
孟鲁斯特/氯雷他定联合疗法对变应性鼻炎的荟萃分析
2017-04-06 03:53黄鑫梅张艳慧郑沙盟
浙江实用医学 2017年1期
黄鑫梅,张艳慧,郑沙盟
(1.金华市中医医院,浙江 金华 321017;2.浙江省中医院,浙江 杭州 310006)
·综述·
孟鲁斯特/氯雷他定联合疗法对变应性鼻炎的荟萃分析
黄鑫梅1,张艳慧1,郑沙盟2
(1.金华市中医医院,浙江 金华 321017;2.浙江省中医院,浙江 杭州 310006)
孟鲁司特/氯雷他定(montelukast/loratadine,M/L)联合疗法已被广泛用来改善变应性鼻炎患者的临床症状,但是M/L联合疗法是否优于单药疗法仍存在争论。本文采用荟萃分析评价M/L联合疗法是否优于单药疗法,并从鼻部症状评分,生活质量问卷评分,夜间症状评分三方面进行分析,结果发现在改善鼻部症状方面,M/L联合疗法优于孟鲁司特或氯雷他定单药疗法,但是在改善生活质量和夜间症状方面,M/L联合疗法是否优于单药治疗需进一步研究证实。
孟鲁斯特;氯雷他定;变应性鼻炎;荟萃分析
变应性鼻炎(allergic rhinitis,AR)是一种由过敏原引起的鼻黏膜炎症的常见疾病[1],可以引起患者鼻塞、流涕、瘙痒等,严重降低患者生活质量。目前治疗AR的方案较多,临床研究已证实,第二代抗组胺药与白三烯受体阻断剂可显著改善AR患者的临床症状,但仍有部分患者病情难以控制,临床上为了更好地控制AR症状,常采取联合用药,其中孟鲁斯特与氯雷他定是常用的联合疗法之一。从理论上,孟鲁司特/氯雷他定(montelukast/ loratadine,M/L)联合使用效果可能优于单药使用,已有较多研究评价M/L联合疗法与单药疗法的疗效,但是结论仍然未达成一致。本文拟采用荟萃分析,综合比较M/L联合疗法与单药疗法在AR患者中的疗效,以期为临床用药策略提供参考。
1 资料与方法
1.1 文献来源 本文检索了Cochrane数据库,MEDLINE和EMBASE数据库,采用以下检索词:rhinitis,allergic,montelukast,loratadine,检索截止日期为2016年9月30日,所有关于M/L联合疗法治疗AR的研究均纳入初步检索范围,并且手工检索了纳入研究的参考文献以避免遗漏。研究纳入标准:(1)随机对照研究;(2)干预方式:M/L联合疗法与单药治疗的比较;(3)结果:鼻部症状评分(Total nasal symptom score,TNSS),生活质量问卷评分 (Rhinoconjunctivitis Quality of Life Questionnaire,RQLQ),夜间症状评分(Nighttime Symptom Score,NSS),如数据缺失,则联系相关作者获取数据,但仅成功获取1项研究的缺失数据;(4)因中文文献相关研究报道不多,且Jadad评分较低,本文未予纳入。
1.2 文献纳入与采集 文献纳入、采集及核对由2名参与者独立完成并交叉核对,如遇分歧则讨论解决。采集以下数据,包括研究设计方法、发表时间、患者年龄、干预药物剂量/时间、结果和Jadad评分。本文采用Jadad评分量表[2],对纳入文献进行质量评估,包括随机化、双盲和退出/丢失,分值为1~5分。分值越高提示研究质量越好,1~2分提示研究质量欠佳。本文主要终点是TNSS,包括鼻塞、流涕、瘙痒和喷嚏等4个症状,积分越高提示症状越严重,因各研究总分值不一致,本文采用最高分值的百分比进行分析。次要终点为生活质量问卷评分RQLQ和NSS,RQLQ包括7个指标:活动、睡眠、鼻部症状、眼部症状、非鼻/非眼部症状、活动情况和情绪,较高的分值提示生活质量较差;NSS由3部分组成:难以入睡、夜间觉醒以及鼻塞情况,0分表示无症状,3分为症状最严重。因为相关纳入研究结论数据表示方式不一致,为了增加可比性,本文统一采用了变化值(结果值减去基线值)进行分析。其中一项纳入的研究[3]包含了2个临床试验。在3项研究[4-6]中,变化值的标准差根据结果和基线值的标准差计算得到。在其他纳入研究中,变化值标准差由95%的置信区间的推断而来。非正态分布的数据[7]未采用。上述所有的推算公式均来自Cochrane手册。
1.3 数据分析 本文中对于连续变量计算其加权均数差(固定效应模型)和95%的置信区间。对于二分类变量采用Mantel-Haenszel计算比值比和95%置信区间。如果检测到显著异质性(P<0.1),则先尝试分析异质性的可能原因,采用分层分析或选择随机效应模型。
1.4 统计学处理 所有的统计分析采用RevMan 5.1完成。
2 结果
初始检索得到526篇研究,经阅读标题和摘要后504篇被排除,剩余22篇。经全文评估后,又排除12篇,包括2项非随机对照试验[8-9],6项交叉试验[10-15](其中4项[10-11,13-14]为同一临床研究),3项研究仅单次剂量治疗[16-18],1项研究数据不足[19]。最终10篇研究符合标准纳入,其中1项纳入的研究[3]包含了2个临床试验,表示为 Lu 2009a和Lu 2009b。所有纳入研究均发表于2000~2013年;治疗时间为14~50天。在方法学质量评分方面,1项研究[6]使用随机、单盲方法,Jadad评分为1分。其他的研究Jadad评分在3~5分,详见表1。

表1 纳入研究的临床特征
2.1 TNSS评分 M/L组与孟鲁司特组 (MD=-0.05,-0.07~-0.03,95%CI,图1)、氯雷他定组(MD =-0.03,-0.05~-0.01,95%CI,图2)和安慰剂(MD =-0.10,0.12~-0.08,95%CI,图3)比较差异均有统计学意义(P<0.001)。
2.2 RQLQ评分 M/L组与孟鲁司特组 (MD= 0.12,-0.26 0.01,95%CI,图4)、氯雷他定组(MD =0.10,-0.23~0.02,95%CI,图4)相比有所降低,但差异无统计学意义(P>0.05)。与安慰剂组相比,M/L可明显降低 RQLQ评分(MD=-0.45,-0.59~-0.32,95%CI,图5),差异均有统计学意义 (P<0.001)。
