
A 6-week diet and exercise intervention alters metabolic syndrome risk factors in obese Chinese children aged 11—13 years
2013-06-21 12:53BeibeiLuoYngYngDviNiemnYjunZhngJieWngRuWngPeijieChen
Beibei Luo,Yng Yng,b,Dvi C.Niemn,Yjun Zhng,Jie Wng,Ru Wng, Peijie Chen,*
aKey Laboratory of Exercise and Health Sciences of Ministry of Education,Shanghai University of Sport,Shanghai 200438,China
bShanghai Municipal Center for Students’Physical Fitness and Health Surveillance,Shanghai 200031,China
cHuman Performance Laboratory,Appalachian State University,North Carolina Research Campus,Kannapolis,NC 28081,USA
d458th Hospital of Chinese People’s Liberation Army,Guangzhou 510699,China
Original article
A 6-week diet and exercise intervention alters metabolic syndrome risk factors in obese Chinese children aged 11—13 years
Beibei Luoa,Yang Yanga,b,David C.Niemanc,Yajun Zhanga,Jie Wangd,Ru Wanga, Peijie Chena,*
aKey Laboratory of Exercise and Health Sciences of Ministry of Education,Shanghai University of Sport,Shanghai 200438,China
bShanghai Municipal Center for Students’Physical Fitness and Health Surveillance,Shanghai 200031,China
cHuman Performance Laboratory,Appalachian State University,North Carolina Research Campus,Kannapolis,NC 28081,USA
d458th Hospital of Chinese People’s Liberation Army,Guangzhou 510699,China
Purpose:A randomized,controlled trial was conducted to determine whether a 6-week low calorie diet and aerobic exercise intervention could alter metabolic syndrome(MetS)risk factors in pre-pubescent obese Chinese children.
Methods:The subjects were randomized into diet and exercise(DE)and control(C)groups.The DE group ingested 1600—2000 kcal/day adjusted to each participant’s basal metabolic rate,and engaged in high-volume aerobic exercise(6 days/week,twice daily,for 3 h per session) for 6 weeks.A total of 215 obese children between the ages of 11 and 13 years were recruited into the study,with 167 subjects(DE,n=95;C, n=72)completing all phases.Pre-and post-study measures included body weight,body mass index,waist circumference,body fat percentage, blood pressure and other MetS-related markers from fasting blood samples(serum cholesterol,triglycerides,insulin,and glucose).
Results:Compared to controls,the DE subjects experienced significantly reduced levels for all outcome markers(p<0.05),except for fasting blood glucose in boys(p=0.09).
Conclusion:An intensive,6-week diet and exercise intervention had favorable effects in altering MetS risk factors in obese Chinese children aged 11 to 13.
Copyright©2013,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved.
BMI;Children;Insulin;Obesity;Triglycerides;Waist circumference
1.Introduction
China has experienced marked increases in the prevalence of childhood obesity over the last few decades.The consequences of childhood obesity include an increased incidence of metabolic syndrome(MetS),type 2 diabetes mellitus,and other chronic diseases in adulthood.1MetS is a common metabolic disorder that is caused by obesity.2Its pathophysiology is considered to be increased abdominal fat combined with dyslipidemia,insulin resistance and hyperinsulinemia.3The current epidemic of obesity with an increased risk for MetS constitutes a threat to the health of children in China.4Kong et al.5found that 1.2%of Chinese adolescents in Hong Kong,China suffered from MetS.Li et al.1reported a 3.3%prevalence of MetS in children aged 7 to 17,with more than 50%having at least one MetS risk factor.
