
Therapeutic effect of heat-sensitive moxibustion plus medications for senile osteoporosis and its effect on serum BMP-2 and OPG levels
2020-06-22 09:51LiJuan李娟LiuGuiping刘桂平
Li Juan (李娟),Liu Gui-ping (刘桂平)
1Lin'an District People'sHospitalof Hangzhou,Zhejiang Province,Hangzhou 311300,China
2Chun’an OrthopedicHospital of Hangzhou, Zhejiang Province,Hangzhou 311700,China
Abstract
Keywords:MoxibustionTherapy;MoxaStick Moxibustion;Heat-sensitiveMoxibustion;Osteoporosis; Aged;Bone Density;Bone Morphogenetic Protein-2;Osteoprotegerin
Senileosteoporosis (SOP) generally occursafter the ageof 70 yearsold.It isametabolic bonedisorder causedby boneformationandbone destruction and characterizedby pain,spinaldeformity,andbrittle fracture[1].Thepain,deformity,andcomplications causedby SOP cansignificantly reducethepatient's quality of life.Brittlefractureisaseriouscomorbidity of SOPand a maincauseof disability anddeathinelderly patients[2].Studies have shownthat theprevalence of osteoporosis in people over 60 years old in 2010-2016 wasas highas 36%,significantly higher thanthe prevalence between 2002 and 2005[3-4]. In response to SOP, the current main treatments are drugs that inhibit boneresorption(bisphosphonates),stimulate bone formation (parathyroid hormones), and promote bone mineralization(calcium,vitaminD3)[5].Duetothe obvious side effects such as gastrointestinal reactions andnephrotoxicity,andthehighcost of drugs,the patient's medication compliance is not high, which has limited the clinical application of many drugs[6].
Moxibustionisbasedonsyndromedifferentiation and holistic concept. It is a safe, effective, economical,and convenient external therapy in traditional Chinese medicine.It acts tobalanceyinandyang,unblock meridians, and regulate organs. Moxibustion is widely used for knee joint arthritis, frozen shoulder, and other degenerative bone and joint diseases[7]. There are few studies on the clinical efficacy of moxibustionin the treatment of SOP and its mechanism in clinical efficacy.Therefore, this study usedheat-sensitive moxibustion combined with medicine to treat SOP and observed its effectontheserumbonemorphogenetic protein-2(BMP-2) and osteoprotegerin (OPG) levels.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Western medicine diagnostic criteria
Conformed to the diagnostic criteria of SOP[8]: bone mineral density (BMD) measured by dual-energy X-ray absorptiometry, T value ≤-2.5 SD.
1.1.2 Traditional Chinese medicine (TCM) syndrome differentiation criteria
Met the syndrome differentiation criteria for kidney deficiency and blood stasis[9]. The main symptoms were tingling in the lumbar spine, and the soreness in ankles and knees; other symptoms including atrophy of the lower extremities,difficultwalking,tinnitus,apale tongue, and a thready, hesitant pulse.
1.2 Inclusion criteria
Met theabove-mentionedWesternmedicine diagnostic criteriaand TCMsyndromedifferentiation criteria; aged70-85 years, female patients hadbeen menopausalfor more than20 years;nointerfering drugs had been used in the past 3 months; the patients voluntarily participated with informed consent.
1.3 Exclusion criteria
Patients withfragility fractures;thosewhowere allergic to thedrugsinthistrial;skinruptureand infectionat acupuncturepointstobetreatedwith heat-sensitive moxibustion; accompanied by kidney and other serious diseases, or unconsciousness, unable to cooperate with the research.
1.4 Rejection and shedding criteria
Serious adverse reactions occurred; those who took the initiative to withdraw from the trial; those who did not follow the doctor's instructions during treatment;those who lacked data that affected the statistics.
1.5 Statistical methods
The SPSS 20.0 statistical software was used for data analysis.Themeasurementdataweretestedfor normality first. If conforming to the normal distribution,it would be expressed as mean ± standard deviation(±s). Theindependent samplet-test wasused for between-group comparison, and the pairedt-test was used for intra-group comparison. Non-parametric test was used to analyze data that didn’t conform to the normaldistribution.Thenon-rankingcounting data adoptedChi-squaretest.P<0.05indicatedthat the difference was statistically significant.
