
英夫利西降阶梯治疗中重度溃疡性结肠炎的疗效分析
2016-08-07 13:53谭晓燕毛靖伟王英德
胃肠病学和肝病学杂志 2016年3期
谭晓燕, 毛靖伟, 王英德
大连医科大学附属第一医院消化内科,辽宁 大连 116033
英夫利西降阶梯治疗中重度溃疡性结肠炎的疗效分析
谭晓燕, 毛靖伟, 王英德
大连医科大学附属第一医院消化内科,辽宁 大连 116033
目的 探讨英夫利西(infliximab,IFX)降阶梯治疗中重度溃疡性结肠炎(ulcerative colitis,UC)的有效性。方法 收集初始应用IFX治疗的中重度UC患者14例,分别在第0周(治疗前)、2周、6周、14周、22周及30周对其临床资料进行回顾性分析。结果 14例UC中9例完成30周随访。有效率:2周为85.71%(12/14),6周为92.31%(12/13),14周为100%(12/12),22周为81.82%(9/11),30周为100%(9/9)。临床缓解率:2周为0(0/14),6周为23.08%(3/13),14周为66.67%(8/12),22周为63.64%(7/11),30周为88.89%(8/9)。白蛋白(albumin,ALB)和C-反应蛋白(C-reactive protein,CRP)水平在2周、6周、14周、22周及30周与治疗前比较,差异有统计学意义(P<0.05)。结论 IFX降阶梯治疗中重度UC疗效好,ALB和CRP水平可以作为评估IFX疗效的参考指标。
英夫利西;溃疡性结肠炎;疗效;安全性
溃疡性结肠炎(ulcerative colitis,UC)是一种以结肠黏膜连续性、弥漫性炎症改变为特点的慢性非特异肠道炎症性疾病。我国发病率有逐年上升趋势,且病变范围较前更为广泛,中重度UC发病率增高。2012年广州共识意见[1]指出英夫利西(infliximab,IFX)诱导中重度UC缓解有效,但我国在此方面的研究尚处于初步阶段。本文拟探讨IFX降阶梯治疗中重度UC的疗效和安全性,为UC的生物治疗方案提供一定的帮助。
1 资料与方法
1.1 一般资料 收集大连医科大学附属第一医院消化内科2013年1月-2015年5月初始应用IFX治疗的中重度UC患者14例。入选标准:确诊为中重度UC的18~70岁患者,至少应用3次IFX治疗。排除标准:(1)应用糖皮质激素及免疫抑制剂;(2)年龄<18岁或>70岁;(3)有药物过敏史;(4)感染性疾病(包括肺结核、病毒性肝炎或其他潜在感染);(5)器质性心肺疾病、糖尿病、恶性肿瘤等;(6)妊娠期患者。接受IFX治疗前,签署知情同意书。病变范围分类采用蒙特利尔分类,活动分度采用改良Mayo评分系统[1]。
1.2 治疗方法 在第0周、2周、6周分别给予剂量为5 mg/kg的IFX静脉滴注(每次时间不少于2 h)作为诱导缓解治疗,之后每隔8周给予相同剂量的维持治疗,每次输注过程中及结束后观察有无不良反应并记录。
1.3 疗效判定 以用药第0周、2周、6周、14周、22周、30周为观察时间点。(1)有效:Mayo评分相对于基线值的降幅≥30%及≥3分,且便血的分项评分降幅≥1分或该分项评分为0分或1分;(2)临床缓解:评分≤2分,且无单个分项评分>1分;(3)复发:疾病由缓解期进入活动期,活动期定义为Mayo评分≥2分;(4)黏膜愈合:随访患者,内镜分项评分均为0或1分;(5)无应答:临床症状、结肠镜复查均无改善。
1.4 不良事件 如实填写不良事件记录表,记录不良事件的发生时间、严重程度、持续时间、采取的措施和转归。

2 结果
2.1 一般情况 14例UC中男女各7例,第一次输注IFX的平均年龄为(44.14±1.40)岁,病程2周~20年;病变范围E1 1例(7.14%),E2 5例(35.71%),E3 8例(57.14%);严重程度:中度 3例(21.43%),重度11例(78.57%);基础Mayo评分为11.07±0.83;有肠外表现3例(21.43%),合并银屑病1例(7.14%)。
2.2 疗效 14例UC患者中有9例患者完成30周随访。总有效率:2周为85.71%(12/14),6周为92.31%(12/13),14周为100%(12/12),22周为81.82%(9/11),30周为100%(9/9)。临床缓解率:2周为0(0/14),6周为23.08%(3/13),14周为66.67%(8/12),22周为63.64%(7/11),30周为88.89%(8/9)。22周时有18.19%(2/11)复发。复查肠镜:6周为2例(15.38%,2/13);14周为3例(25.0%,3/12),其中2例达到黏膜愈合;22周为3例(27.27%,3/11),其中1例达到黏膜愈合;30周为2例(22.22%,2/9),其中1例达到黏膜愈合。
