attributableto geneticfactors?Twin Research and Human Genetics,17(2),65–71.
Kristeller,J.,Wolever,R.Q.,& Sheets,V.(2014). Mindfulness-based eating awareness training(MB-EAT) for binge eating:A randomized clinical trial.Mindfulness, 5(3),282–297.
Laessle,R.G.,& Schulz,S.(2009).Stress-induced laboratory eating behavior in obese women with binge eating disorder.International Journal of Eating Disorders, 42(6),505–510.
Lewinsohn,P.M.,Seeley,J.R.,Moerk,K.C.,&Striegel-Moore,R.H.(2002).Gender differences in eating disorder symptomsin young adults.InternationalJournalof Eating Disorders,32(4),426–440.
Lynch,W.C.,Everingham,A.,Dubitzky,J.,Hartman,M.,& Kasser,T.(2000).Does binge eating play a role in the self-regulation of moods?Integrative Physiological and Behavioral Science,35(4),298–313.
Mason,T.B.(2015).Parental instrumental feeding,negative affect,and binge eating among overweight individuals.Eating Behaviors,17,107–110.
Mason,T.B.,&Lewis,R.J.(2015).Minority stress and binge eating among lesbian and bisexual women.Journal of Homosexuality,62(7),971–992.
Meule,A,& Platte,P.(2015).Facetsofimpulsivity interactively predict body fat and binge eating in young women.Appetite,87,352–357.
Pearson,N.,&Biddle,S.J.H.(2011).Sedentary behavior and dietary intake in children,adolescents,and adults:A systematic review.AmericanJournalofPreventive Medicine,41(2),178–188.
Puhl,R.M.,&Schwartz,M.B.(2003).If you are good you can have a cookie:How memories of childhood food rules link to adult eating behaviors.Eating Behaviors,4(3), 283–293.
Racine,S.E.,Burt,S.A.,Iacono,W.G.,McGue,M.,& Klump,K.L.(2011).Dietary restraint moderates genetic risk for binge eating.Journal of Abnormal Psychology,120(1), 119–128.
Robinson,T.E.,&Berridge,K.C.(2008).The incentive sensitization theory of addiction:Some current issues.PhilosophicalTransactionsoftheRoyalSocietyB: Biological Sciences,363(1507),3137–3146.
Rodgers,R.F.,Paxton,S.J.,Massey,R.,Campbell,K.J., Wertheim,E.H.,Skouteris,H.,&Gibbons,K.(2013). Maternalfeeding practices predictweightgain and obesogenic eating behaviors in young children:A prospective study.International Journal of Behavioral Nutrition and Physical Activity,10(1),24.
Schäfer,A.,Vaitl,D.,&Schienle,A.(2010).Regional grey mattervolumeabnormalitiesin bulimianervosaand binge-eating disorder.Neuroimage,50(2),639–643.
Schag,K.,Schönleber,J.,Teufel,M.,Zipfel,S.,&Giel,K.E. (2013).Food-related impulsivity in obesity and binge eating disorder–a systematic review.Obesity Reviews, 14(6),477–495.
Schag,K.,Teufel,M.,Junne,F.,Preissl,H.,Hautzinger,M., Zipfel,S.,&Giel,K.E.(2013).Impulsivity in binge eating disorder:Food cues elicitincreased reward responses and disinhibition.PloS One,8(10),e76542.
Schienle,A.,Schäfer,A.,Hermann,A.,&Vaitl,D.(2009). Binge-eating disorder:Reward sensitivity and brain activation to images of food.Biological Psychiatry,65(8), 654–661.
Schmitz,F.,Naumann,E.,Trentowska,M.,&Svaldi,J. (2014).Attentional bias for food cues in binge eating disorder.Appetite,80,70–80.
Schulz,S.,Laessle,R.,& Hellhammer,D.(2011).No evidence of increased cortisol stress response in obese women with binge eating disorder.Eating and Weight Disorders-StudiesonAnorexia,BulimiaandObesity, 16(3),209–211.
Sherry,S.B.,&Hall,P.A.(2009).The perfectionism model of binge eating:Tests of an integrative model.Journal of Personality and Social Psychology,96(3),690–709.
Sherry,S.B.,Sabourin,B.C.,Hall,P.A.,Hewitt,P.L.,Flett, G.L.,&Gralnick,T.M.(2014).The perfectionism model of binge eating:Testing unique contributions,mediating mechanisms,and cross-cultural similarities using a daily diarymethodology.Psychologyof AddictiveBehaviors, 28(4),1230–1239.
