
Prevalence of autism spectrum disorders among children in China: a systemati c review
2013-12-11 05:14YumeiWANQiangFUTingLILijuanJIANGYasongDULeiFENGJohnCheeNengWONGChunboLI
上海精神医学 2013年2期
Yumei WAN, Qiang FU, Ting LI, Lijuan JIANG, Yasong DU, Lei FENG, John Chee-Neng WONG,,Chunbo LI*
1上海交通大学医学院附属精神卫生中心 上海
2 Department of Psychological Medicine, Yong Loo Lin School of Medicine, National University of Singapore,Singapore
3 Department of Psychological Medicine, National University Hospital, Singapore
·Meta-analysis·
Prevalence of autism spectrum disorders among children in China: a systemati c review
Yumei WAN1, Qiang FU1, Ting LI1, Lijuan JIANG1, Yasong DU1, Lei FENG2, John Chee-Neng WONG2,3,Chunbo LI1*
1. Introduction
Autism is a developmental disorder with an onset during early childhood that results in social deficits, communication deficits, stereotyped interests, and repetitive behaviors.[1]Recently the term ‘autism spectrum disorders’ (ASD) has been used to describe a group of disorders that include autism and similar types of disorders.[2]The conditions included under the ASD label vary slightly between the three diagnostic systems commonly used in China - the 3rdedition of the Chinese Classification and Diagnostic Criteria of Mental Disorders;[3]the 10thedition of the International Classification of Diseases (ICD-10);[4]and the 4thedition of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).[5]In all three diagnostic systems, ASD includes autism, atypical autism, Rett syndrome, childhood disintegrative disorder,Asperger syndrome, and pervasive developmental disorder not otherwise specified (PDD-NOS). The ASD diagnosis in ICD-10 also includes ‘overactive disorder associated with mental retardation and stereotyped movements’. Rett syndrome will be excluded from the ASD diagnosis in the forthcoming DSN-5.[6]
Prevalence studies conducted by the United States Centers for Disease Control and Prevention[7-9]and others centers[10-12]have documented a rapid increase in the prevalence of ASD. A meta-analysis conducted by Williamsand colleagues in 2006[13]reported a pooled estimate of prevalence of 7.1 per 10 000 for autism, and 20.0 per 10 000 for ASD among individuals under the age of 18.Another meta-analysis conducted by Fombonne and colleagues in 2009[14]summarized data from 57 studies and yielded a pooled prevalence of 22 per 10 000 for autism and 60 to 70 per 10 000 for ASD. Elsabbagh and colleagues[15]reviewed studies conducted after the year 2000 and found a median prevalence of 17 per 10 000 for autism and 62 per 10 000 for ASD.

Figure 1. Identification of studies included in the meta-analysis
Information from China has not figured prominently in these prevalence estimates for autism and ASD: the 2006 analysis by Williams[13]included no data from China;the 2009 analysis by Fombonne[14]included one study from Fong Kong; and the 2012 report from Elsabbagh[15]combined data from China and Japan together as the‘Western Pacific region’. Nost studies on the prevalence of ASD in mainland China have been provincial studies with relatively small sample sizes that report wide variati ons in prevalence.[16-18]The only national study, a study conducted by Li and colleagues in 2011,[19]reported a very low prevalance of autism (2.4 per 10 000). The current report is a systematic review and meta-analysis of prevalance studies on autism and ASD from mainland China, Fong Kong and Taiwan.
2. Methods
2.1 Identification of studies for inclusion in the metaanalysis
The process of identifying studies for inclusion in the meta-analysis is shown in Figure 1. Two authors (YW and QF) first conducted electronic searches in the following databases: the Chinese Nati onal Knowledge Infrastructure database (CNKI, 1979-2013), the Chongqing VIP database for Chinese Technical Periodicals (1989-2013), the WANFANG DATA database (1990-2013), the Chinese Biological Nedical Literature Database (1978-2013),Pubmed (1966-2013), and Web of Science (1950-2013).All reports published by 28 February 2013 were included in the search. All articles in which any word denoting autism (including ‘autism spectrum disorders’, ‘pervasive developmental disorders’, ‘autism’, ‘autism disorder’, ‘zi bi zheng’ [an older term for auti sm in Chinese], ‘Asperger’,‘Asperger syndrome’) in either Chinese or English occurred with any word denoting prevalence (including ‘prevalence’,‘detectable rate’, ‘incidence rate’, and ‘epidemiology’) in either Chinese or English were identified. Reference lists of identi fi ed studies were hand-searched.
Included studies were epidemiological studies about the prevalence of auti sm or ASD (as def i ned by CCND[3],ICD[4]or DSN[5]diagnosti c criteria) among Chinese individuals (including those from mainland China,Fong Kong, Nacau, and Taiwan) under the age of 18 who were identified from the general population, from clinical populations, or from student populations. Non-human studies, unpublished reports, reviews, and case reports were excluded. The report of the study had to provide the sample size and estimates of the prevalence of auti sm or ASD based on the use of a valid diagnostic tool or data from an authoritative health monitoring system.
First, all studies were imported to the literature management soft ware Endnote X5 to eliminate duplicated records. Two authors (WY and FQ) independently conducted a preliminary screening of reports by reading titles and abstracts and then the full texts of potentially relevant arti cles were downloaded for the second round of screening. The above inclusion criteria were used to select studies for the analysis. There were six arti cles in which the initial screening result about whether or not to include the article differed between the two raters; after discussion, a third reviewer (TL) made the final decision about inclusion of these articles.
2.2 Data extraction
Two authors (WY and FQ) independently extracted and entered relevant data about the included studies. For each study the basic characteristics of the study (i.e., name of first author; year of publication; location of study; source of sample, sampling method, sample size and number of potential subjects not screened; breakdown of sample by gender, ethnicity, and urban versus rural residence;method of screening and diagnosis) and the reported prevalences of autism and ASD were recorded. Reports of ‘current prevalence’ and ‘point prevalence’ were both included.[20]If prevalence by gender, age group, urban versus rural residence, or ethnicity (Fan versus other) was provided, this was also recorded.
