
对比剂剂量与肾小球滤过率比值在对比剂肾病中的预测价值
2013-04-24 02:26林德胜杨成明曾春雨张小群
中华老年多器官疾病杂志 2013年3期
林德胜, 杨成明, 范 俊, 冉 希, 曾春雨, 陈 乔, 张小群
对比剂剂量与肾小球滤过率比值在对比剂肾病中的预测价值
林德胜, 杨成明*, 范 俊, 冉 希, 曾春雨, 陈 乔, 张小群
(第三军医大学大坪医院野战外科研究所心内科, 重庆 400042)
探讨对比剂剂量(V)与估算肾小球滤过率(eGFR)的比值(V/eGFR)在经皮冠状动脉介入(PCI)诊疗中与对比剂肾病(CIN)的相关性,进一步明确对比剂剂量与eGFR的比值在对比剂肾病中的预测价值。将先后两次在第三军医大学大坪医院野战外科研究所心内科行PCI诊疗操作的202例冠心病患者分为第一次组和第二次组,收集病史、彩色多普勒超声心动图、肾功能检查、血常规等指标,计算V/eGFR,分析V/eGFR与CIN相关性,通过ROC曲线确立V/eGFR对CIN的预测价值。第一次组,CIN发病率为9.9%;第二次组,CIN发病率为17.3%。多元线性回归分析发现V/eGFR是发生CIN的最重要预测因素。第一次组中,V/eGFR>2.895(OR=1.986,95%CI 1.466~2.691,<0.001)为预测CIN发生的最佳值,第二次组中,V/eGFR>2.320(OR=4.685,95%CI 2.783~7.885,<0.001)为预测CIN发生的最佳值。首次使用对比剂并发生CIN的患者,在再次使用对比剂时,CIN的患病率显著升高,提示V/eGFR可能是一个预测CIN更好的指标。
对比剂肾病; 估算的肾小球滤过率; 对比剂剂量; 冠状动脉造影
对比剂肾病(contrast-induced nephropathy, CIN)是指对比剂注射后2~3d内,新发生的无其他原因可解释的急性肾功能损害,通常以血清肌酐比造影前升高25%或5mg/L(44.2≥µmol/L)作为CIN的诊断标准。近年来,随着冠状动脉造影(coronary angiography,CAG)和经皮管状动脉介入术(percutaneous coronary intervention,PCI)的广泛应用,CIN的数量逐年增加。据统计[1],对比剂是造成住院患者急性肾功能损害的主要原因之一,在院内获得性急性肾损害中位列第三。临床上由于疾病的复杂性和易反复性,使得重复使用对比剂有时又是必要的。目前有研究认为对比剂不仅对肾脏造成急性期损伤,可能还有慢性损伤。对比剂剂量与CIN有很大的相关性[2],也有研究认为对比剂对于那些肾功能正常或经过水化预防性治疗者没有影响[3,4]。最近有研究[5,6]认为对比剂剂量(volume,V)与估算的肾小球滤过率(estimated glomerular filtration rate,eGFR)比值是CIN的良好预测指标。本研究拟探讨对比剂剂量与估算肾小球滤过率的比值(V/eGFR)在初次和再次PCI诊疗中对CIN的预测价值。
1 对象与方法
1.1 研究对象