1.6 General data
A total of 70 SOP patients were selected between January 2018 and May 2019 in Lin'an District People's Hospital of Hangzhou, Zhejiang Province and Chun'an Orthopedic Hospitalof Hangzhou,Zhejiang Province.According to the random number table method and the sequenceof patients'hospitalstay,patientswere randomly dividedinto anobservationgroupanda control group, with 35 cases in each group. During the treatment, neither group had patients dropout. There were nosignificant differences ingender,age,and duration of disease between the two groups (allP>0.05).See Table 1 for details.
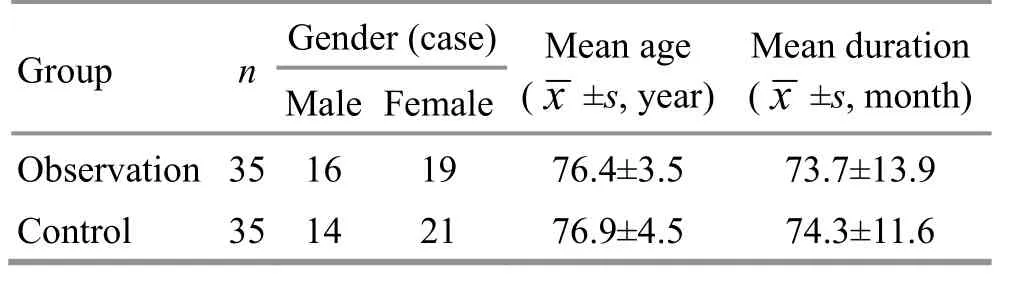
Table 1.Comparison of general data betweenthe two groups
2 Treatment Methods
2.1 Control group
Oral medications were given to participants. Calcitriol capsules (China Food and Drug Administration approval number:J20050021,RochePharmaceuticalCo.,Ltd.,China), 0.25 μg/time, twice a day; calcium carbonate D3tablets (China Food and Drug Administration approval number: H10950029, Wyeth Pharmaceutical Co., China),600 mg/time, twice a day; for 3 consecutive months in total.
2.2 Observation group
The patients in the observation group received heat- sensitivemoxibustiontreatment basedonthe same medications treatment as in the control group.
Points: Bilateral Geshu (BL 17), Shenshu (BL 23) and Yaoyangguan (GV 3).
Methods:Hwato brandmoxasticks of 1.8cmin diameter and 20 cm in length (manufactured by Hanyi Airong Factory, China) were selected. The procedures of heat-sensitivemoxibustionare asfollows[10].The patient took a prone position and exposed the points.First step was to detect the heat-sensitive points. Took circling or mild moxibustion with a moxa stick near the points, keeping a 3-5 cm distance between the ignited moxa stick and the skin. When the patient felt heat- sensitivephenomenasuchasheat penetrationor spreading or conduction, local heat without distant heat,non-thermalsensation,it meantthisistheheatsensitivepoint; after finding the heat-sensitivepoint,the doctor continued with mild moxibustion until the disappearance of the heat-sensitive phenomena, about 10 min for each point. Repeated the above procedures untiltheselectedpointswerecompleted.The treatmentwasdoneevery other day for atotalof 3 months.
Medicationtreatment:Samemedications,dosage,and course of treatment as in the control group.
3 Therapeutic Efficacy Observation
3.1 Observation items and testing indicators
Before and after treatment, the visual analog scale(VAS)and theOswestry disability index (ODI)scores were evaluated, and the bone mineral density (BMD)values of the lumbar spine (L2-L4) and left femoral neck of the participants were measured, and serum BMP-2 and OPG levels of the patients were detected.
3.1.1 VAS score
VAS was used to assess the patient's pain level. The score range is from 0 to 10 points, 0 means no pain, and 10 represents the most unbearable pain[11]. The higher the score, the more severe the pain.
3.1.2 ODI score
The participants completed the ODI questionnaire to evaluate the impact of low back pain on their daily life.Thehigher thescore,themoreseverethe dysfunction[12].3.1.3 BMD value
TheBMD values of the participants'lumbar spine(L2-L4)andleft femoralneck weremeasuredwitha Hologic bone densitometer. The BMD unit was g/cm2.3.1.4 Detection of the serum BMP-2 and OPG levels
Thefasting venousbloodof theparticipantswas drawn in the morning. The levels of serum BMP-2 and OPGwere determinedby enzyme-linkedimmunesorbent assay (ELISA).
3.2 Results
3.2.1 Comparison of the VAS score
Before treatment, there was no significant difference in the VAS scorebetweenthe two groups (P>0.05).After treatment, the VAS scores of the two groups were lower than those before treatment (bothP<0.05), and the VAS score of the observation group was significantly lower than that of the control group (P<0.05). See Table 2 for details.