The quality of the reports of the included studies was assessed using the guidelines recommended for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).[21]This guideline lists 22 criteria,covering specif i c elements of the methods, presentation of the results, and interpretation of the results that are considered important for assessing the integrity of a study.One point was given for each of these elements that was present in the report, so the total score for quality ranged from 0 to 22 points. The inter-rater reliability of the two raters for this quality score was excellent (intraclass correlation coefficient [ICC], 0.96).
2.3 Statistical analysis
After checking for consistency, the Netaprop module in the R-2.15.2 statistical soft ware package was used for the meta-analysis; the prevalence reported in each study was logit transformed prior to computing the pooled prevalence.[13]Tests of heterogeneity were conducted to decide which method would be used to pool the results.Results were considered homogenous when the I2statistic( the percentage of variance due to heterogeneity) was less than 50% and the p-value for the test of heterogeneity was >0.10, in these cases a fixed-effect model was used to compute the pooled estimate of prevalence. In all other cases (i.e., I2>50% or p<0.10) the studies were considered heterogeneous and a random-effect model was used to compute the pooled prevalence.[22]When heterogeneity was present, a sensitivity analysis was conducted to inspect possible reasons for heterogeneity. Subgroup analyses were conducted by gender, urban versus rural residence, source of the study population, and year of publication. Begg’s rank method was used to assess potential publication biases.[23]
3. Results
3.1 Characteristics of identified studies
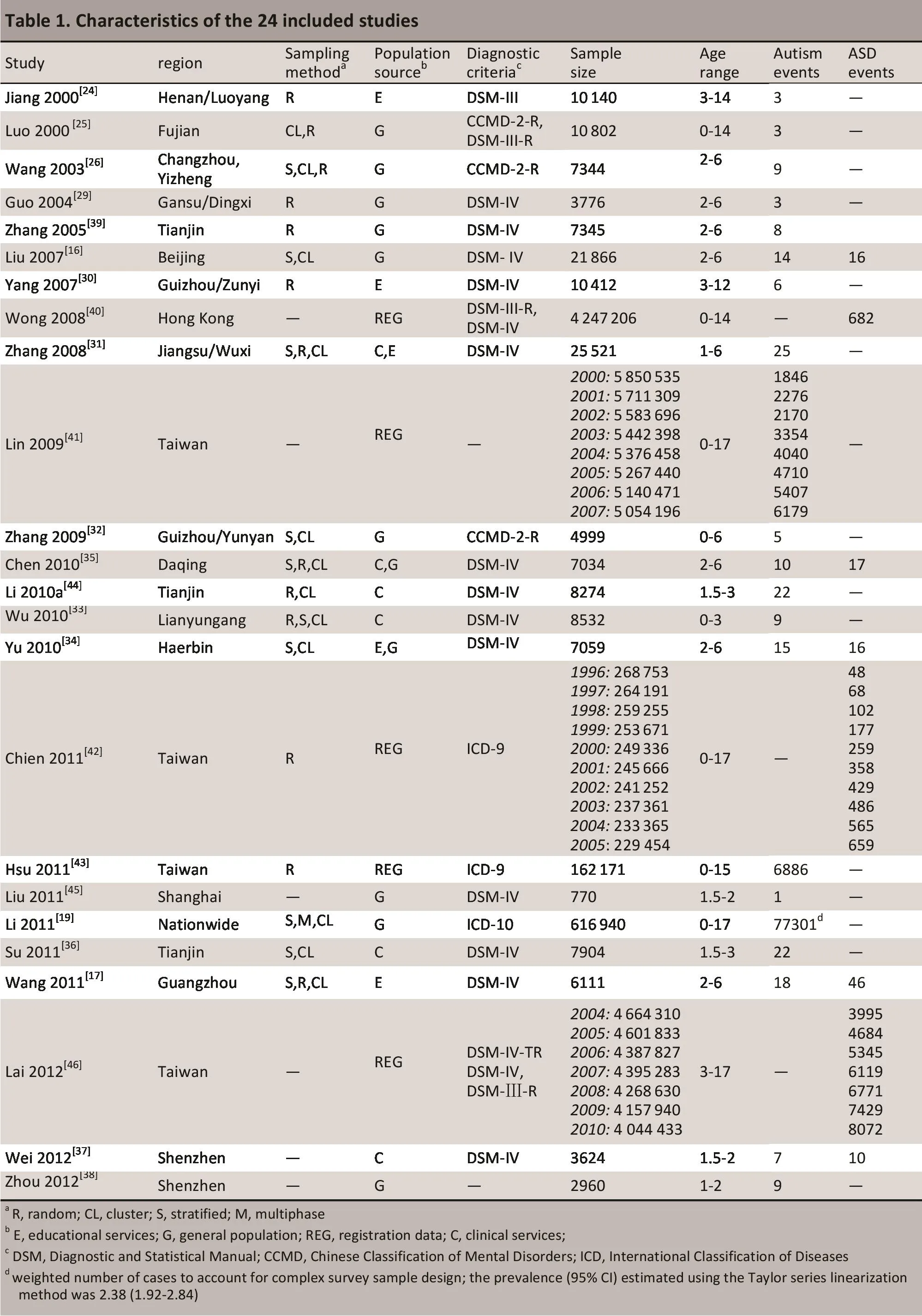
As shown in Figure 1, 30 studies were identified that met the inclusion criteria; 23 of these publications were in Chinese and 7 in English.[16,17,19,24-50]Several sets of reports were from the same study: Wang (2002)[47]and Wang (2003)[26]; Fuang (2010)[48]and Chen (2010)[35]; Li(2010a)[44]and Li (2010b)[49]; Wu[33]and Wang[50]; and Zhang (2005)[39], Zhang (2004)[28]and Guo (2004).[27]Thus,a total of 24 separate studies were identified[16,17,19,24-26,29-46]including 19 population-based screening and diagnostic studies in mainland China[16,17,19,24-26,29-39,44,45](with a combined sample of 771 413 children) and 5 prevalence reports based on health registry data in Fong Kong and Taiwan[40-43,46](covering a total of 14 570 369 children).Details of the included studies are shown in Table 1.