选取2008年7月至2011年6月先后两次在第三军医大学大坪医院野战外科研究所心内科住院并行CAG和(或)PCI的患者202例,年龄(64.63±9.72)(39~83)岁,其中男性143例,女性59例,两次造影时间间隔为(457.31±246.96)d。术中均使用非离子型低渗造影剂优维显370[Iopromide,碘普罗胺,先灵(广州)药业有限公司],术后至少住院3d。排除标准:心源性休克、肺水肿、终末期肾病需行血液透析治疗、2周内已使用对比剂者、怀孕及哺乳期妇女、正在使用氨基糖甙类、二甲双胍、非类固醇消炎止痛药的患者。将研究对象分为第一次组和第二次组,计算V/eGFR,分析V/eGFR与CIN相关性,通过受试者工作特征(receiver operating charactcristic,ROC)曲线确立V/eGFR对CIN的预测价值。
1.2 方法
所有患者入院后采集病史,术前常规检查血常规、生化、肾功、肝功、血脂、血糖、凝血功能、彩色多普勒超声心动图、胸片和心电图。术前采用MDRD法计算eGFR[ml/(min·m2)][MDRD=186×SCr(mg/dl)-1.154×年龄-0.203×0.724(如果是女性)]。术前6~12h均给予静脉滴注生理盐水1.0~1.5ml/(kg·h),术后12h继续给予静脉输注1.0ml/(kg·h)盐水,如果患者超容量负荷或左室射血分数小于40%,则改为0.5ml/(kg·h)。术后48h复查生化、肾功、血常规等。
1.3 统计学处理

2 结 果
2.1 患者临床特征和CIN患病率
第一次组中有20例发生CIN,患病率为9.9%,第二次组中有35例发生CIN,患病率为17.3%,两次PCI诊疗CIN发生率比较,差异有统计学意义(=0.043)。第1次PCI后发生CIN的患者在第二次PCI后有6例再次发生CIN,发生率为30.0%。糖尿病、高血压病患者分别较未患糖尿病、高血压病者更容易患CIN(表1)。
2.2 两组CIN患者与无CIN患者各指标的比较
比较CIN患者与无CIN患者两组的临床指标,CIN组V/eGFR显著高于无CIN组,差异具有统计学意义(<0.01),而其它临床指标差异无统计学意义(表2)。
2.3 CIN危险因素分析
采用多元logistic回归分析方法,分别将年龄、性别、糖尿病、高血压病、V/eGFR、胱抑素C、血尿酸、血红蛋白、白蛋白、射血分数、收缩压、舒张压、甘油三酯、低密度脂蛋白胆固醇、高密度脂蛋白胆固醇、总胆固醇、血糖、β微球蛋白等18个因素作为发生CIN危险因素进行分析,结果显示,无论是第一次还是第二次PCI诊疗中,糖尿病、高血压与V/eGFR与CIN的发生密切相关(表3;表4)。
2.4 CIN发生率与V/eGFR比值的关系
随着V/eGFR比值的增大,CIN发生率均越来越高(图1)。
2.5 V/eGFR的ROC曲线
根据两组患者V/eGFR的结果,绘制V/eGFR判定CIN的ROC曲线(图2),经图形比较,第一次PCI,ROC曲线下的面积为0.819,95%CI为0.712~0.926,最优截断点为2.895,灵敏度80.0%,特异度为77.5%。第二次PCI,ROC曲线下的面积为0.898,95%CI为0.845~0.950,最优截断点为2.320,灵敏度88.6%,特异度为81.4%。比较两组发生CIN的V/eGFR比值,第一次:5.33±3.44,第二次:4.07±1.78,=1.526,=0.140,差异无统计学意义,但第二次比值小于第一次,说明第二次造影时较小的V/eGFR比值就可能发生CIN;第二次曲线下面积也高于第一次,说明第二次造影V/eGFR比值较第一次更敏感。

表1 患者临床特征和CIN患病率

表2 两组CIN患者与无CIN患者各指标的比较