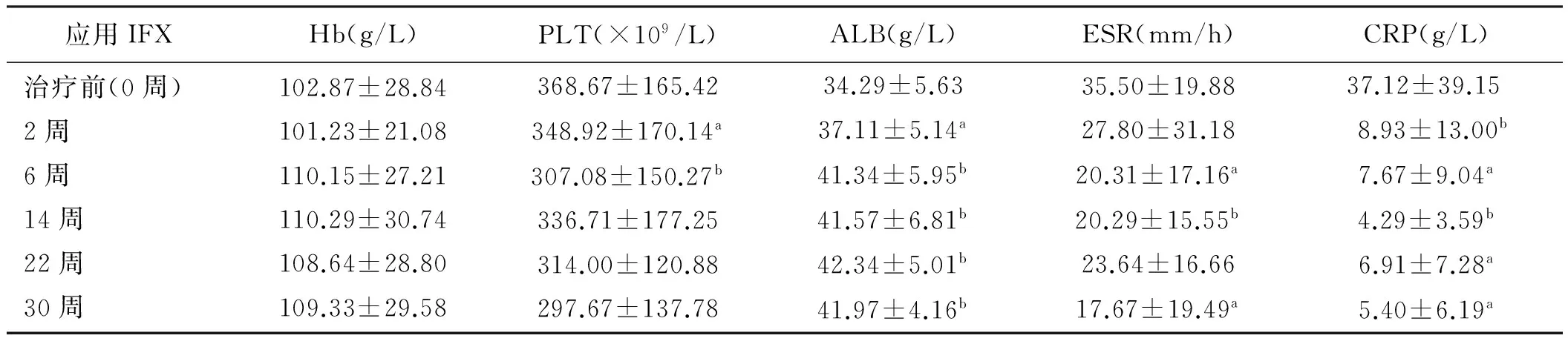
2.3 实验室检查 治疗前,平均Hb为(127.99±26.97)g/L,平均PLT计数为(368.67±162.42)×109/L,平均ALB为(34.29±5.63)g/L,平均ESR为(35.5±19.88)mm/h,平均CPR为(37.12±39.15)g/L。血中ALB和CRP水平在2周、6周、14周、22周及30周与治疗前比较,差异有统计学意义(P<0.05,见表1)。

应用IFXHb(g/L)PLT(×109/L)ALB(g/L)ESR(mm/h)CRP(g/L)治疗前(0周)2周6周14周22周30周102.87±28.84101.23±21.08110.15±27.21110.29±30.74108.64±28.80109.33±29.58368.67±165.42348.92±170.14a307.08±150.27b336.71±177.25314.00±120.88297.67±137.7834.29±5.6337.11±5.14a41.34±5.95b41.57±6.81b42.34±5.01b41.97±4.16b35.50±19.8827.80±31.1820.31±17.16a20.29±15.55b23.64±16.6617.67±19.49a37.12±39.158.93±13.00b7.67±9.04a4.29±3.59b6.91±7.28a5.40±6.19a
注:与治疗前比较,aP<0.05, bP<0.01。
2.4 不良事件 共有28.57%(4/14)发生不良事件。1例为带状疱疹,抗病毒治疗后好转,3例均为过敏反应,1例改用阿达木单抗治疗,2例均改用5-ASA维持治疗。
3 讨论
UC是一种慢性反复发作性疾病,近年来其发病率呈上升趋势,可能与人们生活方式变化、城市环境改变等有关[2]。传统治疗药物有:氨基水杨酸制剂、糖皮质激素和免疫抑制剂等。但糖皮质激素和免疫抑制剂长期应用会导致继发的健康问题,部分激素耐药或抵抗的难治性患者效果更不理想。IFX为肿瘤坏死因子-α(tumor necrosis factor-alpha,TNF-α)单抗,通过与多种免疫反应细胞中的促炎因子TNF-α结合,封闭其促炎效应,并促进炎性细胞凋亡,发挥抗炎作用[3]。研究表明,IFX能诱导UC患者临床症状缓解,提高黏膜愈合率并维持长期缓解[4-6]。
本研究中,应用IFX治疗有效率与缓解率均呈上升趋势。ACT 1和ACT 2的研究显示[7],应用IFX治疗 8周有效率为65%和67%,缓解率为35%和31%,在30周时将近有50%仍能维持缓解。开放性试验表明[8],应用IFX治疗中重度UC在第8周的有效率为60%~100%,临床缓解率为40%~100%。本研究显示应用IFX早期应答率及维持缓解率均较高,考虑与“降阶梯”治疗有关。另外治疗过程中共有5例患者中途退出,1例因过敏改用了阿达木单抗,其余4例分别因无反应、过敏、复发等中途退出,余患者应答率较高,这也是维持缓解率高的原因之一。另外,多数患者难以忍受肠镜检查,肠镜复查率低,造成黏膜愈合率不高。
炎症性肠病的治疗分为“升阶梯”和“降阶梯”2种方案。早在2000年,IFX的降阶梯治疗就在类风湿性关节炎的患者中使用,初始应用IFX,能使类风湿性关节炎的疾病活动指数迅速下降,减缓关节的受损程度[9]。D’Haens等[10]研究表明,降阶梯治疗CD诱导缓解后复发的中位时间更长,黏膜愈合率更高,并能减少住院率和手术风险。还有研究表明[11],初始应用IFX诱导缓解的CD患者,维持缓解率高,可以改变疾病的自然病程。但降阶梯治疗存在限制:(1)过度治疗[12];(2)缺乏血清学和基因学的检测指标来预测疾病的自然病程[13];(3)缺乏强有力的大样本循证医学证据;(4)长期的药物安全性问题:如机会感染、恶性肿瘤、脱髓鞘病变、自身免疫性疾病及加重心力衰竭等[14];(5)医疗费用问题。
近年,很多学者致力于预测IFX疗效指标的研究,例如IFX的血药浓度、谷浓度、抗抗体及基因检测等。研究表明,基础Mayo评分≥11,应用时年龄越小,基础CRP>3 mg/dl,预示IFX的有效率越高[15-16]。Tursi等[17]研究表明,基础Hb<115 g/L以及24周的黏膜愈合率与IFX疗效有关。本研究结果与其一致。另外,治疗后ALB和CRP水平均较治疗前有明显改善,与Armuzzi等[18]和我们之前的研究[19]结果一致。