3.2 Reported prevalence of autism in the registry studies from Taiwan and Hong Kong
Wong and colleagues[40]reported an interval prevalence of 16.1 per 10 000 in Fong Kong during the period of 1986 to 2005. In Taiwan Fsu and colleagues[43]reported a 12-month prevalence of 424.6 per 10 000 individuals under the age of 15 in 2007; Lin and colleagues[41]reported that the 12-month prevalence of autism in individuals under the age of 18 increased from 3.2 to 12.3 per 10 000 from 2000 to 2007; Chien and colleagues[42]reported that the 12-month prevalence of ASD increased at a rate of 1.8 per 10 000 annually from 1996 to 2005, reaching 28.7 per 10 000 in 2005; and Lai and colleagues[46]reported that from 2004 to 2010 the 12-month prevalence of ASD increased steadily from 8.6 to 20.0 per 10 000.
3.3 Pooled prevalence estimates of autism and ASD from studies in mainland China
The registry-based data from Taiwan and Fong Kong were not suitable for inclusion in the meta-analysis because,unlike the studies from mainland China, there was no screening process used to identify cases. Thus, only the 19 population-based screening and diagnostic studies from mainland China[16,17,19,24-26,29-39,44,45]were considered for the meta-analysis. Fowever, the heterogeneity of these studies was great (I2=94.9%, p<0.001) so we first used sensitivity analysis to identify the causes of heterogeneity prior to pooling the results. Based on these analyses, the 2011 study by Li and colleagues[19]- the largest and only nationwide study (the other studies were conducted in provinces and had much smaller samples) - was excluded because it was the cause of substantial heterogeneity in the estimated prevalence. Aft er excluding this study, the I2for the remaining 18 studies decreased from 94.9% to 76.3%. Using a random-effect model to pool results from the 18 remaining studies (after excluding the study by Li[19]), the pooled sample was 154 473 individuals, and the current prevalence of autism was 12.8 per 10 000 (95%CI,9.4 to 17.5 per 10 000). These results are shown in the Forest plot in Figure 2.
The five studies from mainland China that reported the prevalence of ASD were also quite heterogeneous(I2=94.4%, p<0.001). Fowever, sensitivity analysis did not identify any factors that substantially inf l uenced the heterogeneity of the results (i.e., removal of the identified study with the factor did not result in a substantially reduced I2), so all 5 studies were included in the metaanalysis. Using a random-effect model to pool results from the 5 studies, the pooled sample was 45 694 individuals and the current prevalence of ASD was 24.5 per 10 000 (CI,10.4 to 57.4 per 10 000). These results are shown in the Forest plot in Figure 3.
Among studies in mainland China, one study[17]reported a prevalence of 40.9 per 10 000 for Asperger syndrome; two studies[16,35]reported a prevalence of atypical autism of 0.46 and 8.53 per 10 000, and a prevalence of Rett Syndrome of 0.46 and 1.42 per 10 000;and three studies[17,34,37]reported a prevalence of PDDNOS of between 1.4 and 8.3 per 10 000. Due to the small number of studies for these subtypes of ASD, separate,diagnosis-specific meta-analyses could not be conducted.
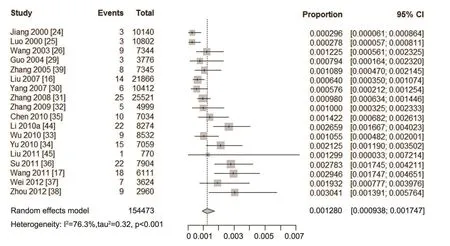
Figure 2. Forest plot of prevalence estimates of autism and 95% confidence intervals from 18 studies in mainland China
?
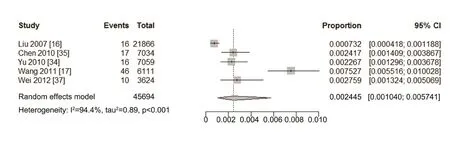
Figure 3. Forest plot of prevalence estimates and 95% confidence intervals from 5 studies of autism spectrum disorders in mainland China
3.4 Study quality and publication bias
Only 8 of the 19 (42%) studies from mainland China[17,26,32,34-36,39,44]considered the influence of nonresponse in the estimation of prevalence and 3 of the 19(16%) studies[37,38,45]did not provide a description of the sampling methods. Based on criteria listed in the STROBE,the quality score of the 19 community-based prevalence studies from mainland China (with a theoretical range of 0 to 22) ranged from 9 to 19 with a mean (sd) of 13.1 (3.2).Four studies[24,30,37,45]with a score of <11 (i.e., less than 50%of the theoretical maximum score) were classified as ‘poor quality’. Of the 22 items from the STROBE assessment, the most common problems were a failure to estimate the required sample size (which was done in only 2 of the 19 reports), and the poor generalizability of the results (which was considered in only 4 of the 19 reports).
A minimum of 10 studies are needed to assess potenti al publicati on bias so it was only possible to conduct this analysis for the 18 studies used to esti mate the prevalence of autism in mainland China and for the subgroup of 13 studies that assessed the prevalence of auti sm using DSN-IV as the diagnostic criteria. The Begg’s funnel plots are shown in Figure 4. Based on the plots,the studies with smaller sample sizes tended to report a higher prevalence of autism. The Z-test for the plot of all 18 studies of the prevalence of auti sm was 2.95 (p=0.003) and that for the 13 studies that used DSN-IV criteria to make the diagnosis of autism was 2.95 (p<0.001); this indicates that publication bias was present in both analyses.
