
晚期胃癌二线化疗的研究现状
2014-09-12 11:22张慧卿综述万以叶审校
实用癌症杂志 2014年1期
张慧卿综述 何 波 万以叶审校
权威数据表明,2008年全球仍有738 000名患者死于胃癌,在肿瘤相关性死亡中排第二位[1-2]。手术是唯一可能根治胃癌的治疗手段,然而,超过2/3的患者在诊断胃癌时已是晚期,失去了手术机会;而实行根治性手术切除的患者中,仍有70%以上出现复发或转移[3]。目前,晚期胃癌的主要治疗方法是化疗,而有关胃癌化疗的大型研究绝大多数关注在一线治疗[4-6]。一线化疗无效或疾病进展的患者部分需要接受二线治疗,据报道,15%~40.8%的患者接受了二线化疗[7-8]。
1 二线化疗获益的临床证据
胃癌是化疗相对敏感的肿瘤,晚期胃癌一线化疗的作用已经明确,能延长患者生存,提高生活质量[9]。胃癌二线化疗已有一段时日,在我国更是非常普遍。但既往文献报道均为Ⅱ期临床试验研究或回顾性研究,缺乏患者获益的高级别证据[10]。最近,两项Ⅲ期临床试验一致证实,与最佳支持治疗(best supportive care,BSC)相比,单药二线化疗能显著延长晚期胃癌患者的总生存时间,为临床晚期胃癌二线化疗的开展提供了依据。
2011年10月,德国Arbeitsgemeinschaft Internistische Onkologie(AIO)报道了伊立替康二线化疗与BSC治疗晚期胃癌的随机对照研究数据,与最佳支持治疗组相比,伊立替康组的中位生存期从2.4个月延长至4.0个月,死亡风险降至0.48[11]。尽管该试验因入组缓慢提前关闭,导致样本量较小,但这是首个比较二线化疗与BSC治疗晚期胃癌的Ⅲ期临床研究,且获得了阳性结果,为晚期胃癌二线化疗提供了确凿的临床证据。也正是在2011年,NCCN指南引入了晚期胃癌二线化疗的概念。
2012年5月,另外一项多中心Ⅲ期临床研究的结果发表在JCO杂志上,这是由韩国学者Kang等牵头完成的[12]。他们共入组了PF方案(DDP+5-FU)化疗失败的晚期胃癌患者202例,其中对照组69例,给予最佳支持治疗;试验组133例,最佳治疗的同时,给予多西他赛(60 mg/m2第1天,每3周重复)或伊立替康(150 mg/m2第1天,每2周重复)单药化疗。结果显示,对照组与试验组不良反应相似,试验组的mOS显著延长(5.3个月vs 3.8个月),死亡风险明显降低,HR为0.657。
2 二线化疗疗效的影响因素
晚期胃癌二线化疗生存获益的数据相对较少,众多学者就二线化疗疗效的影响因素进行了深入探索,以筛选出可能从治疗中获益的群体,从而避免过度治疗,节约医疗资源。研究表明,BRCA1 mRNA、行为评分(PS)、一线化疗时疾病进展时间(TTP)、血红蛋白(HB)等可能是判断二线化疗是否有效的预测因子。
研究较为完善的是俄罗斯学者Kanagavel,他在筛选疗效预测因素的同时,建立了简单有效的预测模型[13]。他们回顾性研究接受二线化疗的晚期胃癌患者126例,多因素分析到3个独立预测因子:PS(0~1分或2分),HB(﹤100 g/L或≥100 g/L)和一线化疗时TTP(﹤或≥5个月)。通过这些预测因子建立了疗效预测模型,预后指数= PS (0或1) + Hb (0或2) + TTP (0或1),再根据预后指数大小将患者分为预后良好、预后中等和预后差3组,统计显示3组间的生存时间具有显著性差异(P=0.00001)(表1)。瑞士学者也筛查到与生存时间相关的3个变量:一线化疗时无进展生存期(PFS)≥36周,既往行胃癌根治术和CEA >6.5 μg/L[14]。Hasegawa等[15]的研究则表明,具备PS≥2分,二线化疗时血清白蛋白≤3.5 g/dl和一线化疗TTP≤170天中有2项或2项以上的患者可能无法从二线化疗中获益。另外,C反应蛋白水平升高(≥1.0 mg/dL)和发生骨、肝、腹膜转移也可能是二线化疗生存时间较短的影响因素[16]。
表1 不同风险组生存时间的比较 (n=126)
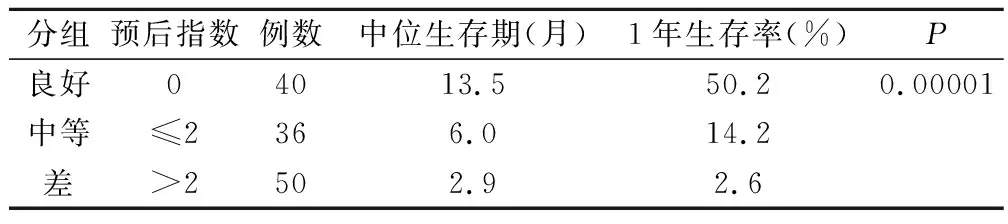
