
带线锚钉弹性内固定与锁骨钩钢板内固定治疗肩锁关节脱位的Meta分析
2017-11-06 10:29李广峰曹烈虎王思成尹志峰曹中华李全苏佳灿
中华肩肘外科电子杂志 2017年3期
李广峰 曹烈虎 王思成 尹志峰 曹中华 李全 苏佳灿
带线锚钉弹性内固定与锁骨钩钢板内固定治疗肩锁关节脱位的Meta分析
李广峰1曹烈虎2王思成1尹志峰1曹中华1李全2苏佳灿2
目的通过Meta分析方法分析带线锚钉弹性内固定与锁骨钩钢板内固定方式治疗肩锁关节脱位的疗效及并发症并进行比较。方法计算机检索Cochrane Library、PubMed、Medline、Embase、CNKI、VIP等数据库; 手工检索中文知名骨科杂志的相关文献。查阅锚钉内固定与锁骨钩钢板内固定治疗肩锁关节脱位的对照研究。提取各研究中观测指标数据,运用Revman 5.3软件对其进行分析和处理。结果经筛选后最终纳入10篇文献,共纳入患者602例。Meta分析结果显示,两种方式在疗效、优良率、肩关节疼痛、肩关节活动受限、内固定物失效、再脱位等术后并发症方面的差异均有统计学意义(P <0.05)。结论 锚钉弹性内固定治疗肩锁关节脱位的疗效和优良率均优于锁骨钩钢板内固定方式。带线锚钉弹性内固定产生肩关节疼痛、活动受限、内固定物失效、再脱位等并发症方面少于锁骨钩钢板内固定方式。
锚钉; 锁骨钩钢板; 肩锁关节脱位; Meta分析
肩锁关节脱位为肩部常见损伤之一,多由肩部遭受直接暴力引起,约占全身骨折脱位的6%,占肩部受损的12%[1]。肩锁关节脱位患者常伴有肩锁韧带和喙锁韧带的完全或不完全断裂。其致伤原因主要以摔伤为主,国内患者以非机动车摔倒者多见,发达国家患者以年轻体育运动者多见[2]。关于肩锁关节脱位的分型,临床上方法众多,其中Tossy分类和Rockwood分类法应用较为常见[3]。Tossy I、II肩锁关节损伤可行保守治疗,疗效一般满意。Tossy Ⅲ型肩锁关节脱位患者肩锁关节完全脱位,伴有肩锁韧带、喙锁韧带完全断裂,关节稳定结构遭到完全破坏[4],保守治疗疗效差,需行手术治疗[5]。对于Tossy Ⅲ型肩锁关节脱位临床医师比较认同内固定治疗方式[6]。能否重建肩锁关节正常解剖、恢复肩锁关节功能直接决定了肩锁关节脱位治疗的成败。在达到该目的的同时尽量减少手术并发症,减少继发创伤性关节炎的发生[7-8],是临床医师不断追求的目标。
肩锁关节脱位的术后远期疗效很大程度上取决于内固定方式的选择。临床上治疗肩锁关节脱位的内固定方式较多,包括克氏针张力带固定、锁骨钩钢板内固定、锚钉内固定、纽扣钢板内固定等。国内外研究者对克氏针张力带固定、锁骨钩钢板内固定方式作了大量报道。近期,锚定重建肩锁韧带、喙锁韧带进行弹性固定治疗肩锁关节脱位逐渐增多,但缺乏多中心随机对照研究,以致许多研究者观点不一致。本研究筛选出一些符合纳入标准的文献后,通过Meta分析对锁骨钩钢板及锚钉弹性内固定治疗肩锁关节脱位的疗效和并发症作出评价,比较锁骨钩钢板及锚钉固定的疗效差异,为临床合理治疗提供一定依据。
资料与方法
一、文献纳入标准与排除标准
1.纳入标准:(1)研究对象:确诊为单纯肩锁关节脱位患者,分型为Tossy Ⅲ型或RockwoodⅢ型以上,需手术干预患者。不合并锁骨骨折、喙突骨折、神经血管损伤等,不分年龄、性别、种族。(2)研究类型:能反映锁骨钩钢板及锚钉治疗肩锁关节脱位的对照研究,如观察性研究、病例分析、随机对照试验。(3)国内外公开发表的锁骨钩钢板及锚钉治疗该疾病的病例对照研究文献,可计算出OR或RR值。(4)内固定方式:单组内固定方式为单一内固定,多组患者其中两组各单一采用锁骨钩或锚钉内固定。(5)报告指标:至少包括疗效评价结果、关节功能恢复、内固定失效、再脱位等术后并发症。