Childhood obesity is the result of a prolonged imbalance between energy intake and expenditure.The decline in physical activity and the increased intake of high-calorie diets over thepast decades are thought to be the primary causative factors for the development of obesity and MetS.6Increasing physical activity is associated with improved body fitness,weight control, and a lowered risk of MetS,7and combined diet and exercise interventions have great potential for improving the metabolic profile.8In a preliminary,non-randomized study,favorable changes in anthropometric and metabolic parameters were measured in 26 obese Chinese children following a 4-week exercise and low-calorie die intervention.9
Therefore,the purpose of this study was to further evaluate the efficacy of a short-duration diet and exercise intervention in altering MetS risk factors.The major outcome measures included changes in waist circumference(WC),blood pressure,body mass index(BMI),body composition,insulin sensitivity,lipid profiles,and other MetS risk factors defined by the International Diabetes Federation(IDF)in 200710and utilized in previous epidemiologic studies.11
2.Methods
2.1.Participants
The subjects included 167 obese boys and girls,aged 11—13 years,who were recruited through the Shanghai Student Physical Fitness Monitoring Program and the Weight Loss Camp in the Shanghai University of Sport between 2009 and 2012.To enter the study,the subjects had to be:(1)at a pre-pubescent stage as determined from questionnaires and physical examinations performed by pediatricians;(2)have a BMI above 23.6 kg/m2,24.7 kg/m2,and 25.7 kg/m2for ages 11,12,and 13,respectively;12(3)have a WC above the 90th percentile of children in Shanghai(79.24 cm,81.37 cm, 82.73 cm,for boys aged 11,12,and 13,respectively;and 72.99 cm,74.89 cm,76.23 cm for girls aged 11,12,and 13, respectively);13and(4)agree to be randomized into intervention or control groups,and be willing to adhere to all aspects of the research design.Written informed consent was obtained from the subjects and their parents,and the experimental procedures were approved by the institutional review board of the Shanghai University of Sport.
2.2.Diet and exercise intervention
The subjects were randomized into diet and exercise(DE) (Weight Loss Camp)and control(C)groups(normal lifestyle patterns in the Shanghai Student Physical Fitness Monitoring Program)for 6 weeks.The DE intervention was similar to the regimen used in a previous study.14Participants in the 6-week intervention group(DE)received well-defined and balanced daily meals.The food intake energy level was individualized for each participant(1600—2000 kcal/day)based on their basal metabolic rate requirements as calculated using the Mifflin equation for overweight and obese subjects,and the China Food Composition tables.15-17Briefly,three wellbalanced meals were provided each day with the following macronutrient allocations(percent of total energy intake): protein 30%,carbohydrate 50%,and fat 20%.Breakfast accounted for 35%of the total daily energy intake,lunch 40%, and supper 25%.The diet included important nutrients such as vitamins,minerals,essential amino acids,fiber,and polyunsaturated fatty acids at adequate levels.
The intervention group engaged in high volumes of moderate exercise(6 days/week,twice daily,for 3 h per session) during the 6-week study period.The program began with 30 min warm up followed by 2 h of moderate aerobic exercise (heart rate 120—150 beats per minute),and included brisk walking,jogging,or swimming in morning,and table tennis or badminton in the afternoon,followed by 30 min relaxation. The heart rate was measured by palpation every 30 min.The emphasis of the exercise program was on enjoyment and safety,not competition or skill development.
2.3.Data collection
A standard questionnaire was administered to the participants and their parents by trained staff at the baseline examination to obtain information about personal and family medical history.Body weight,height,and waist circumference were measured twice with the participant wearing indoor clothing withoutshoes.The waistcircumference was measured 1 cm above the participant’s navel during light breathing.Percentagebody fatwasmeasured by bioimpedence analysis(TBF-215,Tanita,Tokyo,Japan).Blood pressure(BP)measurements were obtained in the morning with the participant in the sitting position after a 15-min rest by a sphygmomanometer(BP742,Omron Healthcare,Bannockburn,IL,USA)according to standard protocols.
Overnight fasting blood specimens were obtained for the measurement of insulin,glucose,and lipid concentrations.The blood samples were drawn at 7:00 am to 9:00 am,with all subjects having avoided food and beverage intake other than water for at least 8 h.The blood samples were drawn from an antecubital vein in overnight-fasted subjects in the seated position and rested for at least 15 min.The blood samples were centrifuged,and the plasma was aliquoted and stored at -80°C until analysis.Fasting blood insulin(FBI)levels were measured with the use of an enzyme immunoassay method (AIA-PACK,Tosoh,Tokyo,Japan).The fasting blood glucose (FBG)concentration was measured with a modified hexokinase enzymatic method(7020 clinical analyzer,Hitachi, Tokyo,Japan).The homeostasis model assessment of insulin resistance(HOMA-IR)was used to measure the changes in insulin sensitivity,and was calculated using the following formula:fasting plasma insulin(μIU/mL)×fasting plasma glucose(mmol/L)/22.5.18A serum lipid panel was performed by our clinical hematology laboratory.The clinical laboratory staff were blinded to the treatment assignments,and the study coordinators were unaware of all outcome data until the end of the intervention.
