
Colorectal cancer fecal screening test completion after age 74,sources and outcomes in French program
2019-09-19 06:45AkoKovoguiChristianBalamouRaushanRymzhanovaTuLetrungHamouAitHadadZahidaBrixiStphaneCornelisneDelattreMassyThomasAparicioRobertBenamouzig
Akoï Koïvogui,Christian Balamou,Raushan Rymzhanova,Tu Letrung,Hamou Ait Hadad,Zahida Brixi,Stéphane Cornelis,Hélène Delattre-Massy,Thomas Aparicio,Robert Benamouzig
Abstract
Key words: Colorectal cancer;Fecal screening test;Participation rate;Colonoscopy completion rate;Elderly
INTRODUCTION
In addition to its high incidence and high mortality (around 42000 new cases and 18000 deaths per year),colorectal cancer (CRC) meets all the conditions to be screened in France[1-3].Screening every two years,allows to obtain a reduction in CRC mortality in tested population[2,3].In Burgundy,this decrease in mortality was of the order of 16% after 11 years of follow-up of a cohort of 45000 individuals[2].European Commission recommended the implementation of the Colorectal Cancer Screening Program (CRCSP) by the search for occult bleeding in stool to face the high morbidity and mortality associated with CRC[4].Following the recommendations,the screening of the CRC started in Germany in 1977[5],was progressively implemented between 2000 and 2010 in other European countries,through CRC screening pilot programs,notably in England[6],in Italy[7]in Holland[8,9]and in France[10].
(1) 微扰动注浆整治对盾构隧道治理效果为:注浆区间中部朝着注浆位置反方向水平位移,两端向注浆位置方向水平移动;注浆引起隧道沉降,且呈明显的注浆区间中部沉降大,两端沉降小;隧道形状逐渐由压扁状向撑圆状变化,水平收敛近似等同于竖直收敛,且受隧道所处的周围土压力影响,竖直收敛量略大于水平向收敛量。
To date,most of the CRCSP policies target a medium risk population of CRC,defined on the age criterion with considerable variability from one program to another[11].Since the effectiveness of screening depends on its application in an appropriate setting and at an appropriate frequency[12],most European programs,observe an interval of 2 years between two screenings campaign.The test was offered to people (all gender) aged between 40 and 60 in Bulgaria,between 50 and 74 in France,England and Belgium;between 50 and 70 in Italy,between 55 and 75 in Holland[13].The justification of these age groups remains controversial in the current state of knowledge.Indeed,there is little objective data to justify discontinuation of screening at 75 years.Recent Modeling was proposed to estimate from what age it was desirable to no longer invite to do the screening.They estimate screening up to age 82 as relevant[14,15].
In France,as in other countries,the CRCSP does not include people aged ≥ 75 years,despite the high incidence of CRC after 74 years[16]and the constant increase in life expectancy since 2000[17].It seems necessary to guide the debate on the problem of screening among the elderly.Indeed,in each French district,the sporadic participation of elderly patients aged at least 75 years old (Elderly_75),out of the national CRCSP’s recommendation,is recorded every year.We describe here,these CRC fecal screening test completion after age 74,the source (screening program or provider ordered) and outcomes.
MATERIALS AND METHODS
Ethical considerations
Before analysis,all data were anonymized.The screening database had a favorable opinion from the institution that oversees the ethics of data collection (“Commission nationale de l'informatique et des libertés”:CNIL).According to the current French legislation,a study that does not change the care of patients did not require the opinion of the Clinical Research Centers Ethics Committee.This article does not contain any studies with human participants performed by any of the authors.This study does not involve human participants and informed consent was therefore not required.This article does not contain any studies with animals performed by any of the authors.
Study design
A descriptive study of 18704 Elderly_75s,residing in eleven French districts (Ain,Doubs,Essonne,Haute-Saone,Hauts-de-Seine,Jura,Seine-Saint-Denis,Territoire-de-Belfort,Val-de-Marne,Val-d’Oise,Yonne),having performed a CRC screening test between January 1,2008 and December 31,2017.The circumstances of performing this test (source of the test,previous behavior in the CRCSP) and the outcome (test result,colonoscopy completion and detected lesions) were described.