2.排除标准:(1)无法获得原始数据的文献。(2)非临床结果、术前术后测量结果不完整及动物实验文献、尸体力学实验。(3)重复文献。(4)研究类型:综述、评论、讲座、读者回信。(5)报告指标:不包括疗效评价结果及相关术后并发症。
二、干预措施
实验组采用锁骨钩钢板内固定方式治疗该疾病; 对照组采用锚钉弹性内固定方式治疗。
三、测量指标
(1)疗效。(2)并发症:肩部疼痛、肩关节活动度、内固定失效、再脱位、感染等。
四、检索策略
检索公开发表的关于锁骨钩钢板及克氏针张力带治疗该疾病疗效方面的中英文文献,使用计算机检 索 Cochrane Library、PubMed、Medline、Embase、CNKI、VIP等中英文数据库;手工检索《中国骨与关节损伤》、《中华骨科杂志》、《中华创伤骨科杂志》、《中国矫形外科》、《临床骨科》等国内影响力较高的杂志,检索中英文。检索英文数据库使用MeSH及自由词进行检索:MeSH用acromioclavicular joint dislocation检索,自由词用acromioclavicular joint dislocation/acromioclavicular luxation/acromioclavicular dislocation, rivet/anchor, clavicular/hook-plate/clavicular hook plate等进行搜索。中文以主题词搜索:肩锁关节脱位/肩锁关节损伤、锁骨钩钢板、锚钉/铆钉、对照研究。
五、文献筛选和质量评价
由2位研究者独立对纳入文献的题目、摘要进行筛选,提取记录数据,如果意见未能达成一致,最终由第3位研究者仲裁解决或经讨论后达成共识。质量评价按照Juni等随机对照试验的质量评价标准进行分析评价:(1)评价研究的随机方法是否正确,并分析研究的基线相似性,以辅助评价选择性偏倚;(2)是否进行了分配隐藏,方法是否正确;(3)是否采用盲法;(4)有无失访、退出、丢失。如果以上4条质量评价标准均满足且方法学正确,则该研究存在偏倚的可能性最小,评为A级;如果其中任一条或多条质量评价标准仅为部分满足(方法不清者),则该研究存在相应偏倚的中度可能性,评为B级;如果其中任一条或多条质量评价标准完全不满足(方法错误或未使用),则该研究存在相应偏倚的高度可能性,评为C级。
六、统计学分析
采用Cochrane协作网提供的RevMan 5.3统计软件进行分析,对具有临床同质性的资料进行Meta分析。当异质性过大或无法解释异质性来源时,则采用描述性分析。异质性检验采用卡方检验和I2检验两种统计学方法,若结果分别为P <0.01以及I2>50%被认为各研究间存在异质性,则进行亚组分析,以减小异质性,若仍存在异质性,采用随机效应模型;若结果分别为P>0.01以及I2<50%被认为各研究间异质性较小从而使用固定效应模型。用森林图评估经多元校正后的相对风险度,应用相应的95%置信区间解释不同研究间的直接证据和随之而来的整体效应。通过漏斗图检验有无发表偏倚。
结 果
一、纳入研究的基本特征和质量评价
最终纳入10篇(表1)相关研究进行Meta分析,均为随机对照试验、对照研究、病例分析,共纳入患者602例。其中锁骨钩钢板组有296例患者,锚钉组有306例患者,2篇为3种方式内固定两两比较,8篇为两种内固定治疗方式的比较。根据质量评价标准,10篇文章,其中1篇为A级,6篇为B级,3篇为C级。8个研究比较了两种手术方式的疗效(优良率),通过异质性检验,异质性较大(P=0.14,I2=49%),通过敏感性分析,剔除不适合的1篇文献,再行异质性分析。10篇文章描述了术后并发症,同样进行异质性分析,发现异质性较大(P=0.06,I2=46%),通过敏感性分析,剔除1篇文献。