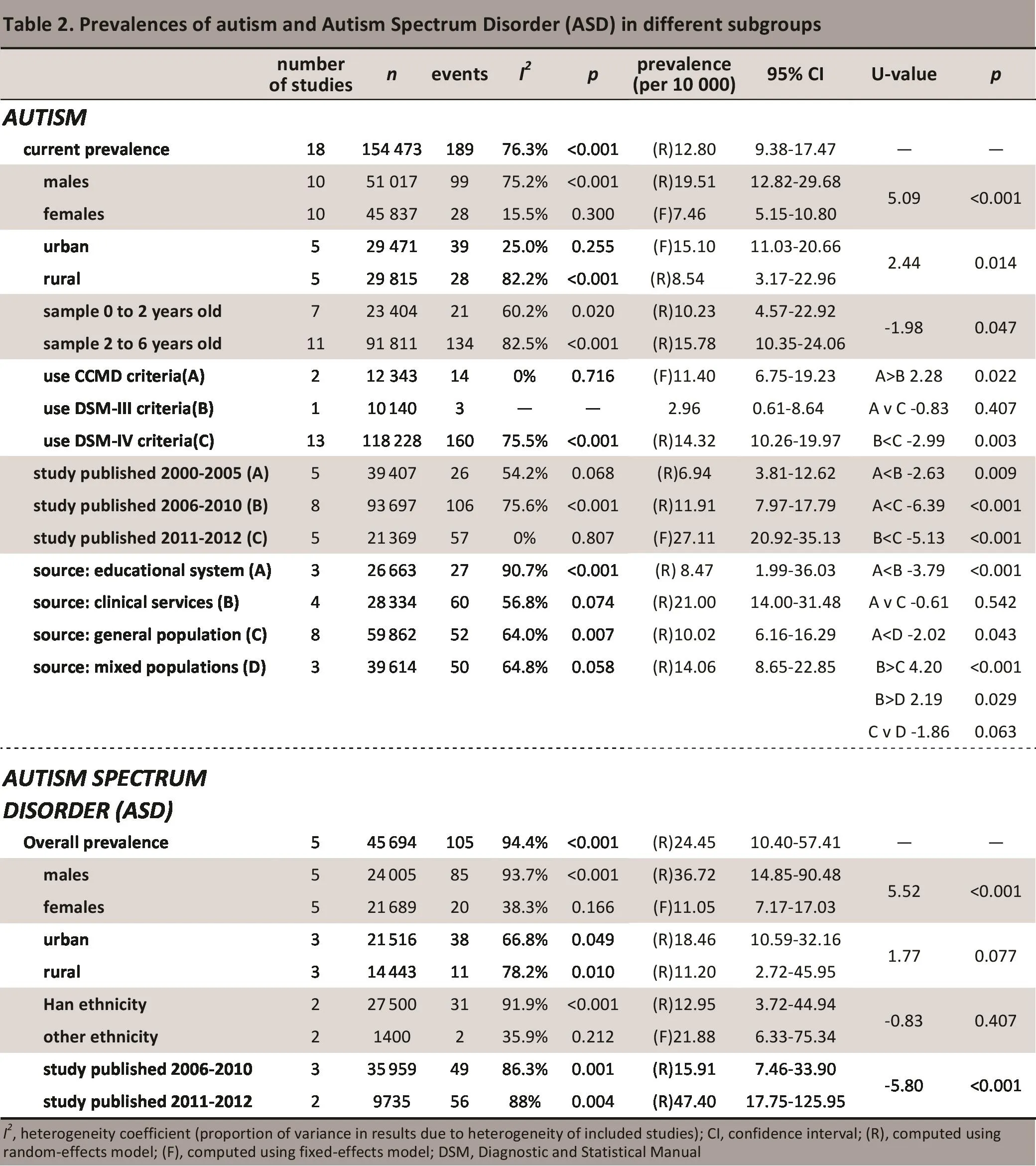
3.5 Prevalences of autism and ASD in mainland China by subgroup
The pooled estimates of the prevalences of autism and ASD in different subgroups of individuals are shown in Table 2. There are significant differences in the estimated prevalence of autism by gender (male prevalence is more than 2-fold female prevalence), residence (urban prevalence is 3-fold rural prevalence), age (children under 2 have a lower prevalence than children 2 to 6 years of age),diagnostic criteria (the prevalence reported in studies using DSN-IV or CCND criteria is much higher than in the single study using DSN-III criteria), year of publication (reported prevalence is higher in more recent publicati ons), and source of population (esti mated prevalence is highest in clinical populations and lowest in samples identified fromschools). The reported prevalence of ASD was also much high in males than in females and higher in more recent publications than in older publicati ons. Fowever, the difference in the urban versus rural prevalence of ASD and the difference in the prevalence of ASD in Fan children versus that in children from other ethnic groups were not statistically significant.