2.3 NSS评分 M/L组与孟鲁司特组(MD=0.01,-0.12~0.09,95%CI,图6)、氯雷他定组 (MD= 0.07,-0.17~0.03,95%CI,图6)相比有所降低,但差异无统计学意义(P>0.05)。

图1 M/L联合疗法与孟鲁斯特(M)TNSS比较(TNSS数值表示为最大值的百分数)

图2 M/L联合疗法与氯雷他定(L)TNSS比较(TNSS数值表示为最大值的百分数)

图3 M/L联合疗法与安慰剂(P)TNSS比较

图4 M/L联合疗法与单药疗法(M或L)RQLQ比较
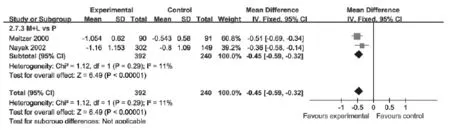
图5 M/L联合疗法与安慰剂(P)RQLQ比较

图6 M/L联合疗法与单药疗法(M或L)NSS比较
3 讨论
AR的治疗方案较多,但临床上仍有部分患者病情难以控制,为了更好地控制AR症状,常采取联合用药方案。目前较多研究评估了联合使用抗组胺药和白三烯受体拮抗剂对AR患者的疗效,但是由于研究样本量、方式以及干预药物类型的不同等原因,尚未达成一致的结论。有研究指出在控制AR鼻部症状方面,联合疗法(M/L[15],孟鲁司特和非索非那定[21])和单药治疗(非索非那定)之间并无明显统计学差异,而另外2个交叉研究[3,22]指出M/L联合疗法在改善鼻症状方面优于单药治疗,提示不同的药物组合对于AR可能具有不同的效果。另外,检索还发现目前已有3项综述[23-25]通过荟萃分析比较了AR联合疗法与单药疗法,但是均将不同的抗组胺药合并在一起,包括氯雷他定、左西替利嗪、非索非那定,由于上述研究已指出不同联合疗法对AR可能具有不同效果,因此此类合并可能会加大荟萃分析的异质性。而且在这3项综述中,只有1项综述[25]提示联合疗法在改善鼻部症状方面优于单药治疗。
为了明确M/L联合疗法是否优于单药治疗,本文从日间鼻部症状、生活质量、夜间症状等3方面比较两者疗效,以期为临床用药提供循证学依据。
本文纳入的10篇研究中仅有2篇[3,22]研究表明在改善鼻部症状方面,M/L联合疗法优于孟鲁斯特或氯雷他定。而本次荟萃分析发现,无论与孟鲁斯特还是氯雷他定单药治疗相比,M/L联合疗法均可以明显改善鼻部症状(P<0.001),这可能与组胺和白三烯在AR发病过程中不同的作用机制相关。研究[26-27]指出,在AR炎症反应中,组胺异常分泌往往可以引起鼻部分泌物增多,瘙痒和喷嚏,但只有在较高浓度时才会引起鼻塞,而白三烯分泌增多可刺激杯状细胞分泌粘液,减弱纤毛清除功能,从而引起鼻塞等症状。因此,理论上M/L联合疗法在改善鼻部症状方面可能具有协同效应,与本次荟萃分析结果相符。而近期发表的一篇综述[28]提示在改善日间鼻部症状方面,M/L联合疗法可能优于孟鲁斯特,但与氯雷他定相比无明显统计学差异,该结论可能与该综述纳入研究数目较少有关。
本文纳入的研究中,3篇[3,22,29]进行了M/L联合疗法和单药治疗在改善AR患者生活质量上的比较,其中Lu[3]2009a指出,相比于孟鲁司特或氯雷他定单药治疗,可更好地改善生活质量。本文发现,M/ L联合疗法与孟鲁斯特或者氯雷他定相比,均可明显降低RQLQ评分,但无明显统计学差异(图4)。但是,图4提示,如将两组单药疗法合并,M/L联合疗法与单药疗法的整体效应差异存在统计学意义(P<0.05),可能由于RQLQ评分中不仅包括鼻部症状,也包括了眼部症状、非鼻/非眼部症状、活动和睡眠等,M/L联合疗法可以明显改善鼻部症状,在RQLQ其他方面作用可能与单药疗法无差异。但考虑在两组合并研究的过程中重复使用了相同数据,可能存在严重偏倚,故该结论需进一步研究证实。
在改善夜间症状方面,仅2篇[22,29]研究纳入了本次分析,提示M/L联合疗法与孟鲁斯特或氯雷他定方面无统计学差异。此外,另有3篇[6,30-31]研究比较了M/L联合疗法与抗组胺疗法对夜间症状的疗效,但均提示无统计学差异。但是,Lu[3]2009指出在改善复合症状 (包括白天鼻部症状、夜间症状)方面,M/L联合疗法优于孟鲁斯特,与一项综述[28]结论相同。本文认为,NSS包括难以入睡、夜间觉醒以及鼻塞三方面,而孟鲁斯特与氯雷他定并无明显中枢镇静作用,根据本次荟萃分析及相关研究,M/L联合疗法在改善夜间症状方面并不优于单药治疗;但因复合症状中包括了日间鼻部症状,而Lu 2009样本量也相对较大,故Lu 2009及上述综述得出了相反结论。因此,根据现阶段研究尚不能表明M/L联合疗法在改善夜间症状方面优于单药治疗。具体有待于大样本证实。
在不良反应方面,已有相关研究指出孟鲁斯特或氯雷他定治疗均可能引起头痛、口干等不良反应,但均无统计学差异,与Prenner等[32]报道结论相符。本文3篇研究[3,22,29]记录了不良反应,包括头痛、口干、疲劳等,但其中大部分为轻度或自限性,由于数据不足本文未对此进行分析。
由于纳入研究的报道数据多样化,本文也存在一些局限性。首先,在评估生活质量问卷和夜间症状方面,只有2篇[22,29]研究符合纳入标准,虽结论提示无统计学差异,但仍需进一步研究证实。其次,由于不同药物组合对改善AR症状效果不一,为了减少异质性,本文只纳入了M/L联合疗法,另外不同的组合被排除在外,对这些不同药物组合(比如孟鲁斯特和左西替利嗪,孟鲁司特和非索非那定)尚需进一步的研究以明确疗效。
总之,M/L联合疗法较之单药疗法可改善AR患者的鼻部症状,但对于生活质量及夜间症状的改善,目前尚认为M/L联合疗法与单药疗法无明显差异,还需大样本临床试验证实。
[1] Van Cauwenberge P,Bachert C,Passalacqua G,et al.Consensus statement on the treatment of allergic rhinitis.European Academy of Allergology and Clinical Immunology.Allergy,2000,55(2):116