表1 纳入研究的10篇文献的基本情况
二、两种手术方式疗效的系统性评价
共8篇文献纳入该研究,样本量共计425例,其中锁骨钩钢板组207 例,锚钉组218 例,各研究间无明显统计学异质性(P=0.29,I2=18%)。故采用固定效应模型进行Meta分析,结果显示,RR=1.10,95%CI:1.03~1.17,P=0.004,提示两种手术方式的优良率差异有统计学意义,说明锚钉固定组在疗效方面较锁骨钩钢板组疗效为好(图1)。通过漏斗图评价文章发表偏倚,通过图2可以看出所有文献均在斜线范围内,而且在中线两边分配疾病均匀,说明各研究间异质性较低,可进行合并分析,发表偏倚低风险较低。

图2 两种方案固定后优良率漏斗图
三、术后并发症的Meta分析
9个研究对两种手术方式发生术后并发症情况作出了比较,根据统计学分析,有1篇文献数据无可比性,纳入8篇文献,样本量共计492例。其中锁骨钩钢板组有248例患者,锚钉组有244例患者,研究具有统计学异质性故采用固定效应模型进行Meta分析,RR=0.19,95% CI:0.11~0.34,P <0.00001, 提示两种手术方式在术后并发症方面差异有统计学意义,说明锚钉固定组在术后并发症的发生情况要少于锁骨钩钢板组(图3)。通过漏斗图评价文章发表偏倚,通过图4可以看出所有文献均在斜线范围内,而且在中线两边分配疾病均匀,说明各研究间异质性较低,可进行合并分析,发表偏倚低风险较低。
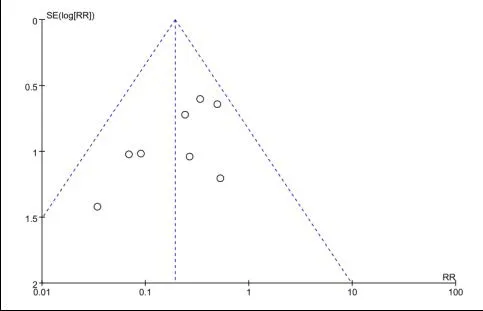
图4 两种内固定术后并发症漏斗图
讨 论
肩锁关节属于微动关节,在肩关节各个方向的运动中起到不可或缺的作用。肩锁关节骨性结构由锁骨肩峰端、肩胛骨、肩峰关节面构成,软组织构成主要有喙锁韧带、肩锁关节囊、肩锁韧带、肩关节周围三角肌、斜方肌的腱性附着部分等[9]。喙锁韧带对维持肩锁韧带的稳定性至关重要,肩锁关节脱位时常伴有喙锁韧带、肩锁韧带断裂,手术治疗须对喙锁韧带进行修复。
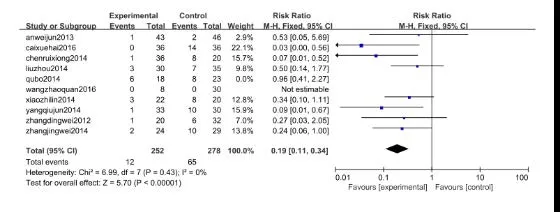
图3 两种内固定术后并发症森林图
锁骨钩钛质钢板是AO/ASIF组织依据肩锁关节的解剖结构及其微动特点设计的一种内固定材料,刚度相对较大,具有组织相容性好,手术操作简单、使用方便、创口小、术后并发症发生率低等优点,符合锁骨S 状解剖外形,对于钢板和锁骨形状差异较大的患者可适当预弯取得与骨面的良好的贴附。其钩部可钩在肩峰的下后,利用钢板翘拨力量恢复肩关节正常解剖结构,为肩锁关节周围软组织及韧带的愈合提供稳定无张力的环境,但锁骨钩钢板置入后,术后活动时引起肩峰撞击致疼痛,肩锁关节为微动关节,虽然锁骨钩钢板的钩端在肩峰下方是游离的,可在肩峰孔中滑动,使肩锁关节保持了一定微动,但其作用有限,且长时间反复与关节摩擦,易产生肩峰下撞击综合征,引起疼痛症状。文献报道,发生率高达22.2%[10]。由于锁骨钩对肩袖的卡压造成肩关节外展上举活动受限,锁骨钩钢板需二次手术取出内固定物, 在一定程度上增加了患者的痛苦及医疗费用。
