
Hepatitis C virus antigens enzyme immunoassay for one-step diagnosis of hepatitis C virus coinfection in human immunodeficiency virus infected individuals
2019-06-20 07:59KeQinHuWeiCuiSusanRousterKennethSherman
World Journal of Hepatology 2019年5期
Ke-Qin Hu, Wei Cui, Susan D Rouster, Kenneth E Sherman
Ke-Qin Hu, Wei Cui, Division of GI/Hepatology, University of California, Irvine, School of Medicine, Orange, CA 92868, United States
Susan D Rouster, Kenneth E Sherman, Division of Digestive Diseases, University of Cincinnati College of Medicine, Cincinnati, OH 45267, United States
Abstract
Key words:Hepatitis C virus; Hepatitis C virus antigens; Hepatitis C virus core antigen;Hepatitis C virus diagnostic test; Diagnostic assay; Enzyme immunoassay
INTRODUCTION
Chronic hepatitis C virus (HCV) infection affects approximately 115 million individuals worldwide that can progress to chronic hepatitis C or cirrhosis, and it is associated with development of hepatocellular carcinoma[1,2]. HCV infection is also common in human immunodeficiency virus (HIV)-infected individuals, as both infections share the same modes of transmission[3]. The activity and progression of liver injury are more severe in HCV and HIV coinfected individuals than those with HCV monoinfection[4]. Research advances have resulted in clinical application of direct acting anti-viral treatment for HCV infection. All these treatment regimens are highly safe and effective and associated with > 95% sustained virologic response rates even in those with HCV/HIV coinfection[5-8]. It is recommended that HIV and HCV coinfection should not be treated differently than HCV monoinfection[7,8]. Successful eradication of HCV has been shown to improve the prognosis of HCV-induced liver disease and reduce the associated mortality[9,10]. Both the World Health Organization and the United States of America Center for Disease Control have advocated eradicating HCV infection by 2030[11,12]. These emphasize the essential need for effective HCV screening and diagnosis, including HIV-infected individuals, to link them to appropriate care.
However, the current two-step HCV test process represents one of the main barriers for effective HCV screening[7,13,14], as it is suboptimal, costly, inconvenient,time consuming, and globally not widely available. Current anti-HCV tests, although highly specific and sensitive, cannot distinguish viremic HCV (V-HCV) infection from resolved HCV (R-HCV) infection[15]. Thus, when anti-HCV is tested positive, an expensive HCV reverse transcription-polymerase chain reaction (RT-PCR) is mandatory to further test the presence or absence of viremia. Additionally, anti-HCV testing cannot be used for diagnosing acute HCV infection and may cause false negative results in immunocompromised patients, those receiving immunosuppressive therapy, or on hemodialysis[16,17]. Although serum HCV RNA RT-PCR is a highly specific and sensitive test to detect V-HCV infection, the dependence on expensive equipment, high cost, and time-consuming nature limit its applicability,especially in developing countries and regions.
Several HCV core antigen (HCVcAg) assays have been reported[18-29]. The detectionlimit of the Ortho HCVcAg enzyme immunoassay (EIA) was reported to be 1.48 pg/mL, corresponding to HCV RNA of 9707 IU/mL. Hence, it is not a sensitive test.The detection threshold of the Abbott Architect HCVcAg assay is reported to be 3 fmol/L, equivalent to HCV-RNA between 1015-1045 IU/mL, which is in line with published data showing HCVcAg detection limits corresponding to serum HCV-RNA levels in the range of 428-2700 IU/mL[30-32]. However, the sensitivity of the Abbott Architect HCVcAg assay was only 64.7% to 81.9% when serum HCV RNA was < 4 log IU/mL and 0.0% to 19.7% when serum HCV RNA was < 3 log IU/mL[31,33].Furthermore, a high false positive rate occurred in patients with R-HCV infection (i.e.,negative HCV RNA and positive anti-HCV results) when tested with the current HCVcAg assay[32-34]. Currently available HCVcAg assays have limited clinical utility due to their low specificity and sensitivity. Recently, we developed a highly sensitive and specific HCV-Ags EIA that could be used for one-step diagnosis of V-HCV infection by testing serum or urine specimens[35].