2.4.Statistical analysis
The data were analyzed using a 2× 2(group× time) repeated-measures analysis of variance between subjectsmodel for each gender separately.An independentttest was used to compare the baseline data between the DE and C groups,the data of changes between the DE and C groups,and the data between boys and girls.All data were presented as means±SD(95%confidence intervals).All analyses were conducted with SPSS software(version 17.0,SPSS Inc., Chicago,IL,USA),and ap<0.05 was considered statistically significant.
3.Results
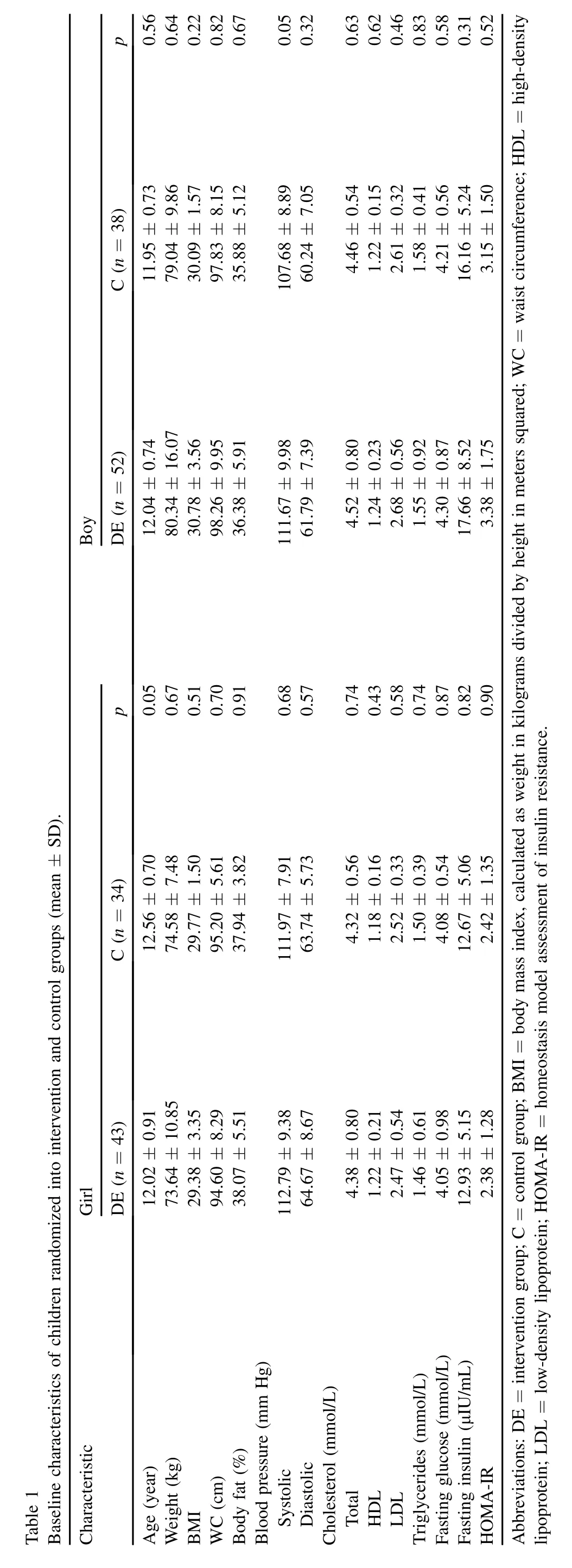
3.1.Participants
3.2.Effects of treatment
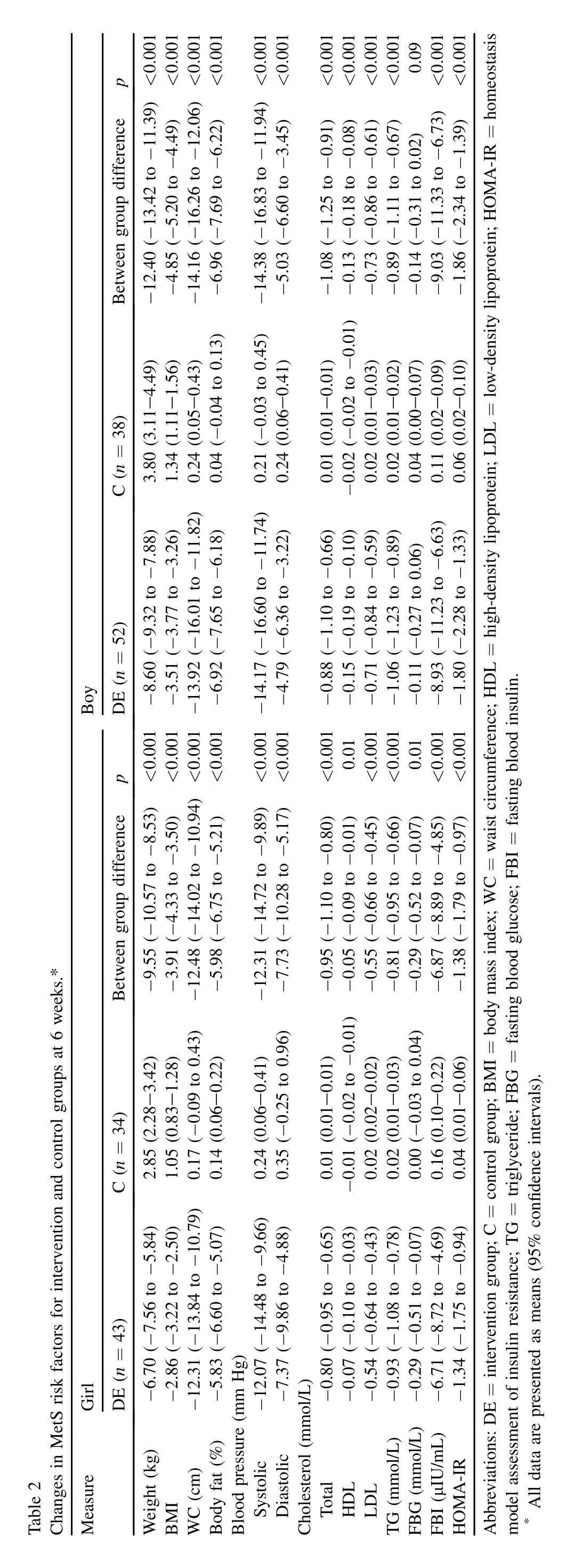
As shown in Table 2 and Fig.2,the body weight,BMI, WC,and percent body fat were reduced in the DE group as compared to increases in the C group.The differences between the two groups for the changes in body weight(-12.40 kg in boys and-9.55 kg in girls),BMI(-4.85 in boys and-3.91 in girls),WC(-14.16 cm in boys and-12.48 cm in girls)and percentage body fat(-6.96%in boys and-5.98%in girls) after 6 weeks were all statistically significant(p< 0.001). Systolic and diastolic blood pressures decreased significantly in the DE group relative to no change in the C group (p<0.001).The serum cholesterol concentrations decreased in the DE group relative to an increase in the controls (p<0.001)with exception in girls’high-density lipoproteincholesterol(HDL-C)(p=0.01)after 6 weeks.Only in the girls was a significant reduction in FBG observed(p=0.01), whereas FBG was unchanged in the boys(p=0.09).The mean FBI concentrations fell by 8.93 μIU/mL in the boys and 6.71 μIU/mL in the girls at 6 weeks in the DE group as compared to the increases in the C group(p<0.001).Thedifferences in the changes in the HOMA-IR between the DE and C groups at 6 weeks(-1.80vs.0.06 in boys and-1.34vs.0.04 in girls)were statistically significant(p< 0.001). Additionally,DBP,FBG,HDL-C,and low-density lipoproteincholesterol(LDL-C)were changed differently in the boys and girls after a 6-week diet and exercise intervention.The DBP and FBG were reduced greater in the girls,while the decrease in the HDL-C and LDL-C level were more prominent in the boys(p<0.05,Fig.2).