有学者报道[11]采用带线锚钉治疗肩锁关节脱位取得满意效果,其优点为:手术创伤小,重建喙锁韧带通过对抗肩锁关节的分离应力而起到张力带的作用,弹性固定更符合生物力学,对恢复肩锁关节的稳定,促进喙锁韧带在一定张力刺激下愈合具有重要作用。锚钉体积小,组织相容性好,无需二次手术取出[12]。缝线不产生切割应力,不破坏肩锁关节面,进行弹性固定时,属于动态固定,符合肩锁关节这一微动关节的生理功能,最大程度保持肩关节功能。锚钉使用符合肩锁关节生物力学要求。上臂外展时,锚钉线固定不妨碍关节上下、前后及旋转移位带来的微动。且不会造成肩峰与肱骨头间隙变小,从而可使患者早期进行各个角度功能锻炼,预防肩关节周围韧带粘连及肌肉萎缩。而且在肩锁关节分离间隙较小,肩锁韧带未完全断裂情况下,不需要修复喙锁韧带时,可应用小切口微创植入喙突[13]。对于带线锚钉把持力和提供的张力的大小是否合适,有报道[14]指出锚钉对维持关节的稳定性、弹性性能和模量、轴向刚度均优于正常喙锁韧带。但对于老年女性患者,尤其伴有严重骨质疏松患者,锚钉把持力可能较正常成年人减低,如需加强锚钉力量或修复韧带张力,术中可在喙突及锁骨钻孔,双线合并,增加张力,重建喙锁韧带,避免因锚钉拔出致使肩锁关节再次脱位的可能。
本系统评价所纳入的研究样本量较大,所纳入文献的整体质量水平较高,从Meta分析的结果来看采用锚钉内固定方式治疗肩锁关节脱位的疗效和优良率与锁骨钩钢板内固定治疗方式比较,优于锁骨钩钢板治疗。术后产生肩关节疼痛、肩关节活动受限、内固定物失效、再脱位等并发症的情况均比采用锁骨钩钢板内固定治疗方式要少。
因此,与锁骨钩钢板内固定方式相比,锚钉弹性内固定治疗肩锁关节脱位的疗效和优良率较高,术后并发症较低,由于各个研究报道的并发症不统一,该研究未进行进一步对并发症种类的探讨及分析。综合考虑,采用锚钉治疗该疾病要优于钢板内固定治疗方式,并且其具有切口小、操作简单、弹性固定利于韧带重建、术后并发症发生率低、无需二次手术取出等优点。
各医疗单位或者医师可根据具体情况选择,在两种内固定方式均可实施情况下,建议首先考虑锚钉内固定方式。因此,锚钉弹性固定修复肩锁关节脱位是一种安全有效的手术方式,值得在临床广泛推广应用。
虽然本系统评价通过检索国内外数据库,同时也存在局限性,例如受语种限制,仅检索了中、英文文献,会忽视其他语言的优质研究,从而导致检索不全面,造成结果偏倚。同时,纳入文献的方法学也可能存在不同程度的局限性,如随机化方法偏倚、测量偏倚、实施偏倚、选择偏倚、发表偏倚等。因此,本研究结果需要收集更多样本量,开展多中心、高质量的随机对照试验进一步验证。
[1]盛敏, 林斌. 肩锁关节脱位治疗现状及进展[J]. 解剖与临床 , 2007, 12(1) : 68-70.
[2]Kaplan LD, Flanigan DC, Norwig J, et al. Prevalence and variances of shoulder injuries in elite collegiate football players[J]. Am J Sports Med, 2005, 33(8): 1142-1146.
[3]许树柴, 袁凯, 林定坤, 等.肩锁关节脱位治疗进展[J].中国矫形外科杂志, 2010, 18(14): 1180-1183.
[4]侯春林, 王诗波, 吴韬.锁骨外科学[M].北京:人民军医出版社, 2004: 97-98.
[5]Spencer EE Jr. Treatment of grade Ⅲ acromioclavicular joint injuries:a systematic review[J]. Clin Orthop Relat Res,2007, 455(1):38-44.