注: LVEF: 左室射血分数; LDL-C: 低密度脂蛋白胆固醇; HDL-C: 高密度脂蛋白胆固醇。与CIN患者比较,**<0.01
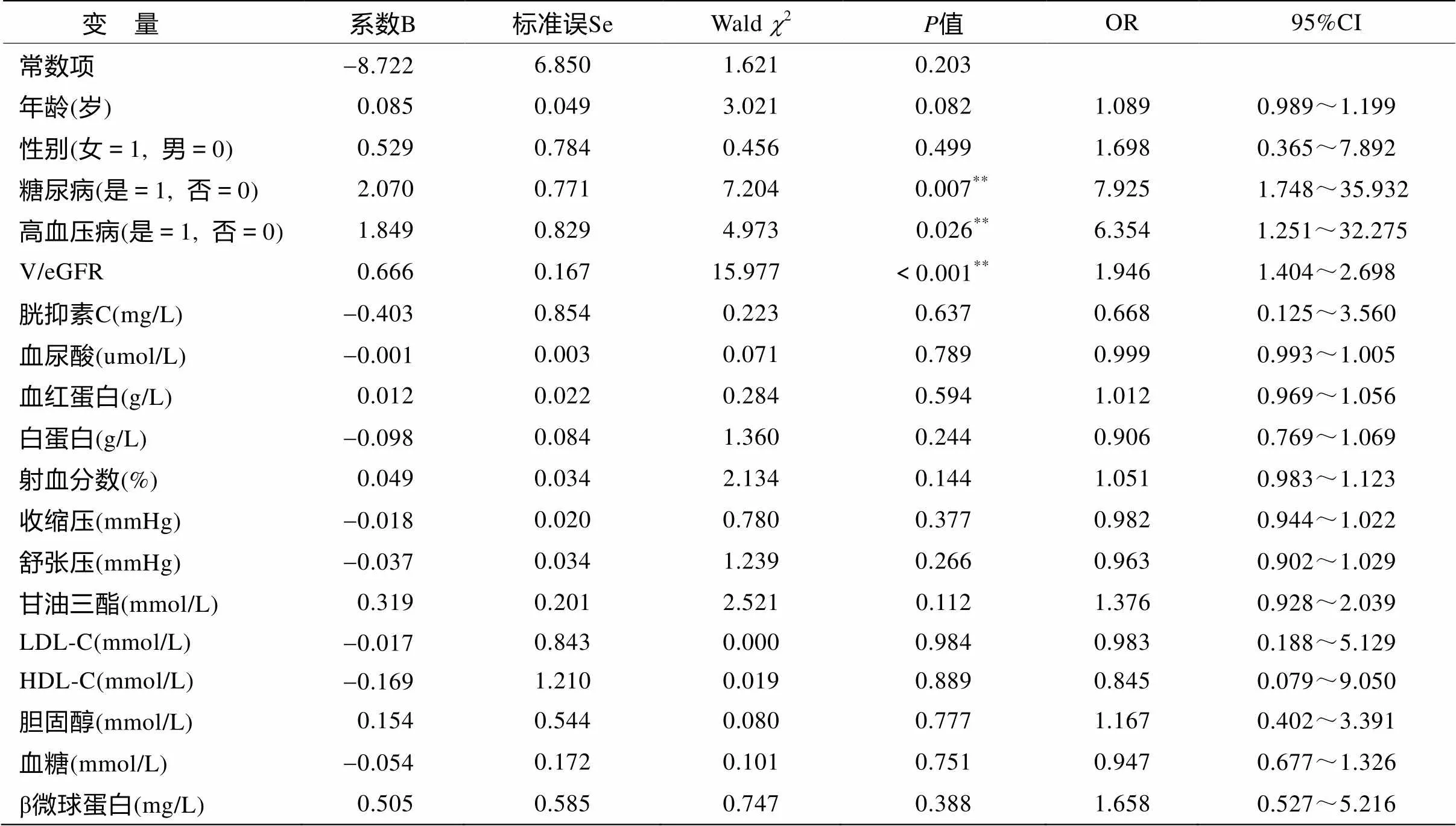
表3 第一次组CIN危险因素分析
注:LDL-C: 低密度脂蛋白胆固醇; HDL-C: 高密度脂蛋白胆固醇。**<0.01

表4 第二次组CIN危险因素分析
注: LDL-C: 低密度脂蛋白胆固醇; HDL-C: 高密度脂蛋白胆固醇。

图1 CIN发生率与V/eGFR比值关系
Figure 1 Relationship between V/eGFR ratio and CIN*<0.05

图2 两次冠状动脉介入诊疗V/eGFR判定CIN的ROC曲线
Figure 2 ROC curve for V/eGFR predicting CIN
3 讨 论
CIN是临床上使用对比剂的主要并发症,随着诊疗技术的发展,特别是心血管介入诊疗的发展,CIN的数量逐年增多。CIN不仅延长住院时间、增加住院费用,增加住院期间病死率,还增加远期病死率、透析、卒中的风险。因此,CIN已成为目前研究的热点。
动物模型显示,注射对比剂后,首先引起血管扩张,继而血管强烈持续收缩,肾脏缺血、缺氧。肾髓质对缺氧最为敏感,导致损伤。对比剂导致的渗透性利尿使血容量减少,引起血管收缩因素和舒张因素的比例失调,加重肾血管收缩,导致肾血流量降低及肾小球滤过率减少,发生缺血缺氧性损伤。对比剂的直接毒性作用和氧化应激等机制均参与CIN的发病过程[7]。
目前尚无效果确切的药物(如N-乙酰半胱氨酸、他汀类)用于CIN的预防[8-10],故术前的预防措施显得特别重要。肾功能损害、大量对比剂均是发生CIN的重要危险因素[11],术前肾功能通常是无法改变的;而可以改变的仅有对比剂剂量,临床上普遍用MDCD公式计算对比剂最大剂量,研究发现:超过最大剂量的患者,术后CIN透析风险和病死率显著增加[12]。因此,寻找一个更合适的公式来估算对比剂剂量显得尤为重要,V/eGFR可能是一个更好地预测CIN的指标[5,6,13]。
Ribichini等[14]观察了216例行CAG的患者,结果发现术后39例发生了CIN,术后30d,仍有15例患者eGFR低于术前25%,这表明对比剂对肾脏可能有慢性损伤。所以,当再次使用对比剂时,肾脏功能可能更加容易受损。但目前关于CIN的报道鲜有区分使用对比剂次数的文献。本研究的目的是给重复PCI的患者确定一个相对安全的V/eGFR值。结果显示V/eGFR是CIN的一个独立预测因素,在第一次PCI中,V/EGFR>2.895[OR=1.986;95%CI 1.466~2.691;<0.001]为预测CIN发生的最佳值;在第二次PCI中,V/EGFR>2.320[OR=4.685;95%CI 2.783~7.885;<0.001]为预测CIN发生的最佳值。所以,在eGFR一定的情况下,PCI过程中应尽量减少对比剂的用量,特别是对于准备再次使用对比剂的患者,更需要注意。我们还发现那些首次使用对比剂并发生CIN的患者,在再次使用对比剂时,CIN的发病率显著高于第一次没有发生CIN者,故对这类患者更要控制对比剂剂量,并在术前术后充分做好水化措施。
本研究也存在一些不足,首先它是单中心小样本研究,其次肾小球滤过率是通过估算获得的,而非直接测定。如能在未来通过大型临床试验来进一步确定V/eGFR的预测价值,将更有说服力。