Distribution of screening tests in the districts
On a voluntary basis,the eleven districts were chosen in three French regions(Bourgogne-Franche-Comté,Ile-de-France,Rhône-Alpes-Auvergne),among those using the same screening database management's materials.With a population (50-74 years) of 2355240 persons targeted by the 2015-2016 screening campaign,these eleven districts totaled 554294 participants in this campaign,with an average participation rate estimated at 23.5%[18].
In France,a nationwide population based CRCSP was rolled out from January 2008 to December 2009.The program was based on a biennial guaiac faecal occult blood test distributed to men and women aged 50-74 at average risk of developing CRC.If positive,the test was followed by a total colonoscopy[19,20].CRCSP was organized at a district level by the local cancer screening managing center (Managing-Center),in accordance with CRCSP's national specifications[19,20].Each year,people targeted by the campaign receive a letter inviting them to take a free screening test from their General Practitioner (GP).The pattern of distribution of the screening test recommends that the GP gives the screening test to any person aged 50 to 74 years,provided with an invitation letter.In the absence of this letter,the GP may give the test after establishing the eligibility of the person,using a connection made available to doctors or by calling to the Managing-Center.Until July-November,2014,people who did not tested after the first recall letter,received the test kit at home,six months after the initial solicitation.The only organizational change (related to the objective of the study) imposed by the introduction of a new screening testi.e.,OC-sensor© fecal immunochemical test (FIT) replacing guaiac test in May 2015,was the supplying mode of GPs in screening tests kit,the classic pattern of kit distribution remaining unchanged.
Operational definition of variables and descriptive analysis
For each Elderly_75 having performed a test out of recommendation,solicitation/participation data from previous campaigns were extracted from the Managing-Centers databases.These databases were regularly enriched by sociodemographic data (gender,age),colonoscopy,histopathology and follow-up data provided by partners (Health Insurance Plan,Medical Information Services,Gastroenterologists,Surgeons,GP,etc.).The tests performed in a circumstance of delayed response after a solicitation (DRS,initial or recall letter existing) from the Managing-Center,done before 75 years were distinguished from the tests nonsolicited by the Managing-Center,performed after a recommendation by a GP or other provider ordered (RGP).DRS was any test realized by an Elderly_75 following an initial invitation from the Managing-Center with a maximum 24 months after this invitation.Any Non-DRS test was considered RGP.
Previous behavior in the CRCSP:Anteriority in the CRCSP was defined by the existence of at least one solicitation to participate in a CRCSP campaign between 50 and 74 years of age.The previous behavior in terms of the outcome of these earlier solicitations was described.
For each solicitation,the participation was defined as carrying out a fecal occult blood test according to the specifications of the French CRCSP[19,20].For each person,the adherence to testing was evaluated as frequency of participation in previous campaigns.This frequency was expressed by the ratio between the observed number of participations in previous campaign and the expected number of participations in these previous campaigns.Considering the bi-annual organization of screening campaigns and a person age (X) at the date of first invitation in the district,the expected number of participation for a person aged Y year old,was (Y-X)/2.It was coded as a discrete variable:Without anteriority (The person was never solicited in the district program);Never participated (The person has not participated in any of the previous campaigns to which it was solicited);Participated with frequency < 30%of campaigns;frequency between 30 and 50%;frequency > 50% to 75% and frequency> 75%.
For Elderly_75 with a history of solicitation,the presence of a history of NLAI(Does Not Live at the Address Indicated) or refusal to participate in a campaign was collected and coded as a binary variable (No/Yes).Similarly,the presence of a history of colonoscopy,reported by a mailing response after solicitation,was described as a binary variable (No/Yes).If the person participated in at least one campaign,history of positive test and colonoscopy performed after this positive test was collected and coded as a discrete variable:No history of positive test,positive test without colonoscopy,positive test with normal colonoscopy,positive test with positive colonoscopy.
CRC fecal screening test completion after age 74:The outcome of screening test performed after 74 years was analyzed in terms of test quality (non-analyzable test proportion) and test result (Negative,Positive).In the event of a positive result,the diagnostic course has been analyzed in terms of frequency of colonoscopy completion and in terms of frequency and types of diagnosed lesions including:Low-risk-polyps,High-risk-polyps,Unspecified-polyp and CRC.High-risk-polyps included,Adenomas ≥ 10 mm (except hyperplastic polyps),Serrated adenomas,Adenomas with high grade dysplasia,Villous or Tubulo-villous adenomas.The diagnoses associated with CRC and polyps were those related to the C18-C20 and D12 codes of the 10th version of the WHO International Classification of Diseases[21].The positive predictive value (PPV) of the test was estimated as the proportion of lesions among the Elderly_75 who completed a colonoscopy after a positive test.