Table 2.Comparison of the VASscorebetween thetwo groups( ±s, point)
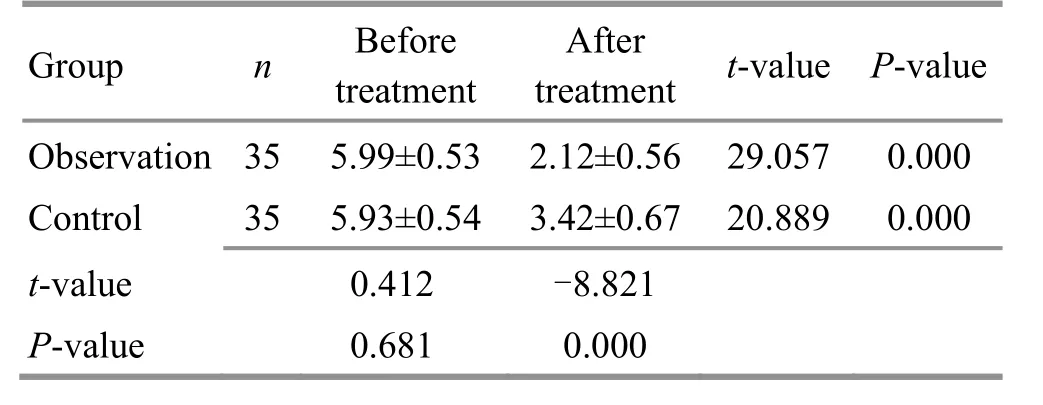
Table 2.Comparison of the VASscorebetween thetwo groups( ±s, point)
GroupnBefore treatment After treatment t-value P-value Observation 355.99±0.532.12±0.5629.0570.000 Control355.93±0.543.42±0.6720.8890.000 t-value 0.412-8.821 P-value0.6810.000
3.2.2Comparisonof the ODIscore
Before treatment, the ODI score of the two groups were not statistically different (P>0.05). After treatment,the ODI scores of the two groups were lower than those before treatment (bothP<0.05), and the ODI score in theobservationgroupwaslower thanthat inthe control group (P<0.05). See Table 3 for details.
Table 3.Comparison of the ODI score betweenthe two groups( ±s, point)
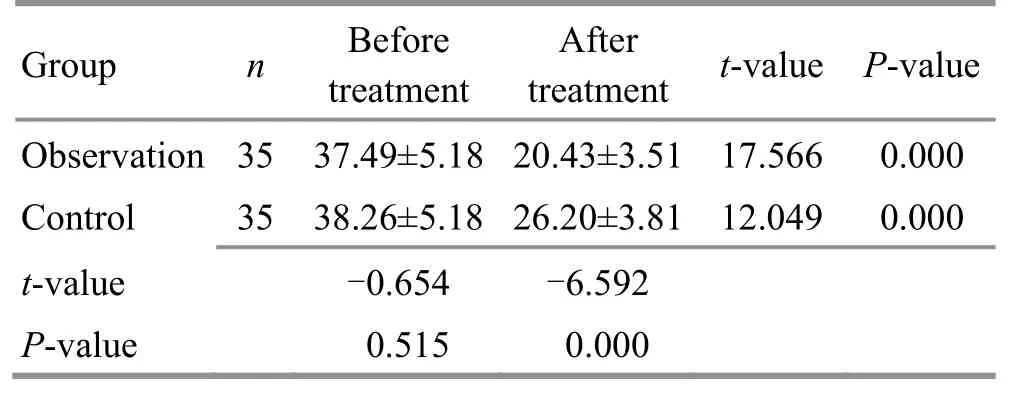
Table 3.Comparison of the ODI score betweenthe two groups( ±s, point)
GroupnBefore treatment After treatment t-value P-value Observation 3537.49±5.1820.43±3.5117.5660.000 Control3538.26±5.1826.20±3.8112.0490.000 t-value -0.654-6.592 P-value0.5150.000
3.2.3Comparisonsof BMDvalues
Beforetreatment,theBMDvalues of thelumbar spine(L2-L4) andleft femoralneck between the two groupswerenotstatistically different (bothP>0.05).After treatment, the BMD values of the lumbar spine(L2-L4)andleftfemoralneck inbothgroups were significantly higher thanthosebeforetreatment(allP<0.05), and the BMD values of the lumbar spine (L2-L4)and left femoral neck in the observation group were higher than those in the control group (bothP<0.05).See Table 4 for details.
