
Unusual neural tract between injured fornix and pedunculopontine nucleus in a patient with traumatic brain injury
2017-10-11 02:21SungHoJang,JeongPyoSeo
中国神经再生研究(英文版) 2017年9期
IMAGING IN NEURAL REGENERATION
Unusual neural tract between injured fornix and pedunculopontine nucleus in a patient with traumatic brain injury
It has been known that four cholinergic nuclei are located in the septal region and basal forebrain (Ch 1: medial septal nucleus,Ch 2: vertical nucleus of the diagonal band, Ch 3: horizontal limb of the diagonal band and Ch 4: nucleus basalis of Meynert)and two are located in the brainstem (Ch 5: pedunculopontine nucleus and Ch 6: laterodorsal tegmental nucleus) (Selden et al.,1998; Lucas-Meunier et al., 2003; Mesulam, 2004; Nieuwenhuys et al., 2007). Te fornix transfers information on episodic memory between the medial diencephalon and the medial temporal lobe (Afifiand Bergman, 2005; Wolk and Budson, 2010). The fornix is known to obtain cholinergic innervation from Ch 1 and Ch 2, and to project to the hippocampal formation (Selden et al., 1998; Lucas-Meunier et al., 2003; Mesulam, 2004; Nieuwenhuys et al., 2007; Dere et al., 2008; Naidich and Duvernoy,2009; Isaacson and Pribram, 2013).
In this study, using DTT, we attempted to demonstrate an unusual neural tract between the injured fornix and Ch 5viathe thalamus in a patient with TBI.
A 64-year-old, right-handed male patient who had suffered a traffic accident underwent conservative management for subarachnoid hemorrhage, subdural hematoma, and skull fracture at the department of neurosurgery of a university hospital.Findings on brain MRI performed 6 months after onset showed multiple leukomalactic lesions in both frontal lobes and basal forebrain (Figure 1A). Evaluation of cognitive function performed at 6 months after onset showed severe cognitive impairment (decreased alertness, Mini-Mental State Exam (Tombaugh and McIntyre, 1992) score: uncheckable) and severe quadriparesis (Manual Muscle Test (Wintz, 1959): right upper and lower extremities – 0–2, left upper and lower extremities – 3–4. Five normal age-matched normal subjects (2 males; mean age: 59.6 years, range: 55–65 years) withouwt history of neurologic or psychiatric disease were included as controls. Our institutional review board approved the study protocol.
Using a sensitivity-encoding head coil, DTIs were acquired on a 1.5-T at 6 months after onset. We acquired 60 contiguous slices parallel to the anterior and posterior commissure lines for each of the 32 non-collinear diffusion sensitizing gradients. DTI parameters were as follows: total scanning time = 7 minutes 32 seconds; repetition time = 10,726 ms; acquisition matrix = 96 ×96; echo time = 76 ms; number of excitations = 1; reconstruction matrix = 192 × 192 matrix; thickness = 2.5 mm;b= 1,000 s/mm2; and field of view = 240 × 240 mm2. Fiber assignment continuous tracking (FACT) algorithm was used for fiber tracking (Mori et al., 1999). For analysis of the fornix, the first region of interest (ROI) was placed on the middle of the body and the second ROI was placed on the junction between the body and crus on the coronal slice of the color map (green color) (Hong and Jang, 2010). Termination criteria were fractional anisotropy> 0.2 and angle change < 45°.
Findings on 6-month DTT showed discontinuations in the anterior portion of the fornix body and both crus. Te end of the fornix body was connected to the right pedunculopontine nucleus (Ch 5)viaa neural tract that passed through the right thalamus (Figure 1B). However, we did not find this neural tract between the fornix and Ch 5 in five normal age-matched normal subjects (2 males; mean age: 59.6 years, range: 55–65 years)(Figure 1C).