总之,IFX降阶梯治疗中重度UC疗效确切,有效率及临床缓解率高,ALB和CRP可以作为评估IFX疗效的参考指标。降阶梯治疗有其自身的优点,但目前仍有很多问题尚待解决。本研究为回顾性研究,样本量小,缺乏长期随访,所得的结论尚需更大规模的多中心随机对照研究进一步证实。
[1]Digestive Disease Branch of Inflammatory Bowel Disease Study Group of the Chinese Medical Association. The consensus on the diagnosis and treatment of inflammatory bowel disease [J]. Chin J Gastroenterol, 2012, 17(12): 763-781. 中华医学会消化病学分会炎症性肠病学组. 炎症性肠病诊断与治疗的共识意见 (2012年. 广州) [J]. 胃肠病学, 2012, 17(12): 763-781.
[2]Jowett SL, Seal CJ, Pearce MS, et al. Influence of dietary factors on the clinical course of ulcerative colitis: a prospective cohort study [J]. Gut, 2004, 53 (10): 1479-1484.
[3]Ming L, Zhang SM. Biologics applied to inflammatory bowel disease [J]. Chin J Gastroenterol Hepatol, 2015, 24(9): 1047-1049. 明兰, 张苏闽. 生物制剂介入治疗炎症性肠病 [J]. 胃肠病学和肝病学杂志, 2015, 24(9): 1047-1049.
[4]Van Assche G, Dignass A, Bokemeyer B, et al. Second European evidence based consensus on the diagnosis and management of ulcerative colitis part 3: special situations [J]. J Crohns Colitis, 2013, 7(1): 1-33.
[5]Stidham RW, Lee TC, Higgins PD, et al. Systematic review with network meta-analysis: the efficacy of anti-tumour necrosis factor-alpha agents for the treatment of ulcerative colitis [J]. Aliment Pharmacol Ther, 2014, 39(7): 660-671.
[6]Danese S, Fiorino G, Peyrin-Biroulet L, et al. Biological agents for moderately to severely active ulcerative colitis: a systematic review and network meta-analysis [J]. Ann Intern Med, 2014, 160(10): 704-711.
[7]Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis [J]. N Engl J Med, 2005, 353(23): 2462-2476.
[8]Juliao F, Marquez J, Aristizabal N, et al. Clinical efficacy of infliximab in moderate to severe ulcerative colitis in a latin American referral population [J]. Digestion, 2013, 88(4): 222-228.
[9]St Clair EW, van der Heijde DM, Smolen JS, et al. Combination of infliximab and methotrexate therapy for early active rheumatoid arthritis: a randomized, controlled trial [J]. Arthritis Rheum, 2004, 50(11): 3423-3443.