Statistical analysis
Qualitative variables were described in frequency and quantitative variables were described in mean ± SD.Frequencies were compared between groups by a Pearsonχ2test or Fisher’s exact test.Means were compared between two groups by Student'sTtest.All the analyzes were carried out with version 13 of STATA software (College Station,Texas,United States) andP< 0.05 was considered for statistical significance.
RESULTS
Modality of participation
Of 18704 Elderly_75 (56.3% female),performed 18995 tests between January 1,2008 and December 31,2017.These 18995 screening-tests were performed at ages:75(83.5%),76-80 (13.4%) and > 80 (3.1%) years old.Over this period,250 Elderly_75 out of 18704 completed at least 2 tests after the age of 74.On average,over one year of campaign,7 out of 1000 tests were realized by people aged ≥ 75 years.This proportion reached 15 per 1000 in 2015 (Table 1).13442 people (71.9% of the sample),performed the first test after the age of 74,in a circumstance of DRS of the Managing-center.This response delayed by 7.8 ± 5.3 mo after the initial solicitation.For those who have performed a test under recommendation and have an anteriority in CRCSP,the delay between the last test in the CRCSP and this test was 37.6 ± 18.9 mo.
Mean age at the time of the test was 75.7 ± 1.4 years with extremes between 75 and 91 years (75.3 ± 0.3 years in the DRS groupvs76.9 ± 2.3 years in the RGP group,P=0.00001).In the DRS group,98.2% were 75 years old at the time of the test and 1.8%were 76-80 years.In the RGP group,49.8% were 75 years old at the time of the test,40.0% were 76-80 years and 10.2% were > 80 years (P= 0.00001).The proportion of females was not significantly different between DRS (56.5%) and RGP (56.0%,P=0.52).
Previous behavior in the CRCSP
Seventy-nine point five percent of this population (76.9% of the 13442 DRSsvs86.3%of the 5262 RGPs,P= 0.60) had an anteriority,i.e.at least one previous invitation in the CRCSP.Among these 14875 Elderly_75 with an anteriority (10336 in DRS and 4539 in RGP),12678 had at least one previous screening test between 50 and 74 years old(9119 in DRS and 3559 in RGP) and they participated in 73.6% (77.2% in DRSvs65.4%in RGP,P= 0.00001) of the campaigns to which they were solicited.Average number of this previous solicitations was 2.5 ± 1.3 (2.4 ± 1.2 in DRSvs2.7 ± 1.3 in RGP,P=0.00001).11.8% of the Elderly_75 with an anteriority never participated in a previous CRCSP campaign (9.1% in DRSvs18.6% in RGP,P= 0.00001) and 9.3% had a reported history of colonoscopy (8.0% DRSvs12.1% RGP,P< 0.001).Only 1.9% (1.7% in DRSvs2.1% in RGP,P= 0.1) had a reported history of NLAI or sent previously a form indicating their refusal to participate in the CRCSP.The frequency of participation in previous campaign and the results of previous tests by campaign year are summarized in Table 2.The proportion of Elderly_75 with a previous positive test in CRCSP among these with an anteriority was 1.1% (200 Elderly_75/18704).This proportion was higher in RGP (1.1% in DRSvs2.8% in RGP,P= 0.00001).Whatever the source of the test and the year of screening,the frequency of participation in previous campaign was at least 60.0%.Peoples who performed the test under recommendation in 2012 were less regular in the CRCSP than those who performed the test the same year,in a context of DRS (Figure 1).Before 2010,the screening test was performed mostly by people without any anteriority (1339 out of 1721 Elderly_75 in 2009) in the CRCSP or having never participated in a campaign (157/1721 tests in 2009).From 2011 to 2017,the test was mostly performed by people who participated in at least 70% of campaigns.