[6]Bradley JP, Elkousy H. Decision making: operative versus nonoperat ive treatment of acromioclavicular joint in juries[J].Clin Sports Med, 2003, 22(2):277-290.
[7]卢向东.自制弹性肩肘带治疗肩锁关节脱位[J].中医正骨,2005, 17(6):55.
[8]刘远峰.弹力肩肘带加置沙袋治疗重度肩锁关节脱位[J].中医正骨, 2004, 16(3):51.
[9]李欣, 何爱咏. 锁骨钩钢板与克氏针张力带治疗肩锁关节脱位和锁骨远端骨折疗效比较[J].中国矫形外科杂志,2006, 14(24):1855-1857, 1932.
[10]陈新, 王佳, 闫旭, 等. 钩钢板治疗肩锁关节脱位术后肩峰下撞击综合征与第二肩关节间隙的关系[J]. 中华骨科杂志,2010, 30(7):654-657.
[11]杨顺, 姜春岩, 向明, 等. 金属缝合锚治疗肩锁关节脱位 20例[J]. 中国组织工程研究与临床康复, 2011, 15(17):3212-3216.
[12]罗吉伟, 余斌, 魏宽海, 等. 自体掌长肌移植重建喙锁韧带结合带线锚钉固定治疗肩锁关节脱位的疗效[J/CD]. 中华肩肘外科电子杂志, 2014, 2(1):25-29.
[13]胡晓川, 林辉阳, 向明, 等. 锁定钢板结合缝合锚固定治疗NeerⅡB型锁骨远端骨折[J/CD], 中华肩肘外科电子杂志,2015, 3(4):199-205.
[14]王勤业, 罗亚平, 张德堂, 等. 缝合锚技术治疗肩锁关节脱位的功能生物力学研究[J]. 中国骨与关节损伤杂志,2009, 24(4):389-392.
Su Jiacan, Email:drsujiacan@163.com
Curative effect comparison analysis of fixation with suture anchor and hook plate for acromioclavicular joint dislocation
Li Guangfeng1,Cao Liehu2, Wang Sicheng1, Yin Zhifeng1, Cao Zhonghua1, Li Quan2,Su Jiacan2.1Department of Orthopaedics ,Shanghai Zhongye Hospital, Shanghai 200941,China;2Deparpment of Orthopaedic Trauma,Changhai Hospital of Second Military Medical University,Shanghai 200433,China
BackgroundAcromioclavicular joint dislocation is one of the common shoulder injuries, mostly caused by direct violence on shoulder. It accounts for about 6% of whole-body fractures and dislocations, and 12% of shoulder injuries. Acromioclavicular dislocation is often accompanied with complete or incomplete rupture of the acromioclavicular ligament and coracoclavicular ligament.This injury is mainly caused by falling. In China, falling from non-motor vehicles is the most common cause of this injury, while in developed countries, this injury is most common in young athletes.Clinically, there are many classifications of acromioclavicular joint dislocation, of which Tossy classification and Rockwood classification are most commonly applied. Tossy type I and type II injury can be treated conservatively and the effect is generally satisfactory. Tossy type III means the complete dislocation of the acromioclavicular joint, accompanied with the complete rupture of acromioclavicular ligament and coracoclavicular ligament and the complete destruction of the stability of joint structure.Surgical treatment is necessary because the conservative treatment is of poor efficacy. Internal fixation treatment is a clinically accepted treatment for Tossy type III dislocation. Whether we can restore the normal anatomy and the function of the acromioclavicular joint directly determines the success or failure of an acromioclavicular joint dislocation treatment. It is always our goal to achieve this purpose while minimizing surgical complications and reducing the occurrence of secondary traumatic arthritis.The long-term postoperative efficacy of acromioclavicular dislocation is largely dependent on the choice of internal fixation. There are many ways of treating acromioclavicular joint dislocation clinically by internal fixation, including Kirschner wire, tension band, clavicle hook plate, suture anchor, button plate and so on. Domestic and foreign researchers have made a lot of reports on Kirschner wire, tension band and hook plate. Recently, reconstruction of acromioclavicular ligament and coracoclavicular ligament by elastic fixation using suture anchor have gradually increased.However, many researchers hold different opinions because of the lack of multi-center randomized controlled trials. In this study, we selected some papers that met the inclusion criteria, evaluated the effect and complication of hook plate and anchored elastic internal fixation for acromioclavicular joint dislocation by meta-analysis. We also compared the difference of treatment effect between clavicular hook plate and suture anchor fixation, providing a basis for rational clinical treatment.Methods(1)The inclusion and exclusion criteria of literature.Inclusion criteria: ①Object: patients diagnosed of acromioclavicular joint dislocation alone, classified as TossyⅢ or RockwoodⅢ or more, surgery intervention needed.②Type of study: control studies which can reflect the treatment of acromioclavicular joint dislocation using the hook plate and suture anchors, such as observational studies, randomized controlled trials and case reports.