The goals of the present study were to further assess the sensitivity and specificity of the HCV-Ags EIA and its value for one-step diagnosis of viremic HCV infection in HCV monoinfected and HCV/HIV coinfected individuals through a blinded way,i.e.obtaining serum samples from one lab (Kenneth E Sherman; KES) and performing HCV-Ags EIA in another lab (Ke-Qin Hu). Our results indicated that HCV-Ags EIA holds high specificity and sensitivity for detection of V-HCV infection in individuals with HCV monoinfection as well as HCV/HIV coinfection.
MATERIALS AND METHODS
HCV and HIV diagnosing criteria, serum specimen, and clinical data collection
Chronic V-HCV infection was defined as positive anti-HCV and HCV RNA tests for 6 mo. R-HCV (or past) infection was defined on the basis of a known history of prior HCV infection, a positive anti-HCV test, but negative HCV RNA RT-PCR performed at least twice. Chronic viremic HIV infection was diagnosed by positive tests for both anti-HIV and HIV RNA PCR. Whereas, non-viremic HIV infection was defined by history of HIV infection, on HIV treatment, and negative HIV RNA test.
The study was approved by Institutional Review Boards of both institutions. After obtaining informed consent, venous blood specimens were collected, and serum aliquots were prepared and stored at -80 °C. Quantitative HCV RNA RT-PCR and HIV RNA RT-PCR were performed on the same day in the clinical laboratory. The clinical records were also reviewed for details regarding clinical diagnosis and course.
Anti-HCV test was performed using the Architect Anti-HCV Assay, a chemiluminescent microparticle immunoassay (Abbott Laboratories, Abbott Park, IL,United States). Serum HCV RNA was quantitated using the Abbott Real Time HCV assay, which has a lower limit of quantification of 12 IU/mL (Abbott Laboratories,Abbott Park, IL, United States). Anti-HIV was performed using Abbott's Architect HIV Ag/Antibody Combo assay for the simultaneous detection of both HIV antigen and antibodies. HIV RNA test was performed by LabOne, Inc. using the Roche Diagnostics Amplicor HIV-1 Monitor test kit with a linear range of 400-750000 HIV-1 RNA copies/mL.
Serum specimens and study conduction
The present studies utilized a blind fashion to assess the performance of the HCV-Ags EIA that was recently reported highly sensitive and specific[35]in sera with (1) HCV mononfection and (2) HCV and HIV coinfection. For study enrollment, patients must have a full assessment for HCV and HIV infection as described above. Serum samples were collected from the KES lab, and divided into four groups without HCV and HIV infection, HCV monoinfection, and HCV and HIV coinfection with different HIV replication status as shown in Table 1.
All the serum specimens were blindly coded in the KES lab and sent to the Ke-Qin Hu lab to perform HCV-Ags EIA. The test results were then sent back to the KES lab for decoding and used for statistical analysis. The related clinical data, such as age,gender, and CD4 count, were collected in the KES lab.
HCV-Ags EIA
All coded serum samples underwent HCV-Ags EIA that was performed in the Ke-Qin Hu lab, as previously reported[35]. Briefly, 96 microtiter plates were coated with HCVAgs-specific capture antibodies followed by addition of HCV detection antibodies specific to HCV antigens (i.e., HCVcAg and non-structural S3-S5 proteins) and HRP-conjugated secondary antibodies. Finally, a color reaction was produced using substrate solution, and optical density was measured using ELX 800 UniversalMicroplate Reader. Results were expressed as optical density values.