CRC fecal screening test completion after age 74
Overall,3.7% (3.7% in DRSvs3.7% in RPD,P= 0.79) of the 18995 tests performed were positive (Table 3).The proportion of the tests that could not be analyzed and not restarted was 13.2%.For these unanalyzed tests,the reason was age-related in 78.0%of cases,related to the laboratory's refusal to analyze the test of people aged ≥ 77.18.0% of the 366 Elderly_75 with lesions had no anteriority in the CRCSP and 10.4%had never participated.Reported colonoscopy completion rate was 81.3%.For those 575 people with reported colonoscopy,no complication was listed.124 Low-riskpolyps,159 High-risk-polyps,13 Unspecified-polyps and 70 CRCs were detected,with an average neoplasia’s PPV estimated at 0.64.This PPV varied from 0.46 (16 neoplasia out of 35 colonoscopy) in 2008 to 0.67 in 2017 (40 neoplasia out of 60 colonoscopy) (Table 4).The neoplasia detection rate was 19.3 per 1000 Elderly_75 screened and the CRC detection rate was estimated at 3.7 per 1000 Elderly_75screened.An increased detection rate (all neoplasia) was observed after the immunochemical test introduction in 2015 (Table 5).The mean age at neoplasia diagnosis was 75.7 ± 1.2 years (75.2 ± 0.2 years in DRSvs77.1 ± 1.8 years in RGP,P<0.001).This mean age was 75.4 ± 0.7 years when the lesion was a low risk polyp,75.4 ±0.5 years when it was a high-risk polyp and 77.0 ± 2.1 years when it was a CRC.

Table1 Total tests performed in the ten districts and part of tests performed by elderly aged ≥ 75 years (elderly ≥ 75),by year of campaign
DISCUSSION
Few results of CRC fecal screening in elderly are available.This study present results of out of recommendation screening in 18704 elderly over 74 years of age.The results observed appear to be beyond expectations.Indeed,the proportion (3.7%) of positive tests remains significantly higher than that found (2.9) in these districts in the same period or that usually found (2.6%) in the CRCSP program[20].In the national program,reported colonoscopy completion rate after a positive test was 76.9% with approximately major incidents,including perforation in 3 in 1000 colonoscopies[20].In addition to a similar even higher rate of colonoscopy completion observed in this study (81.3%),no major incident was recorded in this elderly population.In France,the detection rate of CRC was estimated at 1.6/1000 in CRCSP[20],which is only half of the rate observed in this study.Certainly,the high detection rate observed could be explained,at least in part,by age.Indeed,the increase in the incidence of CRC with age has been well documented[1,22,23].Between 40 and 80 years of age,the incidence doubles almost every ten years[24]and 45% of CRCs are diagnosed in people aged at least 75 years in Burgundy[16].In this population,CRC were diagnosed on average age at 77 years.Considering these findings,it could be argued that extending the duration of CRCSP in healthy people up to 80 years,could allow the screening of the many cases that occur after the exclusion of the Elderly_75 from CRCSP.
The sample described in this analysis consisted mainly of people regularly invited by the local cancer screening managing center with delayed answer.Although the age group concerned by the CRCSP is 50 to 74 years old,the logistic approach implemented for the last invitation challenges this approach.Indeed,people receive their last invitation until the eve of the 75th birthday.This timing inevitably has the consequence of carrying out a screening test beyond the extreme ages recommended in CRCSP.
The motivation of people previously devoted in the CRCSP,to continue the screening after 74 years has been previously discussed and ending screening at 75 years is a real ethical issue[25].Previous modeling studies have recommended screening up to 82 years,however,heterogeneity of the Elderly_75 population limit this implementation[14,15].Indeed,in addition to the fact that the gain in years of life remains very modest,heterogeneity of the population with both healthy subjects and subjects in precariousness or with comorbidities makes it difficult to choose the type of appropriate screening[25].The United States Preventive Services Task Force advocated screening for CRC in healthy people up to age 84.Beyond this age,it suggested that the disadvantages of screening outweigh profits[22,26].
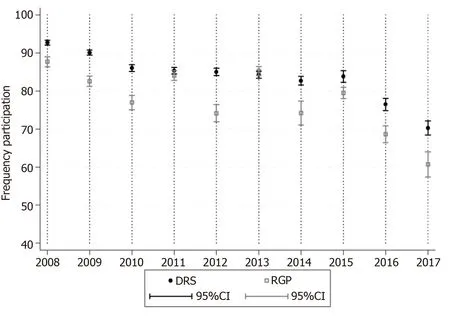
Figure1 Frequency of participation in previous campaigns,by circumstances and by screening year.