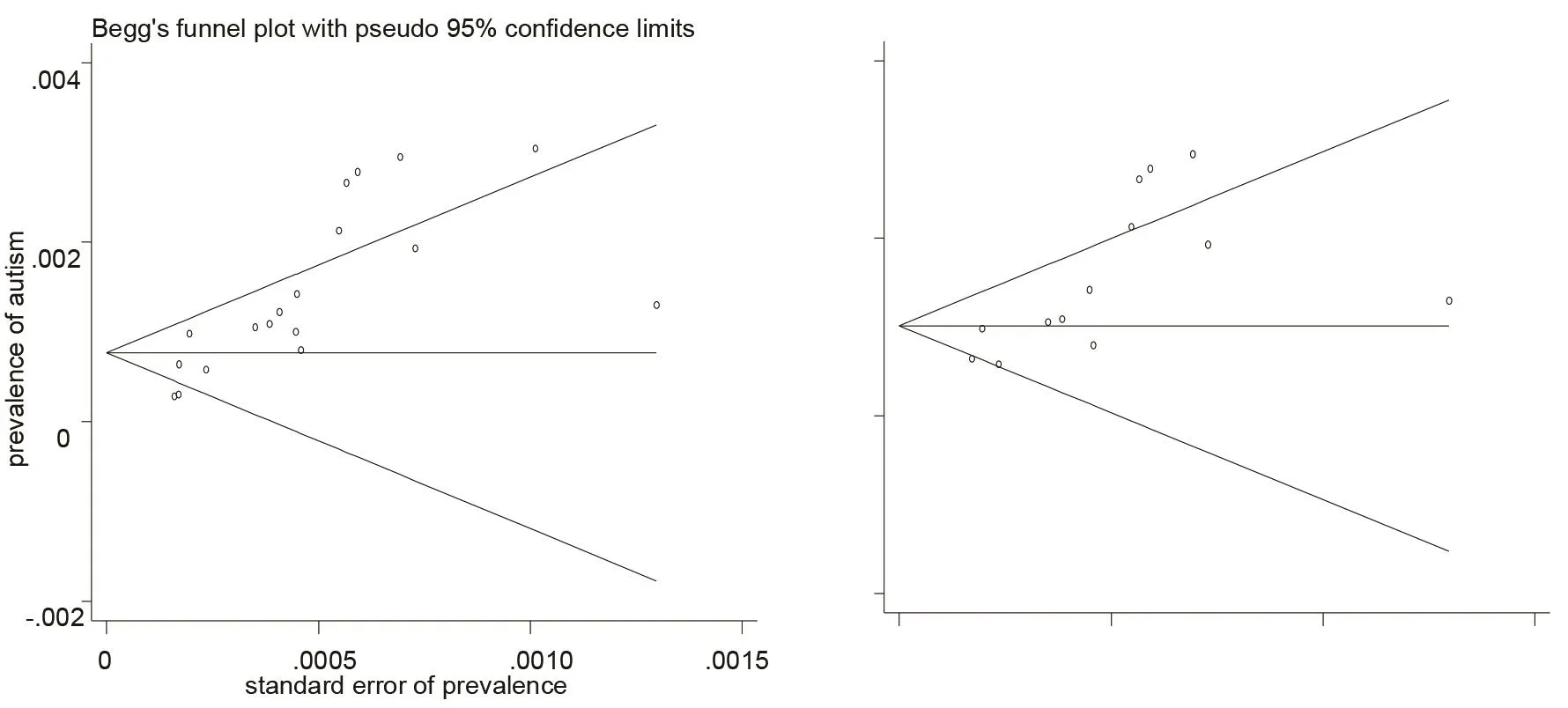
Figure 4. Begg's funnel plots of publication bias for 18 studies of the prevalence of auti sm in mainland China (left 】 and the subgroup of 13 studies that used DSM-IV diagnostic criteria (right】
?
4. Discussion
4.1 Main findings
Based on available registry data from Fong Kong and Taiwan, the reported prevalence of autism over the period from 2000 to 2010 ranged from a low of 1.8 per 10 000 to a high of 424.6 per 10 000, a more than 200-fold difference.Nost of the studies reported increasing rates over ti me, but there must be substantial methodological differences in these studies to result in such a huge range in the estimated prevalence, so it was not possible to pool the results of the registry studies or to integrate them with the communitybased screening and diagnostic studies from mainland China.
The 19 identified studies from mainland China had an estimated prevalence of autism ranging for 2.38 per 10 000 to 30.41 per 10 000, a 13-fold difference. Sensitivity analysis found that by eliminating the study with the lowest prevalence - the large nationwide study - the extremely high heterogeneity of the studies improved substantially (I2decreased from 94.9 to 76.3%), so the meta-analysis only included the remaining 18 studies in which the estimated prevalence of autism ranged from 2.78 per 10 000 to 30.41 per 10 000 (an 11-fold difference). The resulting pooled prevalence of autism from the 18 included studies from mainland China was 12.8 per 10 000 individuals.
Five of these 18 studies also reported the prevalence of ASD in mainland China. The reported prevalence ranged from 7.32 per 10 000 to 75.27 per 10 000, a 10-fold difference. The heterogeneity of these studies was also quite high (I2=94.4%), but sensitivity analysis did not identify factors that could exclude specif i c studies, so all 5 studies were included in the meta-analysis. The pooled prevalence of ASD estimated from these studies was 24.5 per 10 000.
Our estimated prevalences of autism and ASD are substantially lower than the corresponding prevalences reported by most meta-analyses from other countries,[14,15]but some international meta-analyses[13]have reported lower prevalences than those esti mated in this study. There are many possible explanations for these cross-national differences in the reported prevalences of autism and ASD.Nethodological differences - particularly in the source population, in the diagnostic criteria, and in the methods of identifying cases - probably explain the majority of the difference. But there may also be biological and cultural determinants that affect the ‘true’ prevalences of these conditions. Noreover, there appears to be an upward trend in the trajectory of the prevalences of these conditions over ti me that is more than a simple increase in clinical awareness or an increase in care-seeking. If this is the case,it is certainly possible that part of the reason for the lower prevalences in China is that China is at an earlier stage in this trajectory than other regions. Fowever, one major caveat to the suggestion that rates in mainland China are increasing with ti me is that the large nationwide study conducted in 2011 (with a sample several ti mes the combined sample of the remaining 18 studies) had the lowest reported prevalence of autism (2.38 per 1000).
Subgroup differences in the prevalences of autism and ASD found in this study were similar to those reported in other countries. Nale prevalence was three-fold female prevalence, in line with findings from elsewhere.[9,51-53]The prevalences of autism and ASD in urban communiti es was higher than that in rural communities (though the difference was not statistically significant for ASD), a finding that is also reported in high-income countries.[13]Our study found a higher prevalence of autism among children who were 2 to 6 years of age than in younger children; some authors suggest that this may be related to the different clinical manifestations of the condition at different developmental stages during childhood (and the difficulty of establishing the diagnosis at younger ages).[13,54]The one study that used DSN-III criteria to diagnose autism (in 10 140 individuals)had a much lower reported prevalence than the 13 studies that used DSN-IV criteria or the 2 studies that used CCND;these differences may have been related to different characteristi cs of the samples, but other authors have suggested that the use of different diagnostic criteria can result in substantial differenes in the estimated prevalences of these conditions.[10]
4.2 Limitati ons
Our analyses identified several weaknesses in the included studies, so the results need to be interpreted with cauti on.Nany of the included studies were either based in school systems (where rates are much lower) or in clinical populations(where rates are much higher), so their representativeness of the population as a whole is uncertain. The substantial heterogeneity of the results suggests that there were important methodological differences across studies. There was a clear suggestion of publications bias, with smaller studies tending to report higher rates. And the formal assessment of quality of the reports of the study used in the meta-analysis based on the STROBE criteria identified several limitations. Few of the studies reported the prevalences of the subtypes included under the ASD rubric so it was not possible to make robust estimates of the prevalences of these conditions. The huge difference between the rates reported from registry systems (200-fold differences) and the large differences in rates reported from communitybased screening studies (10 to 15-fold differences) indicate that substanti al improvements and standardization of the methodology for estimating the prevalences of these uncommon but serious conditions are needed.