[10]D’Haens G, Baert F, van Assche G, et al. Early combined immunosuppression or conventional management in patients with newly diagnosed Crohn’s disease: an open randomised trial [J]. Lancet, 2008, 371(9613): 660-667.
[11]Kugathasan S, Werlin SL, Martinez A, et al. Prolonged duration of response to infliximab in early but not late pediatric Crohn’s disease [J]. Am J Gastroenterol, 2000, 95(11): 3189-3194.
[12]Baert F, Caprilli R, Angelucci E. Medical therapy for Crohn’s disease: top-down or step-up? [J]. Dig Dis, 2007, 25(3): 260-266.
[13]Ricart E, García-Bosch O, Ordás I, et al. Are we giving biologics too late? The case for early versus late use [J]. World J Gastroenterol, 2008, 14(36): 5523-5527.
[14]Nielsen OH, Ainsworth MA. Tumor necrosis factor inhibitors for inflammatory bowel disease [J]. N Engl J Med, 2013, 369(26): 754-762.
[15]Park SH, Yang SK, Hong SM, et al. Severe disease activity and cytomegalovirus colitis are predictive of a nonresponse to infliximab in patients with ulcerative colitis [J]. Dig Dis Sci, 2013, 58(12): 3592-3599.
[16]Lee KM, Jeen YT, Cho JY, et al. Efficacy, safety, and predictors of response to infliximab therapy for ulcerative colitis: a Korean multicenter retrospective study [J]. J Gastroenterol Hepatol, 2013, 28(12): 1829-1833.
[17]Tursi A, Elisei W, Picchio M, et al. Managing ambulatory ulcerative colitis patients with infliximab: A long-term follow-up study in primary gastroenterology centers [J]. Eur J Intern Med, 2014, 25(8): 757-761.
[18]Armuzzi A, Pugliese D, Danese S, et al. Infliximab in steroid-dependent ulcerative colitis: effectiveness and predictors of clinical and endoscopic remission [J]. Inflamm Bowel Dis, 2013, 19(5): 1065-1072.
[19]Tan XY, Mao JW, Wang YD. Retrospective analysis of 115 cases of ulcerative colitis [J]. World Chinese Journal of Digestology, 2014, 22(33): 5188-5192. 谭晓燕,毛靖伟,王英德. 回顾性分析溃疡性结肠炎115例 [J]. 世界华人消化杂志, 2014, 22(33): 5188-5192.
(责任编辑:陈香宇)
Efficacy of top-down therapy of infliximab in patients with moderate to severe ulcerative colitis
TAN Xiaoyan, MAO Jingwei, WANG Yingde
Department of Gastroenterology, the First Affiliated Hospital of Dalian Medical University, Dalian 116033, China
Objective To evaluate the efficacy of top-down trerapy of infliximab (IFX) in patients with moderate to severe ulcerative colitis (UC). Methods Medical records of 14 patients with moderate to severe UC who
IFX treatment were reviewed retrospectively. Results Nine cases of 14 UC patients were completed 30 weeks follow-up. The clinical response and remission rates were 85.71% (12/14) and 0(0/14) at 2nd week, 92.31%(12/13) and 23.08%(3/13) at 6th week, 100%(12/12) and 66.67%(8/12) at 14th week, 81.82%(9/11) and 63.64%(7/11) at 22th week, 100%(9/9) and 88.89%(8/9) at 30th week. The levels of serum albumin (ALB) and C-reactive protein (CRP) were statistically significant after IFX treatment (P<0.05). Conclusion IFX with top-down strategies is effective in treating patients with active moderate to severe UC. ALB and CRP can be used as markers to assess the efficacy of IFX.
Infliximab; Ulcerative colitis; Efficacy; Safety
10.3969/j.issn.1006-5709.2016.03.015
谭晓燕,在读博士,主治医师,研究方向:胃肠道疾病的诊治。E-mail: quan82_1019@126.com
王英德,硕士,主任医师,教授,硕士生导师,研究方向:炎症性肠病和自身免疫性肝病。E-mail: albertwyd@163.com
R574.62
A
1006-5709(2016)03-0291-03
2015-07-01
猜你喜欢
中老年保健(2021年8期)2021-12-02
中老年保健(2021年8期)2021-08-24
中华养生保健(2020年2期)2020-11-16
医学新知(2019年4期)2020-01-02
医学新知(2019年4期)2020-01-02
云南医药(2019年3期)2019-07-25
人大建设(2017年12期)2017-08-15
幸福(2016年9期)2016-12-01
学苑创造·B版(2016年4期)2016-04-14
中国医药科学(2015年15期)2015-02-27