Table 1 Blinded 147 serum samples in four groups for hepatitis C virus antigens enzyme immunoassay
Statistical analysis
The categorical data were presented as percentage, and continuous data were expressed as the mean and standard deviation. A 2 x 2 table was used to calculate the test sensitivity, specificity, positive, and negative predictive values. ThePvalues less than 0.05 were considered statistically significant. SPSS software was used for statistical analysis.
RESULTS
Study groups, serologic and virologic data, and CD4 count
As summarized in Table 1, a total of 147 coded serum specimens were used in the present study in the following four groups. Group 1 included 10 sera without HCV or HIV infection (i.e., negative anti-HCV, HCV RNA, anti-HIV, and HIV RNA tests);group 2 included 54 sera with HCV monoinfection (i.e., positive HCV RNA, negative anti-HIV tests); group 3 included 38 sera with viremic HCV and HIV coinfection (i.e.,positive for both HCV RNA and HIV RNA tests), and group 4 included 45 sera with viremic HCV infection, but non-viremic HIV infection (i.e., history of positive HCV RNA and anti-HIV, on HIV treatment, and currently negative HIV RNA tests).
In group 2, HCV genotype (GT) distribution was GT1 = 47, GT3 = 4, GT4 = 1, and GT mixed = 2, and the range of serum HCV RNA load was from 4.8 x 2 log to 2.6 x 7 log IU/mL. In group 3, HCV GT distribution was GT1 = 28 and GT4=10. The range of serum HCV RNA load was from 4.6 x 5 log to 7.8 x 7 log IU/mL. The range of serum HIV RNA load was from 4.7 x 1 log to 1.2 x 6 log copies/mL, and mean CD4 count was 482.3 (282-800). In group 4, HCV GT distribution was GT1 = 35, GT2 = 6, GT4 = 2,and ND = 2. The range of serum HCV RNA load was from 9.5 x 3 log to 2.1 x 7 log IU/mL. All were negative for HIV RNA, and mean CD4 count was 594 (174-1106).
Additionally, five sera with HCV monoinfection and HCV RNA load ranging from 50-59 IU/mL were tested by the HCV-Ags EIA.
Performance of HCV-Ags EIA in HCV monoinfection
As shown in Table 2, in ten sera without HCV and HIV infection, all (100%) tested negative for HCV-Ags EIA. All 54 (100%) sera with viremic HCV infection tested positive for HCV-Ags EIA regardless of serum HCV RNA level and GT. Thus, the test results of HCV-Ags EIA were in 100% accordance to HCV infection status by HCV RNA PCR. Statically, HCV-Ags EIA test was confirmed to have 100% sensitivity and specificity for HCV viremic infection. Additionally, in five sera with low viremic HCV infection (HCV RNA level ranged between 50-59 IU/mL), 4/5 were positive for HCVAgs EIA.
信号发生模块电路如图5所示,可由1个外部参考时钟、1个退耦电容电路、1个低精度数字电位器组成[6]。外部参考时钟采用的是25M的有源晶振;低精度电阻器采用的是MCP41010数字电位器[7],用来调节幅度的大小(因为AD9833产生正的弦波只有5V,采用数字电位器可以调节其幅度的大小,便于按键调节幅度的输出)。
Performance of HCV-Ags EIA in HCV/HIV coinfection
As shown in Table 3, in 38 sera with viremic HCV and HIV coinfection, all (100%)were positive for HCV-Ags EIA. In 45 sera with viremic HCV and non-viremic HIV coinfection, all (100%) were positive for HCV-Ags EIA. Thus, the test results of HCVAgs EIA were in 100% accordance to HCV infection status by HCV RNA PCR,regardless if HIV infection was active and of the CD4 count.
DISCUSSION
HCV infection affects approximately 115 million people globally[1]. Currently,diagnosis of HCV infection requires two sequential steps:testing anti-HCV to screen,followed by HCV RNA RT-PCR to confirm viremia[7,13,14]. The latest anti-HCV tests are highly sensitive and specific, but they cannot differentiate acute HCV infection with V-HCV and R-HCV infection. Therefore, all positive anti-HCV test results need to be further tested by HCV RNA RT-PCR. Although HCV RNA RT-PCR tests are highly sensitive and specific for V-HCV infection, it is time consuming, costly, and not available and affordable in many developing countries and regions.