4.3 Significance
Studies from other countries have reported a clear upward trajectory in the prevalences of autism and ASD over ti me.The current systematic review and meta-analysis identified 24 studies published since 2000 that hadesti mated the prevalences of autism or ASD in Chinese children. There were widely varying rates reported in these studies,presumably due to methodological differences across studies, so it is not certain whether or not China is also experiencing the upward trend in the prevalences of autism and ASD reported from high-income countries. There is,however, an increased awareness of the importance of autism since the first reported cases in mainland China in 1982.[56]Improved study methodology is needed to provide valid estimates of the prevalences of these conditions overtime. Unti l these methodological improvements have been made it will not be possible to develop evidence-based prevention and treatment strategies for the management of these seriously disabling conditions.
Conflict of interest
Authors declare no conflict of interest related to this article.
Acknowledgement
Authors would like to thank PhD candidate Yi JIN at the Insti tute of Psychology, Chinese Academy of Sciences for technical support on R soft ware.
Funding
This study is funded by the Research Leadership Development Plan of the city of Shanghai (XBR2011005).
1. Kanner L. Autistic disturbances of affective contact. Nervous Child 1943; 2(3): 217-250.
2. Szatmari P. New recommendati ons on autism spectrum disorder. BMJ 2011; 342:d2456.
3. Chinese Society of Psychiatry. Chinese Classification and Diagnostic Criteria of Mental Disorders, 3rdedition. Jinan:Shandong Science and Technology Publisher; 2001.
4. World Fealth Organizati on. The Internati onal Classification of Diseases (10threvision). Geneva: World Fealth Organizati on; 1992.
5. American Psychiatric Associati on. Diagnosti c and Statistical Manual of Mental Disorders, 4thed. Washington: American Psychiatric Assoati on; 1994.
6. American Psychiatric Association [Internet]. Washington:American Psychiatric Association [updated 2012; cited 2013 Nar 20]. DSN-5 Proposed Criteria for Autism Spectrum Disorder Designed to Provided Nore Accurate Diagnosis and Treatment.Available from: //www.dsm5.org/Documents/12-03%20 Autism%20Spectrum%20Disorders%20-%20 DSN5.pdf.
7. Prevalence of autism spectrum disorders--autism and developmental disabilities monitoring network, 14 sites, United States, 2002. MMWR Surveill Summ 2007; 56(1): 12-28.
8. Prevalence of autism spectrum disorders - Autism and Developmental Disabiliti es Nonitoring Network, United States,2006. MMWR Surveill Summ 2009; 58(10): 1-20.
9. Prevalence of autism spectrum disorders--Autism and Developmental Disabiliti es Nonitoring Network, 14 sites, United States, 2008. MMWR Surveill Summ 2012; 61(3): 1-19.
10. Natson JL, Kozlowski AN. The increasing prevalence of autism spectrum disorders. Res Autism Spectr Disord 2011; 5(1): 418-425.
11. Nanning-Courtney P, Nurray D, Currans K, Johnson F, Bing N,Kroeger-Geoppinger K, et al. Autism spectrum disorders. Curr Probl Pediatr Adolesc Health Care 2013;43(1): 2-11.
12. Feng L, Li C, Chiu F, Lee TS, Spencer ND, Wong JCN. Autism spectrum disorder in Chinese populati ons: a brief review. Asia-Pacif i c Psychiatry 2013 (in press).
13. Williams JG, Figgins JP, Brayne CE. Systematic review of prevalence studies of autism spectrum disorders. Arch Dis Child 2006; 91(1): 8-15.
14. Fombonne E. Epidemiology of pervasive developmental disorders.Pediatr Res 2009; 65(6): 591-598.
15. Elsabbagh N, Divan G, Koh YJ, Kim YS, Kauchali S, Narcin C, et al.Global prevalence of autism and other pervasive developmental disorders. Autism Res 2012;5(3): 160-179.
16. Liu J, Yang X, Jia N, Qu C, Shi J, Liu G, et al. A cross-secti onal study of pervasive developmental disorders among children 2-6 years of age in Beijing, 2004. Chinese Mental Health Journal,2007;21(5): 290-293.
17. Wang X, Yang W, Jin Y, Jing J, Fuang X, Li X, et al. A study on the prevalence of autism spectrum disorders and associated factors in kinder gardens in Guangzhou. Chinese Mental Health Journal.2011; 25(6): 401-408.
18. Yu R, Lin L, Xu D, Li X, Qiu F. An analysis of prevalence of autism in Chinese children. Maternal and Child Health Care in China 2011;26(29): 4563-4565.
19. Li N, Chen G, Song XN, Du W, Zheng XY. Prevalence of auti smcaused disability among Chinese children: A nati onal populati onbased survey. Epilepsy Behav 2011;22(4): 786-789.
20. Wang J, Wang B. Clincial epidemiology, 3rd edition.Beijing:People’s Nedical Publishing Fouse,2002:14.
21. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC,Nulrow CD, Pocock SJ, et al. Strengthening the Reporti ng of Observati onal Studies in Epidemiology (STROBE): Explanati on and Elaborati on. Epidemiology 2007;18(6): 805-835 10.1097/EDE.0b013e3181577511.
22. Figgins J, Thompson SG, Deeks JJ, Altman DG. Neasuring inconsistency in meta-analyses. BMJ 2003;327(7414): 557-560.
23. Fang J, Lu Y. Nodern medical stati sti cs. Beijing: People’s Nedical Publishing Fouse,2002:202-204.
24. Jiang L, Li R, Li Y, LiY, Li F. A health survey of child mental health in Luoyang. Journal of psychological health 2000; 8(1): 27-28.