3.2.4Comparisonsof theserumBMP-2andOPG levels Before treatment, the serum BMP-2 and OPG levels of the two groups were not statistically different (bothP>0.05). After treatment, thelevels of serumBMP-2 and OPG in the two groups were significantly higher than those before treatment (allP<0.05), and the serum BMP-2 and OPG levels in the observation group were higher than those in the control group (bothP<0.05).See Table 5 for details.
Table 4.Comparisonsof the BMDvaluesbetweenthe twogroups( ±s,g/cm2)

Table 4.Comparisonsof the BMDvaluesbetweenthe twogroups( ±s,g/cm2)
Groupnlumbar spine(L2-L4)Left femoral neck Before treatment After treatment t-value P-valueBeforetreatment After treatment t-value P-value Observation 350.70±0.06 0.80±0.07 -5.3730.0000.44±0.030.57±0.05-11.2920.000 Control 350.71±0.06 0.75±0.05-3.0050.0050.45±0.030.50±0.02 -6.4550.000 t-value -0.1423.294 -0.4927.360 P-value0.8870.002 0.6230.000
Table 5.Comparisonsof the serumBMP-2and OPG levelsbetweenthe twogroups( ±s, pg/mL)

Table 5.Comparisonsof the serumBMP-2and OPG levelsbetweenthe twogroups( ±s, pg/mL)
GroupnBMP-2OPG Beforetreatment After treatment t-value P-valueBefore treatment After treatment t-value P-value Observation 3567.35±4.4683.86±3.66-16.5160.000200.83±25.34255.21±20.19-9.7650.000 Control 3564.45±4.9075.90±3.32-7.0840.000206.04±20.82232.57±28.06 -4.6810.000 t-value 0.9869.529-0.9393.874 P-value 0.327 0.0000.3510.000
3.2.5 Adverse reactions in the two groups
During thetreatment period,2cases of anorexia appearedinthecontrolgroup;1caseof dizziness occurredintheobservationgroup.Theadverse reactions were mild, untreated, and alleviated within a short period of time.
4 Discussion
The SOP is closely associated with age and hormone.Age directly affects thebonemineral content of the human body. After 40 years old, the bone mass starts to lose,andafter 65years old,thebonemass loses quickly[13]. With increasing age, the levels of androgens in men and estrogen in women gradually decrease, and their ability to inhibit parathyroid hormone decreases,resulting inanincreasednumber andviability of osteoclasts.Therefore,therate of bonedestruction exceeds the speed of bone tissue reconstruction, and finally SOPoccurs[14].Inaddition,nutrition,genetics,and life style factors (smoking, drinking, etc.) can induce andaggravateSOP[13].Studies inrecentyearshave found that BMP-2 and OPG play an important role in the occurrence, progression, and prognosis of SOP.
BMP-2isacytokineinthebonemorphogenetic protein family that strongly promotes bone formation.BMP-2canpromotetheproliferationof bonecells,induce thedifferentiationof mesenchymalcells into chondrocytesandosteoblasts,andpromotethe differentiation of osteoblasts. Studies have shown that BMP-2caninduceosteogenic precursorcells to differentiateintoosteoblasts andincreasethe expression of alkalinephosphatase,osteopontin, and other osteogenic genes[15]. Reduced activity of BMP-2 cancausesevereosteoporosis-like symptoms;the serum BMP level of patients with osteoporosis is also lower comparedwithnormalpeople[16].E40071can up-regulateBMP-2,promoteSmad1/5/8 protein phosphorylation,andup-regulateRunx2protein expressionto promote stemcelldifferentiationand osteoblastformation[17].It canbeseenthat the decrease of BMP-2 level can induce SOP, and correcting the low levelof BMP-2expressionhasbecomea potential target and research hotspot for the treatment of SOP.
OPG is synthesized and secreted by osteoblasts and bone marrow stromal cells. It is an important member of thetumor necrosisfactor family.Asanegative regulator of osteoclasts, OPG can inhibit the activity of matureosteoclastsandstimulatetheapoptosisof osteoclasts.OPGis animportant proteinof the OPG/RANGL/RANK pathway inosteoclasts.OPG competitively binds to RANKL and prevents the binding of RANK to RANKL,thereby inhibiting osteoclast differentiationto promoteboneformationand maintainbonemass[18].Qiao S,et al[19]observeda significant decrease in the serum OPG level in elderly osteoporosis patients and healthy subjects, and found that the OPG level was positively correlated with bone formationindex andnegatively correlated withbone resorption index, but not with age. It can be seen that the decrease of OPG level may be one of the causes of SOP.