[1] McCullough PA, Sandberg KR. Epidemiology of contrast-induced nephropathy[J]. Rev Cardiovasc Med, 2003, 4 (Suppl5): S3-S9.
[2] McCullough PA, Adam A, Becker CR,. Risk prediction of contrast-induced nephropathy[J]. Am J Cardiol, 2006, 98[6(Supplement 1)]: 27-36.
[3] Cho JY, Jeong MH, Hwan Park S,. Effect of contrast-induced nephropathy on cardiac outcomes after use of nonionic isosmolar contrast media during coronary procedure[J]. J Cardiol, 2010, 56(3): 300-306.
[4] Davidson C, Stacul F, McCullough PA,. Contrast medium use[J]. Am J Cardiol, 2006, 98(6A): 42K-58K.
[5] Liu Y, Tan N, Zhou YL,. The contrast medium volume to estimated glomerular filtration rate ratio as a predictor of contrast-induced nephropathy after primary percutaneous coronary intervention[J]. Int Urol Nephrol, 2012, 44(1): 221-229.
[6] Wang XC, Fu XH, Wang YB,. Prediction of contrast-induced nephropathy in diabetics undergoing elective percutaneous coronary intervention: role of the ratio of contrast medium volume to estimated glomerular filtration rate [J]. Chin Med J, 2011, 124(6): 892-896.
[7] Cronin RE. Contrast-induced nephropathy: pathogenesis and prevention[J]. Pediatr Nephrol, 2010, 25(2): 191-204.
[8] ACT Investigators. Acetylcysteine for prevention of renal outcomes in patients undergoing coronary and peripheral vascular angiography: main results from the randomized Acetylcysteine for Contrast-induced nephropathy Trial (ACT) [J]. Circulation, 2011, 124(11): 1250-1259.