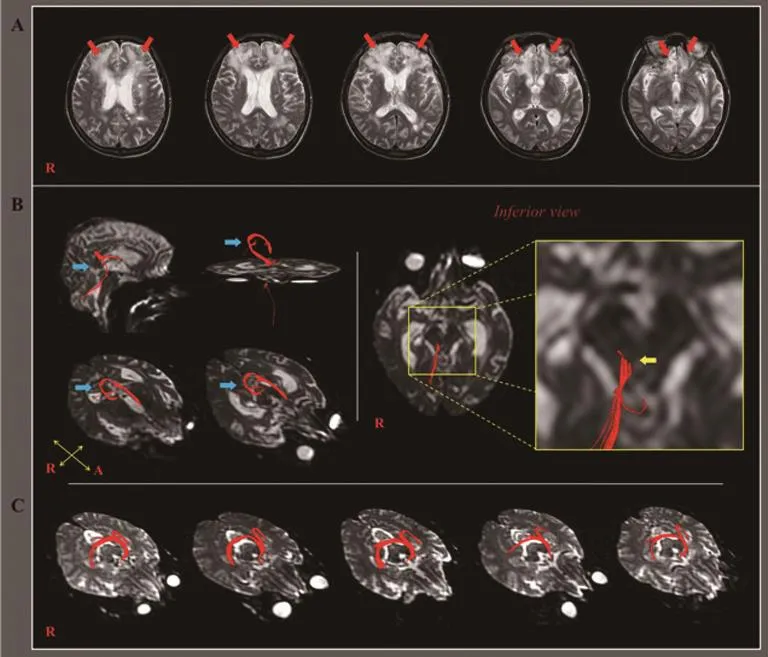
Figure 1 T2-weighted MRI and DTT images in a 64-year-old male patient with traumatic brain injury.
In the current study, we observed an unusual neural tract between the injured fornix and Ch 5viathe thalamus in a patient with TBI. Tis neural tract was not observed in any of five agematched normal subjects. Findings on 6-month DTT for the fornix showed severe injury (discontinuation) of the anterior portion of the fornix body. Consequently, it appears that the neural pathway from Ch 1 and Ch 2 was completely injured.The fornix is known to obtain cholinergic innervation from Ch 1 and Ch 2 (Selden et al., 1998; Lucas-Meunier et al., 2003;Mesulam, 2004; Dere et al., 2008; Naidich and Duvernoy, 2009;Isaacson and Pribram, 2013). On the other hand, some studies have reported that the thalamus is a target area of Ch 5 (Mesulam et al., 1983; Woolf and Butcher, 1986; Mesulam, 1990; Paxinos,1990; Butcher and Woolf, 2004; Naidich and Duvernoy, 2009).Terefore, the unusual neural tract between the injured fornix and Ch 5 appears to be a compensatory phenomenon to allow the injured fornix to obtain cholinergic innervation from Ch 5 instead of Ch 1 and 2, following destruction of the cholinergic pathway from Ch 1 and Ch 2 to the fornix. Because the cholinergic nuclei are interconnected with each other, this unusual neural connection observed on DTT might be the result of process of recovery for injured cholinergic innervations or facilitation of a weak already existing neural connection (Mesulam,1990).
Since introduction of DTI, unusual neural tracts between an injured fornix and brainstem cholinergic nuclei have recently been reported in stroke patients (a patient with subarachnoid and intraventricular hemorrhage: the neural tract between the injured fornix and Ch 5, and a patient with cerebral infarct:the neural tract between the injured fornix and Ch 6 (Yeo and Jang, 2013; Jang and Seo, 2016). As a result, as far as we are aware, this is the first study to demonstrate the unusual neural tract which connected between injured fornix and brainstem cholinergic nuclei in patients with TBI. However, our results are limited to this case report. Further studies involving larger numbers of patients are warranted. In addition, the lack of DTI at onset and long-term follow up DTI should be considered in future studies. Moreover, studies on the clinical significance of this unusual neural tract should be encouraged.
In conclusion, we report on a patient who showed an unusual neural tract between the injured fornix and Ch 5 following traumatic brain injury. We believe that our findings may suggest a possible recovery phenomenon between cholinergic nuclei and the Papez circuit following brain injury.
This work was supported by the Medical Research Center Program (2015R1A5A2009124) through the National Research Foundation of Korea (NRF) funded by the Ministry of Science,ICT and Future Planning.
Sung Ho Jang, Jeong Pyo Seo*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daemyungdong, NamGu, Daegu,Republic of Korea
*Correspondence to:Jeong Pyo Seo, M.S., raphael0905@hanmail.net.
Accepted:2017-01-14
orcid:0000-0002-2695-7957 (Jeong Pyo Seo)
How to cite this article:Jang SH, Seo JP (2017) Unusual neural tract between injured fornix and pedunculopontine nucleus in a patient with traumatic brain injury. Neural Regen Res 12(9):1559-1560.
Author contributions:SHJ conceived and designed the study, was responsible for fundraising, data acquisition, manuscript development and writing. JPS participated in data acquisition, manuscript development,writing and authorization. Both of these two authors approved the ?nal version of this paper.