In order to sustain the CRCSP extension after 74 years,the availability of the medical profession must be acquired for medical monitoring and a continuous evaluation of the disadvantages and benefits of screening.It has been documented that the adherence of the GP is a determining factor in the acceptability and effectiveness of a screening campaign[27].Although the inequalities in access to cancer care are still visible in France[28,29],the results of this study show the possible availability of GPs to do a shared decision making process with patients regarding the pros and cons,and individualized risk assessments.Indeed,more than a quarter of the test were performed under medical recommendation which would testify not only an adherence of GPs but especially their concern for the follow-up of patient excluded from CRCSP.However,two major hypotheses could explain the test delivery to the Elderly_75 by the GPs.The hypothesis of a catch-up for the less regular persons in the CRCSP between 50 to 74 years,is concordant with the low frequency of participation in previous campaign of the people having performed a test after provider ordered recommendation (compared to the DRS).It is not excluded that GPs also use the screening test as an additional means of diagnosis.The bond in Elderly_75 participation after FIT introduction (in 2015),which is more sensitive and more userfriendly (only one sample) is also an essential point to be mentioned.
The proportion of non-analyzable tests remains abnormally high,especially among those who have taken the test under provider recommendation and after the introduction of FIT.Indeed,the proportion of non-analyzable tests was 1.6% in the CRCSP[19,20].When we subtract these numerous cases related to the refusal of the laboratory,the elderly could have a rate of non-analyzable tests lower than that observed in the CRCSP.The fundamental question with this main reason could be:"How many cancers have not been detected because of this age-based refusal of the person who made the tests”? The answer to this question is predicted by the high incidence of CRC (0.6/1000 Person-years) among people performing their last screening tests (between 70 and 74 years) in the CRCSP[23].
The study sample consisted mainly of 83.4% of tests performed at the age of 75,which could lend interpretation almost exclusively to this age.In addition,outside of the hypotheses evoked,the study could not bring more precise details on the real circumstances of realization of the test after 74 years.Indeed,a major concern regarding the RGP group is the possible self-selection bias:The considered population could have been motivated to participate in the screening by high risk factors or symptoms.In this group,screening test could have been used as a diagnostic tool.However,performing a colonoscopy after a positive screening test is a classic pattern in the French organized screening program.Certainly,the obtained results do not provide enough evidence on the benefits of screening in this age group,i.e.decrease in mortality from CRC if screening would be recommended above the currently accepted age limit.The results could,however,constitute a starting point (or even a reference) for a possible experimentation of the screening program for CRC in the elderly,in France.
In conclusion,despite a regulatory framework that is not favorable to their participation in CRCSP campaigns,a motivation to continue CRCSP after 74 years ofage was observed.To optimize CRC fecal screening for these Elderly_75,in addition to existing communication tools,the implementation of other means to better select patients and minimize the proportion of non-analyzable tests could be beneficial.The motivation to participate including the high colonoscopy participation rates and the high proportion of screened lesions demonstrate eloquently that the lengthening of the follow-up period in a screening program,up to about 80 years of age,could make it possible to detect many cases that occur after the exclusion of Elderly_75 from CRCSP.In a period of implementation of proposals for improving national program of CRCSP,it seems necessary to feed the debate on screening of the elderly to alert decision-making bodies.More in-depth studies on the feasibility of organized screening in Elderly_75 seem necessary to confirm or not,the current screening age limit.