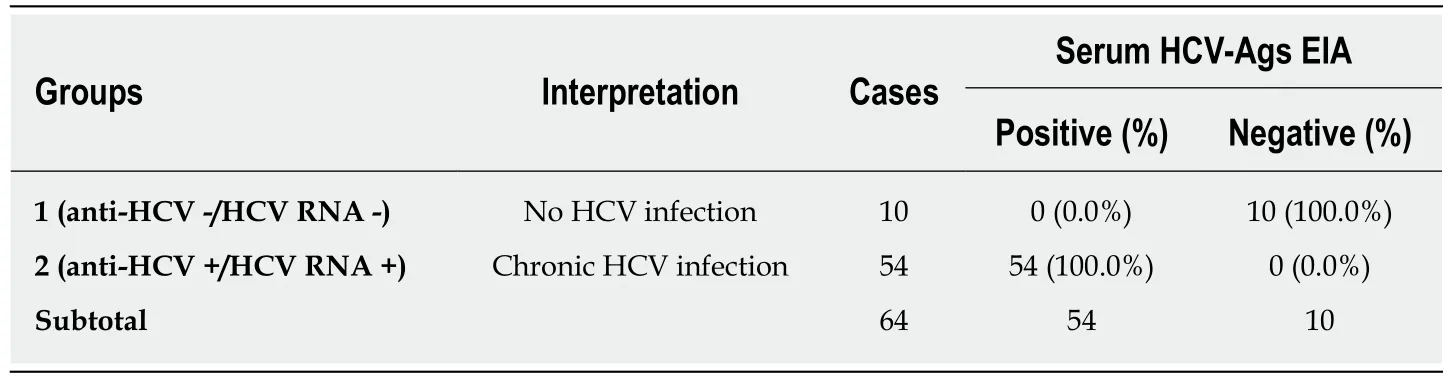
Table 2 The accordance of serum hepatitis C virus antigens enzyme immunoassay test results to hepatitis C virus RNA PCR in sera with hepatitis C virus monoinfection
Recently, we developed a novel HCV-Ags test that is more sensitive and specific than traditional HCVcAg tests and holds potential for one-step serologic diagnosis of V-HCV infection[35]. In the present study, we used a blinded fashion to further test the sensitivity and specificity of the HCV-Ags EIA in HCV sera with monoinfection and HCV/HIV coinfection. The serum samples were from one laboratory with coding,and HCV-Ags EIA were performed blindly in another laboratory, then decoded for data analysis.
In 64 sera, 10 without HCV and HIV infection and 54 with viremic HCV infection, it was in 100% accordance of HCV-Ags EIA test results to HCV infection status by HCV RNA PCR. This blinded study further confirmed our previous report that the HCVAgs EIA is highly specific and sensitive in diagnosing viremic HCV infection in those with HCV monoinfection. In an additional five sera with viremic HCV infection as low as HCV RNA load ranging between 50-59 IU/mL, 4/5 were positive for HCVAgs EIA, further confirming the lowest limits of detection of the HCV-Ags assay as previously reported[35].
We then tested utility of HCV-Ags EIA in sera with HCV and HIV coinfection. In 38 sera with viremic HCV and HIV coinfection and 45 sera with viremic HCV and nonviremic HIV coinfection, it was in 100% accordance of HCV-Ags EIA test results to HCV infection status by HCV RNA PCR, regardless if HIV infection was active and of the CD4 count. These results confirmed that the HCV-Ags EIA is highly specific and sensitive in diagnosing viremic HCV infection in those with HCV and HIV coinfection, no matter if HIV infection was active or not. The present study confirmed the potential that HCV-Ags EIA may provide an equal and cost-effective way for onestep screening and diagnosing viremic HCV infection. As HCV infection is common in HIV-infected individuals, these results are very promising in further study on the clinical application of the HCV-Ags EIA in the population with risk for both HCV and HIV infection, an important addition to the World Health Organization and the Center for Disease Control’s commitment of HCV elimination globally[11,12].