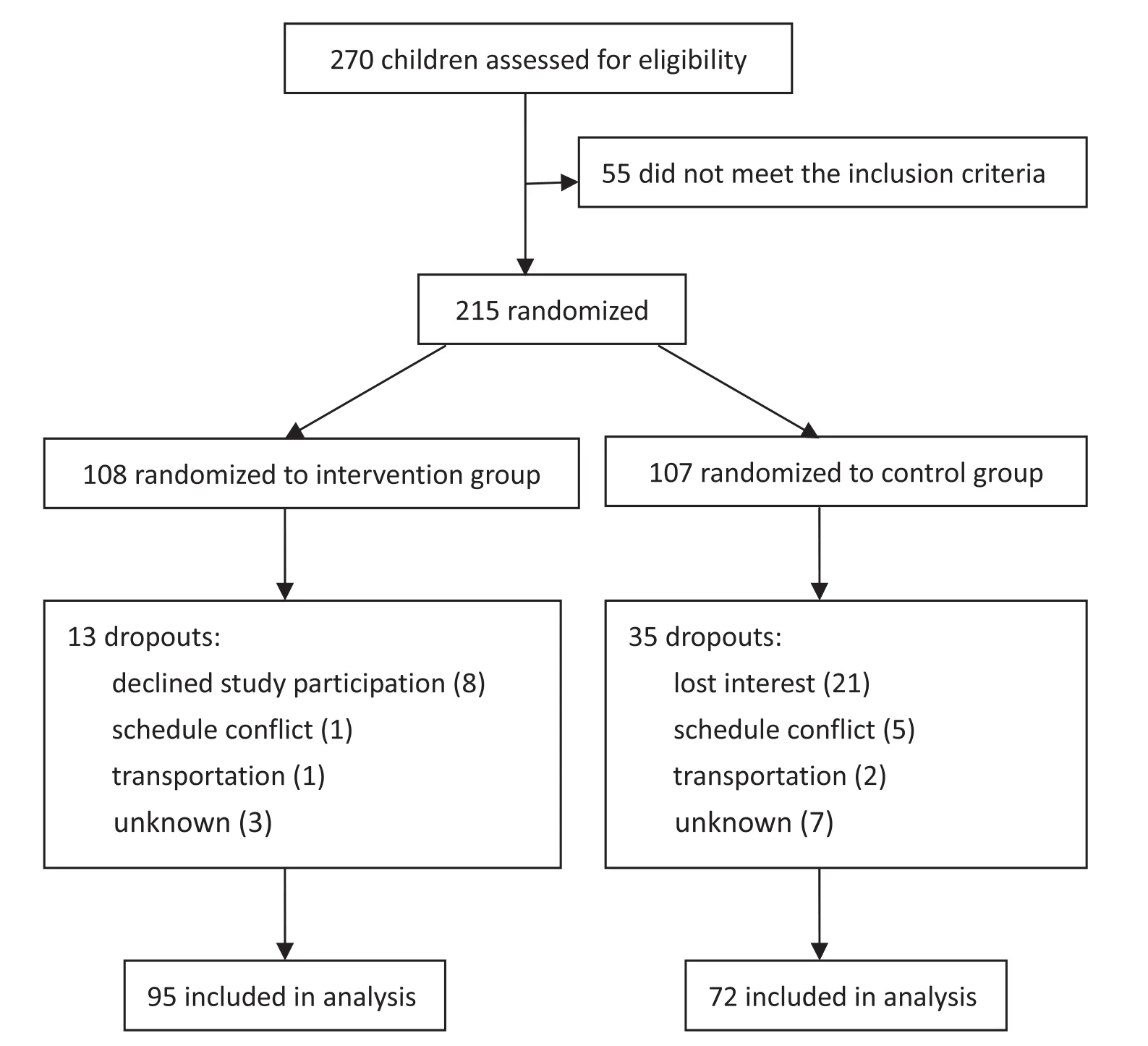
Fig.1.Enrollment,randomization,and dropout of the study participants.
?
?

Fig.2.Changes in metabolic risk factors:weight,body mass index(BMI),waist circumference(WC),body fat percentage,systolic blood pressure(SBP),diastolic blood pressure(DBP),total cholesterol(TC),high-density lipoprotein-cholesterol(HDL-C),low-density lipoprotein-cholesterol(LDL-C),triglyceride(TG), fasting blood glucose(FBG)and insulin(FBI),and homeostasis model assessment of insulin resistance(HOMA-IR)for control(C)and diet and exercise intervention groups(DE).All data are shown as the percentage changes in relation to the baseline value.*p<0.05,EDvs.C;†p<0.05,girlsvs.boys.