Conflicts of interest:Te authors reports no disclosures relevant to the manuscript.
Ethics:Te study was approved by the institutional review board of Yeungnam University Hospital.
Declaration of participant consent:Te authors certify that they have obtained the appropriate participant consent forms. In the form, participants have given their consent for their images and other clinical information to be reported in the journal. Te participants understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Plagiarism check:Checked twice by iTenticate.
Peer review:Externally peer reviewed.
Open access statement:Tis is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
AfifiAK, Bergman RA (2005) Functional neuroanatomy: text and atlas, 2ndEdition. New York: Lange Medical Books/McGraw-Hill.
Butcher LL, Woolf NJ (2004) Cholinergic neurons and networks revisited. In:Te rat nervous system, 3rd Edition (Paxinos G, ed), pp 1257-1268. Amsterdam; Boston: Elsevier Academic Press.
Dere E, Easton A, Nadel L, Huston JP (2008) Handbook of Episodic Memory:Elsevier Science.
Hong JH, Jang SH (2010) Degeneration of cingulum and fornix in a patient with traumatic brain injury: diffuse tensor tractography study. J Rehabil Med 42:979-981.
Isaacson RL, Pribram KH (2013) Te Hippocampus. Springer US.
Jang SH, Seo YS (2016) A new neural tract between injured fornix and brainstem cholinergic nucleus in a stroke patient. Am J Phys Med Rehabil doi:10.1097/PHM.0000000000000469.
Lucas-Meunier E, Fossier P, Baux G, Amar M (2003) Cholinergic modulation of the cortical neuronal network. Pflugers Arch 446:17-29.
Mesulam MM (1990) Human brain cholinergic pathways. Prog Brain Res 84:231-241.
Mesulam MM (2004) Te cholinergic innervation of the human cerebral cortex. Prog Brain Res 145:67-78.
Mesulam MM, Mufson EJ, Wainer BH, Levey AI (1983) Central cholinergic pathways in the rat: an overview based on an alternative nomenclature(Ch1-Ch6). Neuroscience 10:1185-1201.
Mori S, Crain BJ, Chacko VP, van Zijl PC (1999) Tree-dimensional tracking of axonal projections in the brain by magnetic resonance imaging. Ann Neurol 45:265-269.
Naidich TP, Duvernoy HM (2009) Duvernoy’s atlas of the human brain stem and cerebellum: high-field MRI: surface anatomy, internal structure, vascularization and 3D sectional anatomy. Wien; New York: Springer.
Nieuwenhuys R, Voogd J, Huijzen CV (2007) The human central nervous system, 4thEdition. New York: Springer.
Paxinos G (1990) Te Human nervous system. San Diego: Academic Press.
Selden NR, Gitelman DR, Salamon-Murayama N, Parrish TB, Mesulam MM(1998) Trajectories of cholinergic pathways within the cerebral hemispheres of the human brain. Brain 121(Pt 12):2249-2257.
Tombaugh TN, McIntyre NJ (1992) The mini-mental state examination: a comprehensive review. J Am Geriatr Soc 40:922-935.
Wintz MN (1959) Variations in current manual muscle testing. Phys Ther Rev 39:466-475.
Wolk DA, Budson AE (2010) Memory systems. Continuum (Minneap Minn)16:15-28.
Woolf NJ, Butcher LL (1986) Cholinergic systems in the rat brain: III. Projections from the pontomesencephalic tegmentum to the thalamus, tectum,basal ganglia, and basal forebrain. Brain Res Bull 16:603-637.
Yeo SS, Jang SH (2013) Recovery of an injured fornix in a stroke patient. J Rehabil Med 45:1078-1080.
Copyedited by Li CH, Song LP, Wang L
10.4103/1673-5374.215269

- 中国神经再生研究(英文版)的其它文章
- Tp53 gene mediates distinct dopaminergic neuronal damage in different dopaminergic neurotoxicant models
- Structure and function of the contactin-associated protein family in myelinated axons and their relationship with nerve diseases
- Promises and pitfalls of immune-based strategies for Huntington’s disease
- Post electrical or lightning injury syndrome: a proposal for an American Psychiatric Association’s Diagnostic and Statistical Manual formulation with implications for treatment
- Odorants could elicit repair processes in melanized neuronal and skin cells
- Neuroprotective effects of erythropoietin on neurodegenerative and ischemic brain diseases: the role of erythropoietin receptor