③Domestic and foreign published papers reporting of randomized controlled trials treated with hook plates and suture anchors, of which OR or RR value can be calculated.④internal fixation: a single group adopt single way of internal fixation; for two groups, each group adopts either way of fixation. ⑤Report indicators: including at least the results of the evaluation of efficacy, joint function recovery and post-complications such as internal fixation failure and re-dislocation.Exclusion criteria: ① literatures unable to obtain the original data; ② non-clinical results, incomplete preoperative and postoperative measurement results, animal experiments and cadaver mechanics experiments; ③ repeated literature;④ type of study: type of research for the review,comments, lectures, readers reply; ⑤ report indicators: not including the results of evaluation and related postoperative complications.(2)Interventions.The study group uses the hook plate to treat this injury, while the controlled group uses the elastic internal fixation.(3)Index of measurement.①Efficacy; ②Complications: shoulder pain, ROM, internal fixation failure, re-dislocation, infection and so on.(4)Searching strategy.We search the Chinese and English literatures discussing the treating efficacy of the clavicular hook plate and the Kirschner wire tension band. We search the Cochrane Library, Pubmed, Medline, Embase, CNKI, VIP and other Chinese and English databases by computer, and "Chinese Orthopedic Surgery", "Clinical Orthopedics”, "Chinese Journal of Orthopedics and Traumatology " and other domestic influential magazines by hand, both in Chinese and English. Search the English databases using MeSH and free words for retrieve: MeSH searched with “acromioclavicular joint dislocation” We use free words like acromioclavicular joint dislocation/acromioclavicular luxation/acromioclavicular dislocation, rivet/anchor, clavicular/hook-plate/clavicular hook plate, etc. Search keywords in Chinese "acromioclavicular dislocation, acromioclavicular joint injury, clavicular hook plate, anchoring/rivet, controlled study".(5)Literature screening and quality evaluation.Two researchers screened the titles and abstracts of the included literature by, and then extracted the recorded data. If they failed to reach an agreement, the final decision was made by the third author or by discussion to reach a consensus. Quality evaluation was based on the standard evaluation on RCT performed by Juni et al. ① evaluate whether the randomized method is correct and analyze the baseline similarity of the study to assist the evaluation of the selective bias; ②whether the distribution is hidden and whether the method is correct; ③ the use of blindness; ④ whether missed,quit, lost. If all four quality evaluation criteria are met and the methodology is correct, the probability of bias in the study is minimal, which ranked as Grade A; if one or more of the criteria is only partially satisfied (the method is unclear), then the study has a medium possibility of bias, which is rated as Grade B. If one or more of the quality evaluation criteria is completely unsatisfied (the method is incorrect or unused), the study has a high possibility of the corresponding bias, which we rate as Grade C.(6)Statistical analysis.Statistical analysis was performed by RevMan 5.3 statistical software, provided by the Cochrane Collaboration Network. to make a meta-analysis of clinical homogeneity data. Descriptive analysis is used when the heterogeneity is too large or the heterogeneity source cannot be explained. Heterogeneity test has two methods: chi-square test and I2test. If P <0.01 and I2>50% we consider there is heterogeneity between the various studies, and then a sub-group analysis was performed to reduce heterogeneity. If it still existed, random effect model was introduced; if P >0.01 and I2<50%, we think there is little heterogeneity between the studies and then we can use the fixed effect model. Using the forest map to assess the relative risk after multiple corrections, we apply the corresponding 95% confidence interval to explain the direct evidence between the different studies and the consequent overall effect. We use a funnel chart to check whether there is a publication bias.ResultsThe basic characteristics and quality evaluation of the included literatures: 10 meta-analyzes were included in the study finally. All of them were randomized controlled trials, controlled studies and case analysis. 