SOP falls under the category of bone flaccidity and bone Bi-Impediment in Chinese medicine. In TCM, SOP mainly affects the kidney,andis alsorelated to the spleen and liver. The kidney is the congenital foundation,andresponsible for bone growth and generating the bone marrow. When kidney essence is sufficient, the boneis healthy;if kidney essencedeclines,bone marrow will lose, resulting in brittle bones. Blood stasis isboththepathologicalbasisandproductof SOP.Kidney qi deficiency may cause blood stasis; exogenous pathogenic factors may obstruct meridians and cause blood stagnation; SOP has a long duration and can lead to blood stasis. Blood stasis may cause pain; long-term malnourishment of bones, tendons, muscles, marrows and bones may induce and aggravate SOP. Therefore,kidney deficiency andbloodstasisaretheprimary cause of SOP[20]. As a result, the treatment strategies are to tonify kidney,promotebloodcirculation,and resolve blood stasis.
Heat-sensitivemoxibustionis a new and improved moxibustionmethodby stimulating heat-sensitive points and applying saturated moxibustion. According to Professor Chen Ri-xin, when the body is in the state of sub-health or disease, the points can be thermally sensitized. At this time, thecorresponding pointsof moxibustion will appear diathermy, heat transfer, heat expansion,heat feeling from thedeeparea,heat in distance,andother specialheat sensitive phenomena[10]. Heat-sensitive moxibustion focuses on stimulating the meridians and collaterals of the points,and emphasizes qi reaching the point of disease, so as toachievethepurposeof ‘sensitizing thesmall stimulationof thepoints andtriggering thelarge response of thebody’,toimprovethemoxibustion effect.At thesametime,thewarmthproducedby heat-sensitive moxibustion can unblock meridians and collaterals; the warmth can tonify organs and tissues.They complement with each other, so as to exert the effects of unblocking meridians,reinforcing the deficiency andpromoting bloodcirculationand resolving blood stasis. Geshu (BL 17), Shenshu (BL 23)and Yaoyangguan (GV 3) were selected in this research.Geshu(BL 17)isone of theEight InfluentialPoints,wherebloodgathers.It cannourishbloodand harmonize the Ying-nutrient, regulate qi to soothe the chest, promote blood circulation and unblock meridians.Geshu (BL 17) can unblock and replenish at the same timeandisanimportant point for blooddiseases.Shenshu (BL 23) is the Back-Shu point of the kidney. It can tonify kidney yang, warm the kidney and absorb qi.Yaoyangguan (GV 3) is a point of the Governor Vessel,wherestorestheYuan-Primary qiinthelower Jiao (energizer). The warmth of the moxibustion can directly go into the abdomen and distribute in Zang-fu organs. It can tonify the kidney and the low back, warm yang and replenish qi, and unblock meridians.
The results of this study showed that after treatment,the VAS score and ODI score of both groups decreased,and the observation group was significantly lower than the control group. The BMD values, serum BMP-2 and OPG levels of both groups were significantly increased after treatment,andthevaluesof theobservation group were higher than those of the control group. The resultsshowedthat heat-sensitivemoxibustionplus medicationscouldsignificantly relieveSOPpatients'pain,improvedysfunctionandincreaseBMD,which may berelatedto theimprovementsof theserum BMP-2 and OPG levels.
Received:26 September 2019/Accepted:31October 2019
猜你喜欢
学与玩(2022年2期)2022-05-03
Plasma Science and Technology(2021年8期)2021-08-05
今日农业(2020年23期)2020-12-15
文史春秋(2019年10期)2019-12-21
林业与生态(2019年2期)2019-04-12
火花(2018年10期)2018-11-01
商情(2017年26期)2017-07-28
高中生学习·高二版(2016年9期)2016-05-14
名作欣赏(2011年16期)2011-08-15
 Journal of Acupuncture and Tuina Science2020年3期
Journal of Acupuncture and Tuina Science2020年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic observation on lung-clearing and spleen-strengthening tuina in children with exogenous cough
- Therapeutic efficacy observation on auricular point sticking therapy for cardiac syndrome X in women
- Effects of electroacupuncture plus drug anesthesia on pain and stress response in patients after radical surgery for stomach cancer
- Clinical observation on heat-sensitive moxibustion plus lactulose for postoperative constipation of mixed hemorrhoid due to spleen deficiency
- Efficacy of transcutaneous electrical acupoint stimulation (TEAS) for menopausal insomnia and its effect on serum hormone levels
- Therapeutic observation of manipulation plus exercise therapy in treating upper crossed syndrome postures of primary school students