3.3.The prevalence of MetS in the DE group
Before the intervention,10 children in the DE group were diagnosedasMetSpatientsaccordingtothe2007IDFcriteria.10All children in the DE group had at least one MetS risk factor: WC≥90th percentile for ages 11—13(95/95,100%),systolic blood pressure(SBP)≥130 mmHg(4/95,4.21%),diastolic blood pressure(DBP)≥85 mmHg(1/95,1.05%),triglyceride (TG)≥1.7 mmol/L(29/95,30.53%),HDL-C<1.03 mmol/L (19/95,20%),or fasting blood glucose(FBG)≥5.6 mmol/L (1/95,1.05%).Aftertheintervention,noneofthechildreninthe DE group were classified as having MetS.The number of children having MetS risk factors also dropped:SBP≥130 mmHg (decrease 100%),DBP ≥ 85 mmHg(decrease 100%), FBG≥5.6 mmol/L(decrease 100%),TG≥1.7 mmol/L(1/95, 1.05%,decrease 96.55%),and WC≥90th percentile for ages 11—13(68/95,71.58%,decrease 28.42%).
4.Discussion
In this randomized,controlled 6-week study of a group of 167 obese children,a low-calorie diet in combination with high volumes of moderate exercise significantly lowered MetS risk factors such as BMI,WC,BP,serum cholesterol and TGs,and FBI.In a previous study,we showed that supervised exercise improved the neutrophil-to-lymphocyte ratio.13In another study,a 12-week dietand physical activityintervention reduced MetS risk factors without changes in systemic inflammation in obese children from the United States.19The major strengths in our study included the use of a randomized design,the enrollment of both males and females,careful monitoring of the diet, and supervised exercise sessions for all DE subjects.We found some gender-specific differences in MetS risk factor changes, suggestingthatpre-pubescentgirlsandboysmaynotrespondin the same way to diet and exercise interventions.
Anthropometric outcome measures showed positive changes in the obese children following the lifestyle intervention,with 6%—8%decreases in body weight,BMI,and WC.The percentage change in the WC was greater than for the BMI and weight in the DE subjects,suggesting that diet and exercise intervention may preferentially reduce abdominal fat in obese children and thus lower the risk of MetS.20
The systolic and diastolic blood pressures have increased substantially among children and adolescents in China,and is likely to increase the incidence of early hypertension.21Both acute and chronic moderate exercise have an effect in reducing BP.Sharman et al.22reported that an acute 10-min bout of moderate aerobic exercise reduced the brachial SBP and DBP in healthy adults.Roberts et al.23found that a short-term, rigorous diet and exercise intervention reduced both SBP and DBP by 10%in overweight children.In our study,we found similar decreases in blood pressure after the 6-week,lowcalorie diet and high volume moderate exercise intervention.
The prevalence of insulin resistance is increasing,and is considered to be a major pathophysiological factor responsible for many clinical complications of childhood obesity.11Therefore,wemeasuredthechangesinHOMA-IRinthetwogroupsas a surrogate riskfactor.Similartothe anthropometric parameters, the HOMA-IR decreased in the DE group as compared to an increaseinthecontrols,withsubstantialchangesinbothboysand girls(-1.80 and-1.34,respectively).Exercise is known to increase insulin receptor auto-phosphorylation,glucose transporter-4 expression,and glucose transport.24The factors responsible for the changes in the insulin profile in our subjects are likely due to improved insulin sensitivity from increased physical activity and the low-calorie diet.25Despite improvements in both HOMA-IR and insulin levels,no changes in FBG levels were measured in the boys,as reported by others.26
“咦?”霍铁和小达忍不住叫了出来。小达仔细端详着小姑娘,然后哈哈大笑起来。她扭头扯了扯霍铁的胳膊:“哥哥,你忘了?几个月前的那次体操表演赛,我还采访过她呢!”
Obesecomparedtonon-obesechildrenoftenconsume larger amounts of processed carbohydrates.27The diet used in this intervention program was largely devoid of re fined carbohydrates.The improvement in TG experienced by the DE subjects was primarily due to the combination of the low-calorie,unrefined-high fiber carbohydrate diet and the large volumes ofmoderatephysicalactivity.Thedecreaseininsulinalsoplayeda role in reducing TG levels.A 3-month study utilizing a lowcarbohydratedietalsofounda20%—25%decreaseinTGlevels in obese adults.28In our 6-week study of obese children,the TC also decreased 0.65—1.10 mmol/L.Nieman et al.29reported a 0.6—0.8 mmol/L decrease in TC in overweight women following 12-week of energy restriction and exercise training. The LDL-C decreased 0.54 mmol/L in the girls and 0.71 mmol/lin the boys,similar to what has been reported in previous studies using diet and exercise interventions.23,29The HDL-C decreased in the DE group as compared to the controls,which has been reported in other studies when subjects are experiencing strong decreases in body weight.26
Our study has several limitations.The duration of our intervention program was 6 weeks,and the follow-up was limited due to the summer vacation period.We combined data from 2009 to 2012,with a focus on MetS risk factors,but not other important clinical end points.Futurestudies may focus on thelong-termbenefitstoMetSriskfactorsafter 6-week dietand exercise interventions in children,and a cost-benefit analysis.