[2] Jadad AR,Moore RA,Carroll D,et al.Assessing the quality of reports of randomized clinical trials:is blinding necessary. Controlled clinical trials,1996,17(1):1
[3] Lu S,Malice MP,Dass SB,et al.Clinical studies of combination montelukast and loratadine in patients with seasonal allergic rhinitis.The Journal of asthma:official journal of the Association for the Care of Asthma,2009,46(9):878
[4] Hung CH,Hua YM,Hsu WT,et al.Montelukast decreased exhaled nitric oxide in children with perennial allergic rhinitis.Pediatrics international:official journal of the Japan Pediatric Society,2007,49(3):322
[5] Moinuddin R,deTineo M,Maleckar B,et al.Comparison of the combinations of fexofenadine-pseudoephedrine and loratadine-montelukast in the treatment of seasonal allergic rhinitis.Annals of allergy,asthma&immunology:official publication of the American College of Allergy,Asthma,& Immunology,2004,92(1):73
[6] Pullerits T,Praks L,Ristioja V,et al.Comparison of a nasal glucocorticoid,antileukotriene,and a combination of antileukotriene and antihistamine in the treatment of seasonal allergic rhinitis.The Journal of allergy and clinical immunology,2002,109(6):949
[7] Saengpanich S,deTineo M,Naclerio RM,et al.Fluticasone nasal spray and the combination of loratadine and montelukast in seasonal allergic rhinitis.Archives of otolaryngology—head&neck surgery,2003,129(5):557
[8] Cingi C,Oghan F,Eskiizmir G,et al.Desloratadine-montelukast combination improves quality of life and decreases nasal obstruction in patients with perennial allergic rhinitis. International forum of allergy&rhinology,2013,3(10):801
[9] Cingi C,Oghan F,Eskiizmir G,et al.Health-related quality of life and prognostic value of acoustic rhinometry in patients with perennial allergic rhinitis treated with fix combination of montelukast plus desloratadine.World Allergy Organization Journal,2012,5:98
[10]Ciebiada M,Barylski M,Gorska Ciebiada M.Nasal eosinophilia and serum soluble intercellular adhesion molecule 1 in patients with allergic rhinitis treated with montelukast alone or in combination with desloratadine or levocetirizine.American journal of rhinology&allergy,2013,27(2):e58
[11]Ciebiada M,Gorska-Ciebiada M,Barylski M,et al.Use of montelukast alone or in combination with desloratadine or levocetirizine in patients with persistent allergic rhinitis.American journal of rhinology&allergy,2011,25(1):e1
[12]Moskovljevic J,Zivkovic M.Treatment of persistent allergic rhinitis with montelukast with desloratadine or levocetirizine. Allergy:European Journal of Allergy and Clinical Immunology,2010,65:153