602 patients were included totally.There were 296 patients in clavicular hook plate group, 306 patients in anchor group, 2 papers of the comparison between 3 ways of internal fixation, and 8 papers of the comparison between 2 ways of internal fixation. According to the quality evaluation criteria, among the 10 articles, 1 is for the Grade A, 6 are for the Grade B, 3 are for the Grade C. Eight studies compared the efficacy (excellent rate) of the two surgeries, the heterogeneity was largely through heterogeneity tests (P=0.14, I2=49%). We excluded a study after sensitivity analysis and then performed the heterogeneity analysis. Appling the same heterogeneity analysis on the 10 articles described postoperative complications, the heterogeneity was found large (P=0.06, I2=46%). Therefore, we remove a literature through the sensitivity analysis.A systematic review of the efficacy of the two surgeries: 7 articles were included in the study. Totally 425 cases were included in the study. There were 207 cases of clavicular hook plate group and 218 cases of suture anchor group. There was no statistically significance between different groups (P=0.29,I2=18%). Therefore, Meta-analysis was performed using fixed effect model, RR=1.10, 95% CI: 1.03-1.17, P=0.004, suggesting that the difference between the two surgical methods was statistically significant and indicating that the anchor group has a better curative effect over the hook plate group.All the literatures were in the range of slash, and the disease was distributed evenly on both sides of the middle line, indicating that the heterogeneity of each study was low, which could be combined and analyzed and the publication bias was low. Meta-analysis of postoperative complications: 9 studies compared the postoperative complications of the two surgical methods. According to statistical analysis,there is one literature of which data is not comparable, so eight literatures were included. The total sample size is 492. There were 248 patients in the clavicular hook plate group and 244 patients in the suture anchor group. The meta-analysis was performed in fixed model because of the statistical heterogeneity. RR=0.19, 95% CI: 0.11-0.34, P <0.00001, suggesting that there was statistically significance between the two surgical methods in the postoperative complications and indicating the postoperative complications of the anchoring group are less than hook plate group. We evaluated all of the literatures by funnel chart. All of the literatures were in the range of slash and the disease was distributed evenly on both sides of the middle line, indicating that the heterogeneity of each study was low, which could be combined and analyzed and the publication bias was low. Conclusions Compared with hook plates, elastic internal fixation using suture anchors has a better efficacy and excellence rate and lower rate of post-op complications when treating AC dislocation. As the complications are different according to different research, this study didn't further discuss and analyze the types of complications. Generally, suture anchors are better than the hook plates, since it has many advantages such as smaller incision, easy manipulation, elastic internal fixation which is good for tendon reconstruction, (less) post-op complications, no need for a second-time surgery and so on. Different hospitals and doctors can make decisions according to their own conditions. We give priority to suture anchors when both ways of fixation are applicable.
Acromioclavicular separation; Anchor; Clavicular hook plate; Meta-analysis
10.3877/cma.j.issn.2095-5790.2017.03.008
国家自然国际合作基金(8141101156);上海市科委生物医药专项(154119500600)
200941 上海中冶医院骨科1;200433 上海,第二军医大学附属长海医院创伤骨科2
苏佳灿,Email:drsujiacan@163.com
2016-10-13)
(本文编辑:李静;英文编辑:陈建海、张晓萌、张立佳)
李广峰,曹烈虎,王思成,等. 带线锚钉弹性内固定与锁骨钩钢板内固定治疗肩锁关节脱位的Meta分析[J/CD].中华肩肘外科电子杂志,2017,5(3):199-206.
猜你喜欢
创伤外科杂志(2022年1期)2022-01-27
中华肩肘外科电子杂志(2020年1期)2020-08-24
中华肩肘外科电子杂志(2020年1期)2020-08-24
学习与科普(2019年6期)2019-09-10
中华肩肘外科电子杂志(2019年4期)2019-08-24
中华肩肘外科电子杂志(2019年4期)2019-08-24
中华肩肘外科电子杂志(2019年4期)2019-08-24
意林(2018年6期)2018-04-03
爱你(2017年35期)2017-11-24
Coco薇(2017年5期)2017-06-05