In conclusion,an intensive low-calorie diet and exercise program was associated with substantial improvements in MetS risk factors such as BMI,WC,BP,insulin sensitivity, and serum TC and TG levels.These data support the value of short-term lifestyle interventions in reducing disease risk factors in obese Chinese children.
Acknowledgments
This study was supported by the Shanghai Key Laboratory ofHuman Performance (NO.11DZ2261100),Grants yjscx2012007 and xsxr2012045.We thank Professor Wenhe Chen and all the staff at the Shanghai Dianfeng Sports and Health Management Co.Ltd.for their assistance.
1.Li Y,Yang X,Zhai F,Piao J,Zhao W,Zhang J,et al.Childhood obesity and its health consequence in China.Obes Rev2008;9:82—6.
2.Cook S,Weitzman M,Auinger P,Nguyen M,Dietz WH.Prevalence of metabolic syndrome phenotype in adolescents:findings from the third National Health and Nutrition Examination Survey 1988—1994.Arch Pediatr Adolesc Med2003;157:821—7.
3.Alberti KG,Zimmet P,Shaw J.The metabolic syndrome:a new worldwide definition.Lancet2005;366:1059—62.
4.Chen F,Wang Y,Shan X,Cheng H,Hou D,Zhao X,et al.Association between childhood obesity and metabolic syndrome:evidence from a large sample ofChinese children and adolescents.PLoSOne2012;7:e47380.
5.Kong AP,Ko GT,Ozaki R,Wong GW,Tong PC,Chan JC.Metabolic syndrome by the new IDF criteria in Hong Kong Chinese adolescents and its prediction by using body mass index.Acta Paediatr2008;97:1738—42.
6.Telford RD.Low physical activity and obesity:causes of chronic disease or simply predictors?Med Sci Sports Exerc2007;39:1233—40.
7.Salmon J,Booth ML,Phongsavan P,Murphy N,Timperio A.Promoting physical activity participation among children and adolescents.Epidemiol Rev2007;29:144—59.
8.Weiss R,Dziura J,Burgert TS,Tamborlane WV,Taksali SE,Yeckel CW, et al.Obesity and the metabolic syndrome in children and adolescents.N Engl J Med2004;350:2362—74.
9.Luo BB,Zhang YJ,Wang R,Chen PJ.6-week lifestyle intervention on anthropometry,body composition and risk factors for metabolic syndrome in Chinese obese children.In:Proceedings of the 2010 international symposium on children and youth fitness and health2010.p.262—6.
10.Zimmet P,Alberti KG,Kaufman F,Tajima N,Silink M,Arslanian S,et al. The metabolic syndrome in children and adolescents:an IDF consensus report.Pediatr Diabetes2007;8:299—306.
11.Liu W,Lin R,Liu A,Du L,Chen QP.Prevalence and association between obesity and metabolic syndrome among Chinese elementary school children:a school-based survey.BMC Public Health2010;10:780.
12.Group of China Obesity Task Force.Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents.Zhonghua Liuxing Bing Xue Za Zhi2004;25:97—102.[In Chinese].
13.Wu Y,Yang Y,Peng N,Hong F,Yan W,Zhou G.Waist circumference and waist circumference percentile curves for children and adolescents in Shanghai.Zhongguo Xuexiao Weisheng2012;33:1334—7.[In Chinese].
14.Wang R,Chen P,Chen W.Diet and exercise improve neutrophil to lymphocyte ratio in overweightadolescents.IntJSportsMed2011;32:982—6.
15.Mifflin MD,St Jeor ST,Hill LA,Scott BJ,Daugherty SA,Koh YO.A new predictive equation for resting energy expenditure in healthy individuals.Am J Clin Nutr1990;51:241—7.
16.Weijs PJ.Validity of predictive equations for resting energy expenditure in US and Dutch overweight and obese classiand II adults aged 18—65 y.Am J Clin Nutr2008;88:959—70.
17.Yang Y.China food composition.Beijing:Peking University Medical Press;2005.p.75—213.