[13]Ciebiada M,Ciebiada MG,Kmiecik T,et al.Quality of life in patients with persistent allergic rhinitis treated with montelukast alone or in combination with levocetirizine or desloratadine.Journal of investigational allergology&clinical immunology,2008,18(5):343
[14]Ciebiada M,Gorska-Ciebiada M,DuBuske LM,et al.Montelukast with desloratadine or levocetirizine for the treatment of persistent allergic rhinitis.Annals of allergy,asthma& immunology:official publication of the American College of Allergy,Asthma,&Immunology,2006,97(5):664
[15]Wilson AM,Orr LC,Coutie WJ,et al.A comparison of once daily fexofenadine versus the combination of montelukast plus loratadine on domiciliary nasal peak flow and symptoms in seasonal allergic rhinitis.Clinical and experimental allergy: journal of the British Society for Allergy and Clinical Immunology,2002,32(1):126
[16]Horak F,Zieglmayer P,Zieglmayer R,et al.Onset of action of loratadine/montelukast in seasonal allergic rhinitis patients exposed to grass pollen.Arzneimittel-Forschung,2010,60(5):249
[17]Day JH,Briscoe MP,Ratz JD,et al.Onset of action of loratadine/montelukast in seasonal allergic rhinitis subjects exposed to ragweed pollen in the Environmental Exposure Unit. Allergy and asthma proceedings:the official journal of regional and state allergy societies,2009,30(3):270
[18]Day JH,Briscoe MP,Ratz JD,et al.Efficacy of loratadinemontelukast on nasal congestion in patients with seasonal allergic rhinitis in an environmental exposure unit.Annals of allergy,asthma&immunology:official publication of the American College of Allergy,Asthma,& Immunology,2009,102(4):328
[19]Ciprandi G,Tosca MA,Milanese M,et al.Antihistaminesadded to an antileukotriene in treating seasonal allergic rhinitis:histamine and leukotriene antagonism.European annals of allergy and clinical immunology,2004,36(2):67,2
[20]Yamamoto H,Yamada T,Sakashita M,et al.Efficacy of prophylactic treatment with montelukast and montelukast plus add-on loratadine for seasonal allergic rhinitis.Allergy and Asthma Proceedings,2012,33:17
[21]Lee DK,Jackson CM,Soutar PC,et al.Effects of single or combined histamine H1-receptor and leukotriene CysLT1-receptor antagonism on nasal adenosine monophosphate challenge in persistent allergic rhinitis.British journal of clinical pharmacology,2004,57(6):714