[9] Anderson, SM, Park ZH, Patel RV,. Intravenous N-acetylcysteine in the prevention of contrast media-induced nephropathy[J]. Ann Pharmacother, 2011, 45(1): 101-107.
[10] Zhang L, Zhang L, Lu Y,. Efficacy of statin pretreatment for the prevention of contrast-induced nephropathy: a meta-analysis of randomised controlled trials[J]. Int J Clin Pract, 2011, 65(5): 624-630.
[11] Stacul F, Van der Molen AJ, Reimer P,. Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines[J]. Eur Radiol, 2011, 21(12): 2527-2541.
[12] Freeman RV, O¢Donnell M, Share D,. Nephropathy requiring dialysis after percutaneous coronary intervention and the critical role of an adjusted contrast dose[J]. Am J Cardiol, 2002, 90(10): 1068-1073.
[13] Nozue T, Michishita I, Iwaki T,. Contrast medium volume to estimated glomerular filtration rate ratio as a predictor of contrast-induced nephropathy developing after elective percutaneous coronary intervention[J]. J Cardiol, 2009, 54, (2): 214-220.
[14] Ribichini F, Graziani M, Gambaro G,. Early creatinine shifts predict contrast-induced nephropathy and persistent renal damage after angiography[J]. Am J Med, 2010, 123(8): 755-763.
(编辑: 王雪萍)
Predictive value of ratio of contrast medium volume to eGFR for contrast-induced nephropathy
LIN Desheng, YANG Chengming*, FAN Jun, RAN Xi, ZENG Chunyu, CHEN Qiao, ZHANG Xiaoqun
(Department of Cardiology, Daping Hospital, Institute of Surgery Research, Third Military Medical University, Chongqing 400042, China)
To explore the relationship of the ratio of contrast medium volume to estimated glomerular filtration rate (eGFR) in percutaneous coronary intervention (PCI) and/or coronary angiography (CAG) with the incidence of contrast-induced nephropathy (CIN), so as to elucidate the predictive value of the ratio for CIN.A total of 202 consecutive consenting patients with coronary heart disease who were given PCI and/or CAG for twice in an interval of (457.31±246.96) d in our department during July 2008 to June 2011 were enrolled. Their medical history, color Doppler echocardiogram, renal function and blood routine examination results at the first and second time of PCI and/or CAG were collected. The ratio of contrast medium volume to eGFR (V/eGFR) at the two performance was calculated, and its correlation with CIN was analyzed. Receiver operating characteristic (ROC) curve was plotted to determine the predictive value of the ratio.The CIN incidence of the cohort during the first time receiving PCI and/or CAG was 9.9% (20/202), while that during the second time was 17.33% (35/202), with significant difference between the two performance (<0.05). Multiple linear regression analysis showed that V/eGFR was the most significant predictive factor of CIN. For the patients who receiving PCI and/or CAG for the first time, the ratio of V/eGFR≥2.895 (OR=1.986, 95% CI=1.466–2.691,<0.001) was the independent predictor of CIN. In the second time, the ratio ≥2.230 (OR=4.685, 95% CI=2.783–7.885,<0.001) was the independent predictor.For the patients having CIN in the first time receiving PCI and/or CAG, they are prone to CIN in the second time, suggesting that the ratio of V/eGFR might be a good predictive index of CIN.
contrast-induced nephropathy; estimated glomerular filtration rate; contrast medium; coronary angiography
R543.3
A
10.3724/SP.J.1264.2013.00049
2012-12-10;
2013-01-23
杨成明, Tel: 023-68757028, E-mail: yangchmi@163.com
猜你喜欢
家庭医药(2022年4期)2022-04-18
昆明医科大学学报(2021年12期)2021-12-30
世界科学技术-中医药现代化(2021年8期)2021-12-21
天津医科大学学报(2021年4期)2021-08-21
天津医科大学学报(2019年6期)2019-08-13
中学生数理化·教与学(2017年4期)2017-04-22
爱你(2016年16期)2016-11-26
新高考·高一物理(2015年4期)2015-08-20
医学研究杂志(2015年9期)2015-07-01
医学研究杂志(2015年12期)2015-06-10