It should be noted that the main advantage of the present study is the blinded fashion, but the sample size was small. Further larger, prospective studies are needed to assess the value of clinical application of the HCV-Ags EIA.

Table 3 Accordance of serum hepatitis C virus antigens enzyme immunoassay to hepatitis C virus PCR testing results in sera with hepatitis C virus/human immunodeficiency virus coinfection
ARTICLE HIGHLIGHTS
Research background
Current diagnosis of hepatitis C virus (HCV) infection requires two sequential steps:testing for anti-HCV followed by HCV RNA PCR to confirm viremic infection. We have developed a highly sensitive and specific HCV-antigens (Ags) enzyme immunoassay (EIA) for one-step diagnosis of viremic HCV infection. However, it has not been tested blindly and especially in those with HCV and human immunodeficiency virus (HIV) coinfection.
Research motivation
Although HCV RNA RT-PCR tests are highly sensitive and specific for viremic HCV infection, it is time consuming, costly, and not available and affordable in many developing countries and regions. Further confirming the sensitivity and specificity of HCV-Ags EIA will provide additional support of its clinical value for one-step screening and diagnosing HCV viremic infection.
Research objectives
The present study was aimed to blindly assess the clinical application of the HCV-Ags EIA in one-step diagnosis of viremic HCV infection in HCV-infected and HCV/HIV-coinfected individuals.
Research methods
The study blindly tested HCV-Ags EIA for its performance in one-step diagnosing viremic HCV infection in 147 sera, 10 without HCV or HIV infection; 54 with viremic HCV monoinfection; 38 with viremic HCV/HIV coinfection; and 45 with viremic HCV and non-viremic HIV coinfection.
Research results
The modified HCV-Ags EIA has a lower detection limit equivalent to serum HCV RNA levels of approximately 100 IU/mL. It is highly sensitive and specific in the setting of HIV coinfection,regardless of HIV infection status and CD4 count.
Research conclusions
These data support the clinical application of the HCV-Ags test in one-step diagnosis of HCV infection in HIV-infected individuals.
Research perspectives
The HCV-Ags EIA will be a novel addition to the current standard and is a more cost-effective one-step HCV screening and diagnosis method.
猜你喜欢
股市动态分析(2021年25期)2021-12-30
小学生学习指导(低年级)(2020年10期)2020-11-09
电子技术与软件工程(2019年24期)2020-01-18
数学大王·低年级(2018年9期)2018-10-24
宇航计测技术(2018年3期)2018-09-08
数学大王·中高年级(2017年2期)2017-02-08
中国信息技术教育(2016年23期)2017-01-03
学苑创造·A版(2016年4期)2016-04-16
哈尔滨理工大学学报(2014年3期)2015-01-04
股市动态分析(2014年27期)2014-07-29
 World Journal of Hepatology2019年5期
World Journal of Hepatology2019年5期
- World Journal of Hepatology的其它文章
- Roles of hepatic stellate cells in acute liver failure: From the perspective of inflammation and fibrosis
- Hepatitis C virus cure with direct acting antivirals: Clinical,economic, societal and patient value for China
- Expanding etiology of progressive familial intrahepatic cholestasis
- Carvedilol vsendoscopic variceal ligation for primary and secondary prevention of variceal bleeding: Systematic review and metaanalysis
- Neonatal cholestasis and hepatosplenomegaly caused by congenital dyserythropoietic anemia type 1: A case report
- Successful treatment of noncirrhotic portal hypertension with eculizumab in paroxysmal nocturnal hemoglobinuria: A case report