18.Matthews DR,Hosker JP,Rudenski AS,Naylor BA,Treacher DF, Turner RC.Homeostasis model assessment:insulin resistance and beta cell function from fasting plasma glucose and insulin concentration in man.Diabetologia1985;28:412—9.
19.Christiansen T,Paulsen SK,Bruun JM,Pedersen SB,Richelsen B.Exercise training versus diet-induced weight-loss on metabolic risk factors and inflammatory markers in obese subjects:a 12-week randomized intervention study.Am J Physiol Endocrinol Metab2010;298:E824—31.
20.Zimmet P,Alberti G,Kaufman F,Tajima N,Silink M,Arslanian S,et al. The metabolic syndrome in children and adolescents.Lancet2007;369:2059—61.
21.Chen X,Wang Y.Tracking of blood pressure from childhood to adulthood:a systematic review and meta-regression analysis.Circulation2008;117:3171—80.
22.Sharman JE,McEniery CM,Campbell R,Pusalkar P,Wilkinson IB, Coombes JS,et al.Nitric oxide does not significantly contribute to changes in pulse pressure amplification during light aerobic exercise.Hypertension2008;51:856—61.
23.Roberts CK,Chen AK,Barnard RJ.Effect of a short-term diet and exercise intervention in youth on atherosclerotic risk factors.Atherosclerosis2007;191:98—106.
24.Stiegler P,Cunliffe A.The role of diet and exercise for the maintenance of fat-free mass and resting metabolic rate during weight loss.Sports Med2006;36:239—62.
25.Misra A,Alappan NK,Vikram NK,Goel K,Gupta N,Mittal K,et al. Effect of supervised progressive resistance-exercise training protocol on insulin sensitivity,glycemia,lipids,and body composition in Asian Indians with type 2 diabetes.Diabetes Care2008;31:1282—7.
26.Savoye M,Shaw M,Dziura J,Tamborlane WV,Rose P,Guandalini C, et al.Effects of a weight management program on body composition and metabolic parameters in overweight children:a randomized controlled trial.J Am Med Assoc2007;297:2697—704.
27.St-Onge MP,Keller KL,Heymsfield SB.Changes in childhood food consumption patterns:a cause for concern in light of increasing body weights.Am J Clin Nutr2003;78:1068—73.
28.Foster GD,Wyatt HR,Hill JO,McGuckin BG,Brill C,Mohammed BS, et al.A randomized trial of a low-carbohydrate diet for obesity.N Engl J Med2003;348:2082—90.
29.Nieman DC,Brock DW,Butterworth D,Utter AC,Nieman CC.Reducing diet and/or exercise training decreases the lipid and lipoprotein risk factors of moderately obese women.J Am Coll Nutr2002;21:344—50.
21 August 2012;revised 19 March 2013;accepted 3 May 2013
*Corresponding author.
E-mail address:chenpeijie@sus.edu.cn(P.Chen)
Peer review under responsibility of Shanghai University of Sport
2095-2546/$-see front matter Copyright©2013,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved. http://dx.doi.org/10.1016/j.jshs.2013.05.001
猜你喜欢
作文大王·笑话大王(2022年8期)2022-07-10
环球时报(2020-11-30)2020-11-30
延河·绿色文学(2020年6期)2020-09-10
幼儿教育·父母孩子版(2019年6期)2019-10-18
畅谈(2019年10期)2019-06-27
体育时空(2018年3期)2018-09-29
当代贵州(2016年37期)2016-11-23
文理导航·趣味课堂(2016年5期)2016-07-21
文理导航·趣味课堂(2016年4期)2016-06-01
文理导航·趣味课堂(2016年3期)2016-04-26
 Journal of Sport and Health Science2013年4期
Journal of Sport and Health Science2013年4期
- Journal of Sport and Health Science的其它文章
- The effects of Tai Chi exercise on cognitive function in older adults: A meta-analysis
- Effects of resistance and Tai Ji training on mobility and symptoms in knee osteoarthritis patients
- Process and outcome evaluation of the“No more smoking!It’s time for physical activity”program
- ActiGraph GT3X determined variations in“free-living”standing, lying,and sitting duration among sedentary adults
- Human neuromuscular structure and function in old age:A brief review Geoffrey A.Powera,*,Brian H.Daltonb,Charles L.Ricec,d
- Current concepts in sport concussion management:A multifaceted approach