[22]Meltzer EO,Malmstrom K,Lu S,et al.Concomitant montelukast and loratadine as treatment for seasonal allergic rhinitis:a randomized,placebo-controlled clinical trial.The Journal of allergy and clinical immunology,2000,105(5):917 [23]Rodrigo GJ,Yanez A.The role of antileukotriene therapy in seasonal allergic rhinitis:a systematic review of randomized trials.Annals of allergy,asthma&immunology:official publication of the American College of Allergy,Asthma,& Immunology,2006,96(6):779
[24]Grainger J,Drake-Lee A.Montelukast in allergic rhinitis:a systematic review and meta-analysis.Clinical otolaryngology: official journal of ENT-UK;official journal of Netherlands Society for Oto-Rhino-Laryngology&Cervico-Facial Surgery,2006,31(5):36
[25]Wilson AM,O'Byrne PM,Parameswaran K.Leukotriene receptor antagonists for allergic rhinitis:a systematic review and meta-analysis.The American journal of medicine,2004,116(5):338
[26]Kurowski M,Kuna P,Gorski P.Montelukast plus cetirizine in the prophylactic treatment of seasonal allergic rhinitis:influence on clinical symptoms and nasal allergic inflammation. Allergy,2004,59(3):280
[27]Steinhilber D,Hofmann B.Recent advances in the search for novel 5-lipoxygenase inhibitors.Basic&clinical pharmacology&toxicology,2014,114(1):70
[28]陆忆殷,程雷.白三烯受体拮抗剂孟鲁司特治疗变应性鼻炎的荟萃分析.中国耳鼻咽喉头颈外科杂志,2014,49(8):659
[29]Nayak AS,Philip G,Lu S,et al.Efficacy and tolerability of montelukast alone or in combination with loratadine in seasonal allergic rhinitis:a multicenter,randomized,doubleblind,placebo-controlled trial performed in the fall.Annals of allergy,asthma&immunology:official publication of the American College of Allergy,Asthma,& Immunology,2002,88(6):592
[30]Prenner B,Anolik R,Danzig M,et al.Efficacy and safety of fixed-dose loratadine/montelukast in seasonal allergic rhinitis:effects on nasal congestion.Allergy and asthma proceedings:the official journal of regional and state allergy societies,2009,30(3):263
[31]Watanasomsiri A,Poachanukoon O,Vichyanond P.Efficacy of montelukast and loratadine as treatment for allergic rhinitis in children.Asian Pacific Journal of Allergy and Immunology,2008,26(2-3):89
[32]Prenner BM,Lu S,Danzig MR.Safety of fixed-dose loratadine/montelukast in subjects with allergic rhinitis.Allergy and asthma proceedings:the official journal of regional and state allergy societies,2010,31(6):4
猜你喜欢
中国药学药品知识仓库(2022年10期)2022-05-29
中国药学药品知识仓库(2022年9期)2022-05-23
医学概论(2022年4期)2022-04-24
中国医药科学(2021年11期)2021-07-16
世界最新医学信息文摘(2021年12期)2021-06-09
中国美容医学(2019年3期)2019-03-25
中国实用医药(2017年33期)2017-12-12
糖尿病新世界(2017年9期)2017-09-07
中国实用医药(2016年4期)2016-02-23
新农村(2015年9期)2015-09-24