Table2 Distribution of 18704 elderly aged ≥ 75 years,according to the test performing contexts and history in Colorectal Cancer Screening Program,by year of campaign
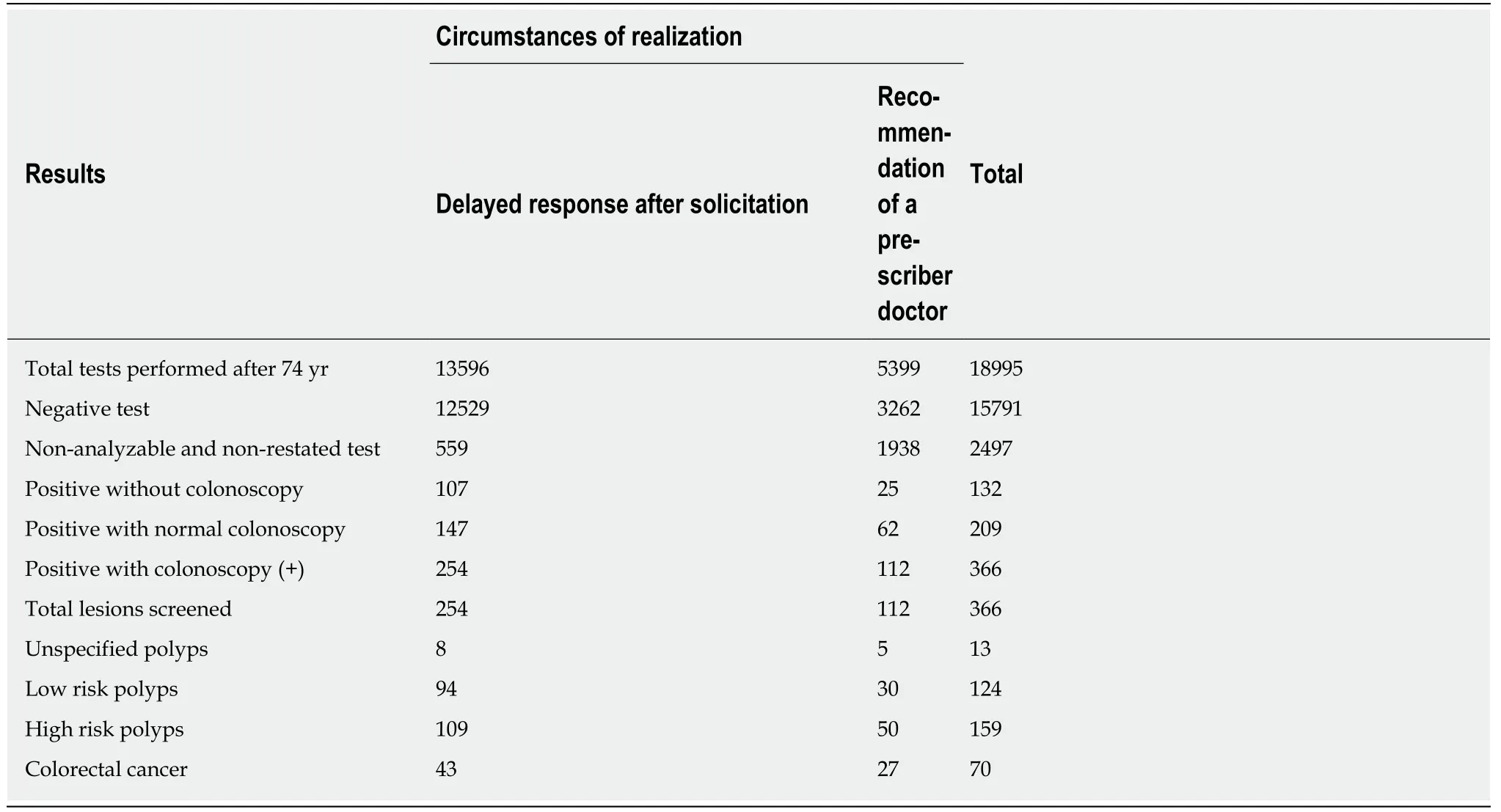
Table3 Distribution of the 18995 tests performed by elderly aged ≥ 75 years,according to the circumstances of realization (lt was about the circumstances of the first test for people who performed at least 2 tests after 74 years) and the results of the test

Table4 Distribution of 18995 tests performed by elderly aged ≥ 75 years (elderly ≥ 75),according to the results of the test and year of screening
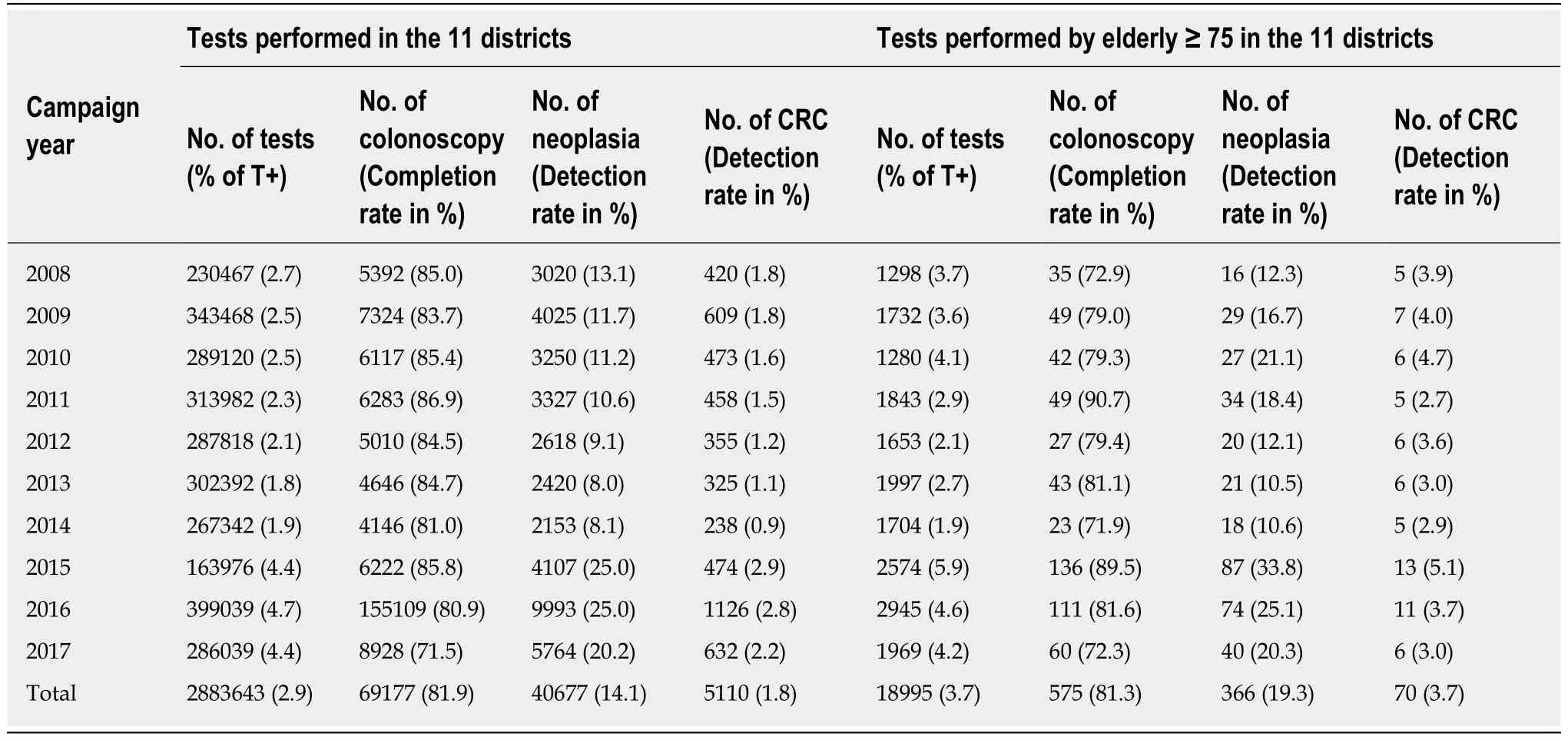
Table5 Colorectal cancer detection rate in the 11 districts and part of tests performed by elderly aged ≥ 75 years (elderly ≥ 75),by year of campaign
ARTICLE HIGHLIGHTS
Research background
In France,as in other countries,the Colorectal Cancer (CRC) Screening Program (CRCSP) does not include people aged ≥ 75 years,despite the high incidence of CRC after 74 years and the constant increase in life expectancy since 2000.Indeed,elderly patients aged at least 75 years old(Elderly_75),represent 45% of CRC incidence.To date,there is little evidence to justify stopping CRC screening at 74 years of age.
Research motivation
In this period of implementation of the proposals for reform of the National CRCSP,our motivation was to feed the debate on the problem of screening in the elderly,in order to alert the decision-making bodies.By noting that in each French district,the sporadic participation of Elderly_75,out of the national CRCSP’s recommendation,is recorded every year.
Research objectives
Our objective was to describe th e sources and outcomes of these screening test performed out of recommendation.Indeed,in the absence of a CRC screening program involving this age group,the elderly and/or their attending physicians decide sporadic participation in the campaigns organized by the local cancer screening managing center.The analysis of these sources and outcomes could argue the need for the implementation of an experimental program on the benefits and risk of CRC screening after the age of 75 years.