Skinner,H.H.,Haines,J,Austin,S.B.,&Field,A.E. (2012).A prospective study of overeating,binge eating, and depressive symptoms among adolescent and young adultwomen.JournalofAdolescentHealth,50(5), 478–483.
Smith,D.G.,&Robbins,T.W.(2013).The neurobiological underpinnings of obesity and binge eating:A rationale for adopting the food addiction model.Biological Psychiatry, 73(9),804–810.
Sonneville,K.R.,Calzo,J.P.,Horton,N.J.,Haines,J., Austin,S.B.,&Field,A.E.(2012).Body satisfaction, weight gain and binge eating among overweight adolescent girls.International Journal of Obesity,36(7), 944–949.
Svaldi,J.,&Naumann,E.(2014).Effects of rumination and acceptance on body dissatisfaction in binge eating disorder.European Eating Disorders Review,22(5),338–345.
Tachi,T.,Murakami,K.,Murotsu,K.,&Washizuka,T. (2001).Affective states associated with bingeing and purging behaviours in Japanese patients with bulimia nervosa.British Iournal of Medical Psychology,74(4), 487–496.
Vella-Zarb,R.A.,Mills,J.S.,Westra,H.A.,Carter,J.C.,& Keating,L.(2015).A randomized controlled trial of motivational interviewing + self-help versus psychoeducation+self-help for binge eating.International Journal of Eating Disorders,48(3),328–332.
Voon,V.,Irvine,M.A.,Derbyshire,K.,Worbe,Y.,Lange,I., Abbott,S.,...Harrison,N.A.(2014).Measuring“waiting”impulsivity in substance addictionsand binge eating disorder in a novel analogue of rodent serial reaction time task.Biological Psychiatry,75(2),148–155.
Wilfley,D.E.,Agras,W.S.,Telch,C.F.,Rossiter,E.M., Schneider,J.A.,Cole,A.G.,...Raeburn,S.D.(1993). Group cognitive-behavioral therapy and group interpersonal psychotherapy for the nonpurging bulimic individual: A controlled comparison.Journalof Consulting and Clinical Psychology,61(2),296–305.
Wilfley,D.E.,Welch,R.R.,Stein,R.I.,Spurrell,E.B., Cohen,L.R.,Saelens,B.E.,...Matt,G.E.(2002).A randomized comparison ofgroup cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge-eating disorder.Archives of General Psychiatry,59(8),713–721.
Wilson,G T.,Wilfley,D.E.,Agras,W.S.,&Bryson,S.W. (2010).Psychological treatments of binge eating disorder.Archives of General Psychiatry,67(1),94–101.
Wolff,G.E.,Crosby,R.D.,Roberts,J.A.,&Wittrock,D.A. (2000).Differences in daily stress,mood,coping,and eating behavior in binge eating and nonbinge eating college women.Addictive Behaviors,25(2),205–216.
Woods,A.M.,Racine,S.E.,&Klump,K.L.(2010). Examining the relationship between dietary restraint and binge eating:Differential effects of major and minor stressors.Eating Behaviors,11(4),276–280.
Wu,M.D.,Giel,K.E.,Skunde,M.,Schag,K.,Rudofsky,G., de Zwaan,M.,...Friederich,H.-C.(2013).Inhibitory control and decision making under risk in bulimia nervosa and binge-eating disorder.International Journal of Eating Disorders,46(7),721–728.
Zendegui,E.A.,West,J.A.,&Zandberg,L.J.(2014).Binge eating frequency and regular eating adherence:The role of eating pattern in cognitive behavioral guided self-help.Eating Behaviors,15(2),241–243.
Zhu,H.,Luo,X.W.,Cai,T.S.,He,J.B.,Lu,Y.,&Wu,S.Y. (2015).Life eventstress and binge eating among adolescents:The roles of early maladaptive schemas and impulsivity.Stress and Health,In press.
猜你喜欢
心理学报(2021年1期)2021-01-29
初中生学习指导·中考版(2020年2期)2020-09-10
劳动保护(2019年7期)2019-08-27
保健与生活(2018年9期)2018-01-26
中国医药指南(2017年3期)2017-11-13
中国新闻周刊(2017年21期)2017-06-15
中国临床护理(2017年5期)2017-01-12
大众健康(2015年6期)2015-06-16
中学科技(2015年1期)2015-04-28
意林(2013年3期)2013-05-14