25. Luo W, Lin L, Chen R, Cheng W, Fuang Y, Fu T, et al. An epidemiological survey of auti sm in Fujian province. Shanghai Archives of Psychiatry 2000;12(1): 3-5.
26. Wang W, Zhai L, Zheng L, Zhu J, Qu X, Feng Q, et al. An epidemiological survey of auti sm in Jiangsu province. China Behavioral Science 2003;12(2): 173-174.
27. Guo R. An epidemiological study of auti sm in 5000 children aged 0-6 years in Tianjin. China Clinical Rehabilitati on 2004;8(6):1122-1123.
28. Zhang X, Ji C, Li J, Sun J. A survey of autism among children 2-6 years old in Tianjin. Chinese Journal of Reproductive Health 2004;15(4): 206-208.
29. Guo C. An epidemiological survey of psychiatric disability among children 2-6 years of age in Dingxi county. China Rehabilitation Theory and Practice. 2004;10(2): 118-119.
30. Yang S, Fu Y, Fan Y. An epidemiological analysis of autism.Practical Pediatrics 2007; 22 (24): 1872-1873.
31. Zhang F, Gui Q, Wang J, Xue S, Lu X, Na X, et al. A cross-sectional study of autism among children 1-6 years of age in the city of Wuxi. China Women and Children’s Fealth.Maternal and Child Health Care in China 2008;23(27): 3979-3980.
32. Zhang G, Xu Y, Fuang C, Yang F, Lu Y. An epidemiolgoical survey of autism in the Yunyan district of Guiyang city. Journal of Guiyang Medical College 2009;34(4): 463+465.
33. Wu X, Lu Y, Wang Y, Zheng Q, Wang T, Lin J, et al. A prevalence survey of autism in infants and children in Lianyungang city.Journal of Modern Medicine and Health 2010;24(24): 3724-3276.
34. Yu C, Xia W, Sun C, Zhou Y, Liu L, Li J, et al. A cross-sectional survey of autism spectrum disorders among children 2-6 years old in Farbin city. Chinese Journal of Child Health Care 2010;18(10):750-753.
35. Chen Y, Fuang F, Zhao Y, Li D, Li J, Yao L, et al. An epidemiological survey of autism spectrum disorders in children 2-6 years old in Ranghulu district of Daqing city. Chinese Journal of Child Health Care 2010;18(4): 331-333.
36. Su Y, Zhang X, Li A, Li Y, Liu G. Prevalence of autism and associated factors in infants and children in Tianjin. Maternal and Child Health Care in China 2011;26(32): 5004-5007.
37. Wei Q, Ren L, Wong L, Gao W, Fe F, Wang W, et al. The screening and 3-year follow-up study of autism spectrum disorder among infants 18-24 months old in Shenzhen city. Chinese Journal of Child Health Care 2012;20(4): 354-357.
38. Zhou L, Shi J. A clincial diagnostic analysis of infant and child autism. China Modern Doctor 2012;50(17): 50-51.
39. Zhang X, Ji CY. Autism and mental retardation of young children in China. Biomed Environ SCI 2005;18(5): 334-340.
40. Wong VC, Fui SL. Epidemiological study of autism spectrum disorder in China. J Child Neurol 2008;23(1): 67-72.
41. Lin JD, Lin LP, Wu JL. Administrative Prevalence of autism spectrum disorders based on national disability registers in Taiwan. Res Autism Spectr Disord 2009;3(1): 269-274.
42. Chien IC, Lin CF, Chou YJ, Chou P. Prevalence and inCIdence of autism spectrum disorders among national health insurance enrollees in Taiwan from 1996 to 2005. J Child Neurol 2011;26(7):830-834.
43. Fsu SW, Chiang PF, Lin LP, Lin JD. Disparity in autism spectrum disorder prevalence among Taiwan National Fealth Insurance enrollees: Age, gender and urbanization effects. Res Autism Spectr Disord 2012; 6(2): 836-841.
44. Li A. A cross-sectional study of autism and early presentations among children 1.5-3 years old in Tianjin. Tianjin: Tianjin Nedical College, Naster thesis,2010.
45. Liu J. Early screening and a clincial record study of autism spectrum disorder. Shanghai: Fudan University, Naster thesis,2011.
46. Lai DC, Tseng YC, Fou YN, Guo FR. Gender and geographic differences in the prevalence of autism spectrum disorders in children: analysis of data from the national disability registry of Taiwan. Res Dev Disabil 2012; 33(3): 909-915.
47. Wang W, Zhai L, Zheng L, Qu X, Feng Q, Sun W, et al. An epidemiological study of autism in Changzhou city. Journal of Clinical Psychiatry 2002;12(3): 148-149.
48. Fuang F. An epidemiological survey of autism spectrum disorders in children 2-6 years old in Ranghulu district of Daqing city. Feilongjiang: China Nedical University, Naster thesis, 2010.
49. Li A. An analysis of autism behavior among children 1.5-3 years old in Tianjin. Chinese Journal of Mental Health 2010;24(3): 215-218.
50. Wang Y, Lu Y, Wu X, Chen J, Zheng Q. Eearly diagnosis and recognition of child autism spectrum disorders. Maternal and Child Health Care in China 2012;27(27): 4236-4238.
51. Samadi SA, Nahmoodizadeh A, NcConkey R. A national study of the prevalence of autism among fi ve-year-old children in Iran.Autism 2012;16(1): 5-14.
52. Bertrand J, Nars A, Boyle C, Bove F, Yeargin-Allsopp N, Decouf l e P. Prevalence of autism in a United States population: the Brick Township, New Jersey, investigation. Pediatrics 2001;108(5):1155-1161.
53. Fombonne E. Epidemiological surveys of autism and other pervasive developmental disorders: an update. J Autism Dev Disord 2003;33(4): 365-382.
54. Fertz-PicCIotto I, Delwiche L. The rise in autism and the role of age at diagnosis.Epidemiology 2009;20(1): 84-90.
55. Perkins EA,Berkman, KA.Into the unknown: aging with autism spectrum disorders. Am J Intellect Dev Disabil 2012;117(6):478-496.