Research methods
The study concerned 18704 Elderly_75 residing in eleven French districts (Ain,Doubs,Essonne,Haute-Saone,Hauts-de-Seine,Jura,Seine-Saint-Denis,Territoire-de-Belfort,Val-de-Marne,Vald'Oise,Yonne),having performed a CRC screening test between January 2008 and December 2017.
Research results
Of 18995 screening-tests were performed by these 18704 Elderly_75 at ages:75 (83.5%),76-80(13.4%) and > 80 (3.1%) years old.Elderly_75 performed the screening test in a circumstance of delayed response to a solicitation from the local cancer screening managing center (71.9%) or following a recommendation by a General Practitioner or other provider ordered (28.1%).The proportion (3.7%) of positive tests remains significantly higher than that found (2.9) in these districts in the same period or that usually found (2.6%) in the CRCSP program.It’s obvious that the high risk of colonoscopy complication after 75 years is a barrier to screening CRC in the elderly.With a reported colonoscopy completion rate estimated at 81.3%,this study recorded no complications.On reminder,in the national program,reported colonoscopy completion rate after a positive test was 76.9% with approximately major incidents,including perforation in 3 in 1000 colonoscopies.The neoplasia (124 Low-risk-polyps,159 High-risk-polyps,13 Unspecifiedpolyps and 70 CRCs) detection rate was 19.3/1000 Elderly_75 screened and the CRC detection rate was 3.6/1000 Elderly_75 screened.In this population,CRC were diagnosed on average age at 77 years.
Research conclusions
Despite a regulatory framework that is not favorable to their participation in CRCSP campaigns,a motivation to continue CRCSP after 74 years of age was observed.Considering these findings,it could be argued that extending the duration of CRCSP in healthy people up to 80 years,could allow the screening of the many cases that occur after the exclusion of the Elderly_75 from CRCSP.
Research perspectives
We are confident that more in-depth studies on the feasibility of CRC screening in Elderly are needed to confirm or not,the current age limit of screening at 74 years.Our perspectives converge in this direction because a pilot project for the implementation of CRC-screening after the age of 75,is currently in the process of identifying strategic and financial partners.One of the main objectives of this study will be to assess the risk associated with performing colonoscopy.Awaiting the implementation of this project,we intend to open the debate in France with the results of this study.
ACKNOWLEDGEMENTS
The authors are grateful to all staff (Comité Départemental Des Cancers -CDC93-,Office De Lutte contre Les Cancers -ODLC01-,Association pour le Dépistage des Cancers -ADECA-FC-,Prévention and Santé en Val-d’Oise -PSVO-,Association pour le Dépistage des Maladies Cancéreuses -ADMC91-,Association de dépistage organisé des cancers -ADOC94-,Association Icaunaise de Dépistage du Cancer-AIDEC-,Association pour le Dépistage Organisé des Cancers-ADK92-) for the good collaboration and the quality of the data analyzed;the authors are grateful to Aïcha Kallo (West Hertfordshire Hospitals NHS Trust,Watford,United Kindom) for the thorough editing of the manuscript and to all collaborators who took part in the final revisions.
猜你喜欢
上海师范大学学报·自然科学版(2022年3期)2022-07-11
现代电力(2022年2期)2022-05-23
建材发展导向(2021年22期)2022-01-18
山东建筑大学学报(2021年6期)2021-12-23
北京航空航天大学学报(2021年7期)2021-08-13
建材发展导向(2021年11期)2021-07-28
铁道建筑技术(2021年4期)2021-07-21
阅读与作文(英语初中版)(2020年10期)2020-11-06
汽车实用技术(2018年19期)2018-10-22
宇航学报(2017年5期)2017-06-15
 World Journal of Gastrointestinal Oncology2019年9期
World Journal of Gastrointestinal Oncology2019年9期
- World Journal of Gastrointestinal Oncology的其它文章
- Advancements and challenges in treating advanced gastric cancer in the West
- Premalignant lesions and gastric cancer:Current understanding
- Current status of adjuvant chemotherapy for gastric cancer
- Tumor progression-dependent angiogenesis in gastric cancer and its potential application
- MicroRNA-331 inhibits development of gastric cancer through targeting musashi1
- Correlation between invasive microbiota in margin-surrounding mucosa and anastomotic healing in patients with colorectal cancer