56. Tao G. Diagnosis and categorization of infant autism. Chin J Nerv Ment Dis 1982;15(2):104-107. (In Chinese)
中国儿童孤独症谱系障碍患病率的系统综述
万玉美1胡强1李婷1姜丽娟1杜亚松1Lei FENG2John Chee-Meng WONG2,3李春波1*
背景中国孤独症和孤独症谱系障碍(autism spectrum disorders, ASD)的患病率缺乏可靠的估计。目的运用Meta分析综合评价中国18岁以下人群孤独症和ASD患病情况,并分析其在性别、民族、城乡等不同因素间的差异。方法检索中国知识资源总库、中国科技期刊数据库、万方数据检索系统、中国生物医学文摘数据库、PubMed和Web of Science等数据库,收集关于中国孤独症谱系障碍患病率的文献,按照预先制定的纳入及排除标准筛选相关研究。采用R-2.15.2软件对资料进行统计学分析。结果共纳入24项研究,其中5项来自香港和台湾的注册研究(涉及14,570,369名儿童),19项来自大陆以人群为基础的筛查和诊断研究(合并样本量为771,413名儿童)。港台注册研究报道的孤独症年患病率为1.8~424.6/10,000。中国大陆的18项研究(剔除一个患病率最低的全国性研究)报道孤独症患病率为2.8~30.4/10,000,合并后孤独症患病率为12.8/10,000(95%CI,9.4~17.5)。5项研究报道ASD(患病率为7.3~75.3/10,000)合并后患病率24.5/10,000(95%CI,10.4~57.4)。不同性别、居住地点、发表时间和抽样来源之间报道的患病率存在明显差异。结论港台注册研究报道的孤独症患病率存着巨大差异(达200倍),大陆以人群为基础的筛查诊断研究报道的患病率存在较大差异(10~15倍),凸显迫切需要建立标准的方法来估计孤独症和ASD的患病率。只有方法学质量得到改善,才有可能为这些不常见但严重致残的疾病提供循证的防治策略。
Background:There are no reliable esti mates of the prevalences of autism and autism spectrum disorders (ASD)in China.Objecti ve:Combine results across studies to esti mate the prevalences of autism and ASD among Chinese children under the age of 18, and assess variati ons in the prevalences with respect to gender, ethnicity, and urban versus rural residence.Methods:Based on pre-defined inclusion and exclusion criteria, studies were identified by searching the following databases: Chinese National Knowledge Infrastructure, Chongqing VIP database for Chinese Technical Periodicals, WANFANG DATA, Chinese Biological Nedical Literature Database, Pubmed, and Web of Science.Statistical analysis was conducted using R-2.15.2 soft ware.Results: The 24 studies meeting inclusion criteria included 5 registry studies from Taiwan and Fong Kong(covering a total of 14 570 369 children) and 19 community-based screening and diagnostic studies from mainland China (with a combined sample of 771 413 children). The annually reported prevalence of autism in the registry studies ranged from 1.8 to 424.6 per 10 000. A meta-analysis of 18 of the studies from mainland China(excluding a large nationwide study with the lowest prevalence of auti sm) with a range in rates from 2.8 to 30.4 per 10 000 generated an estimated pooled prevalence of autism of 12.8 per 10 000 (95%CI, 9.4 to 17.5).The pooled prevalence of ASD estimated from 5 of these studies (which had a range in rates from 7.3 to 75.3 per 10 000) was 24.5 per 10 000 (95%CI, 10.4 to 57.4). The reported prevalence of autism varied substanti ally by gender, location of residence, date of publicati on, and source of the sample.Conclusion:The huge difference between the rates for autism reported from registry systems in Fong Kong and Taiwan (a 200-fold difference) and the large differences in rates reported from community-based screening studies in mainland China (a 10- to 15-fold difference) highlight the urgent need for establishing standardized methods for estimating the prevalences of autism and ASD. Until these methodological improvements have been made, it will not be possible to develop evidence-based prevention and treatment strategies for the management of these uncommon but seriously disabling conditions.
10.3969/j.issn.1002-0829.2013.02.003
1Shanghai Nental Fealth Center, Shanghai Jiao Tong University School of Nedicine, Shanghai, China
2Department of Psychological Nedicine, Yong Loo Lin School of Nedicine, Nati onal University of Singapore, Singapore
3Department of Psychological Nedicine, Nati onal University Fospital, Singapore
correspondence: chunbo-li@yahoo.com

Yumei Wan graduated with a Bachelor of Medicine from Jining Medical University in Shandong Province in 2011. She is currently a master degree student in psychiatry at the Shanghai Jiao Tong University School of Medicine. Her research interests are the evaluation of clinical guidelines of mental disorders and the conduct of systematic reviews.
1上海交通大学医学院附属精神卫生中心 上海
2Department of Psychological Medicine, Yong Loo Lin School of Medicine, National University of Singapore,Singapore
3Department of Psychological Medicine, National University Hospital, Singapore
*通信作者:chunbo_li@yahoo.com
猜你喜欢
电气自动化(2022年2期)2023-01-07
艺术品鉴(2022年16期)2022-07-09
河池学院学报(2021年1期)2021-07-10
景德镇陶瓷(2021年1期)2021-03-24
新世纪智能(英语备考)(2019年4期)2019-06-26
东方考古(2017年0期)2017-07-11
台商(2017年1期)2017-03-01
人民交通(2012年6期)2012-10-26
当代外语研究(2010年1期)2010-03-20
- 上海精神医学的其它文章
- Comorbidity of mental and physical diseases: a main challenge for medicine of the 21st century
- Neuroimaging studies in pati ents with obsessive-compulsive disorder in China
- Methodology of China's nati onal study on the evaluati on,early recogniti on, and treatment of psychological problems in the elderly: the China Longitudinal Aging Study (CLAS】
- Relationship of changes in cognitive and depressive symptoms during anti depressant treatment of individuals with geriatric depression and their relationship to the APOE epsilon 4 allele
- Effi cacy and safety of generic escitalopram versus Lexapro in the treatment of major depression: a multi center doubleblinded randomized controlled trial
- Pesticides availability and medically serious suicide attempts in China