分组预后指数例数中位生存期(月)1年生存率(%)P良好04013.550.20.00001中等≤2366.014.2差>2502.92.6
值得注意的是,上述两项Ⅲ期临床研究的分层研究提示,晚期胃癌患者能否从二线化疗中获益与既往化疗疗效、血红蛋白水平、转移部位多少和化疗间歇期无关,而且PS(0~1 vs 2)也不是二线化疗总生存时间的确切影响因素[11-12]。
有学者尝试在分子生物学水平筛选晚期胃癌二线化疗的疗效预测因素,为个体化治疗胃癌推广科学依据。BRCA1 mRNA表达水平可预测晚期胃癌患者能否从含多西他赛的二线化疗方案中获益。南京大学附属鼓楼医院入组接受含多西他赛的二线化疗的患者59例,随访生存时间,RT-PCR检测胃癌组织BRCA1 mRNA表达,结果表明,BRCA1高表达患者的mOS为25.8个月,而低表达者仅为8.5个月,BRCA1低表达的患者死亡风险也明显更高(HR=2.49)[17]。P-糖蛋白(P-gp)过表达与胃癌细胞对化疗药物产生多药耐药密切相关,而P-gp的编码基因则是ABCB1。ABCB1基因多态性与晚期胃癌二线化疗的疗效可能相关。Shitara等[18]回顾性研究了接受二线化疗的晚期胃癌患者100例,检测基因位点ABCB1 3435 C>T,结果表达3435 CC基因型患者的PFS比3435CT/TT基因型更长(3.2个月 vs 2.2个月)。
3 二线化疗方案的选择
一线化疗无效或疾病进展的患者可能需要接受二线治疗,目前尚无治疗晚期胃癌的标准二线化疗方案。原则上,一线治疗未选取的药物,均可作为二线治疗方案考虑。对于接受胃癌根治术后的患者,若复发转移发生在辅助化疗结束1年以上,亦可以考虑重新应用辅助化疗方案。晚期胃癌的二线化疗应尽量选择可避免发生一线治疗过程中主要不良反应的方案,同时应格外注意保护患者的生活质量。
3.1 单药化疗
单药伊立替康或多西他赛的二线化疗均能使患者获益,孰优孰劣呢?Kang等[12]对接受二线化疗的患者进行亚组分析,发现多西他赛组和伊立替康组患者的总生存时间无明显差别,但伊立替康显示出更好的趋势(5.2个月vs 6.5个月)。这一结果与Hashimoto等的研究相同[16],为我们在临床工作中选择化疗方案提供了依据。
研究证实,紫杉醇和多西他赛在晚期胃癌的抗癌效果相近[19]。在日本,紫杉醇比多西他赛更多地应用于晚期胃癌。有学者比较了伊立替康和紫杉醇在二线化疗中的优劣性。2012年ASCO会议上,日本公布了Ⅲ期临床试验WJOG4007的部分数据,这是胃癌二线化疗药物首次头对头的比较[20]。该试验采用伊立替康(CPT-11 150 mg/m2第1天,第2周重复)或周剂量紫杉醇(wPTX,80 mg/m2第1、8、15天,每4周重复)二线治疗PF方案(DDP+5-FU)化疗失败的晚期胃癌患者223例,其中CPT-11组112例,wPTX组111例。主要研究终点为OS,预期结果是伊立替康组mOS优于紫杉醇组。结果显示,CPT-11组的中位OS为8.4个月,wPTX组为9.5个月(HR=1.132,95% CI,0.86-1.49;P=0.38);CPT-11组的中位PFS为2.3个月,wPTX组为3.6个月(HR= 1.14; 95% CI,0.88-1.49;P=0.33)。总有效率(ORR):CPT-11组为13.6% (12/88),wPTX组为20.9% (19/91)。最常见的3/4度不良事件为中性粒细胞减少(CPT-11组39.1% vs wPTX组 28.7%)、 贫血(30.0% vs 21.3%)、 食欲下降 (17.3% vs 7.4%) 以及乏力(12.7% vs 6.5%)。研究结果未达到预期目的,伊立替康方案不优于周剂量紫杉醇给药。
3.2 联合药物化疗
单药二线化疗在晚期胃癌的作用已经得到确立,有诸多学者对联合化疗的价值进行了探讨,报道的有效率在20%左右,但均为小样本量的Ⅱ期临床试验或者回顾性研究,且大多方案选择了含伊立替康和(或)紫杉类药物(表2)。
表2 晚期胃癌二线化疗的临床研究
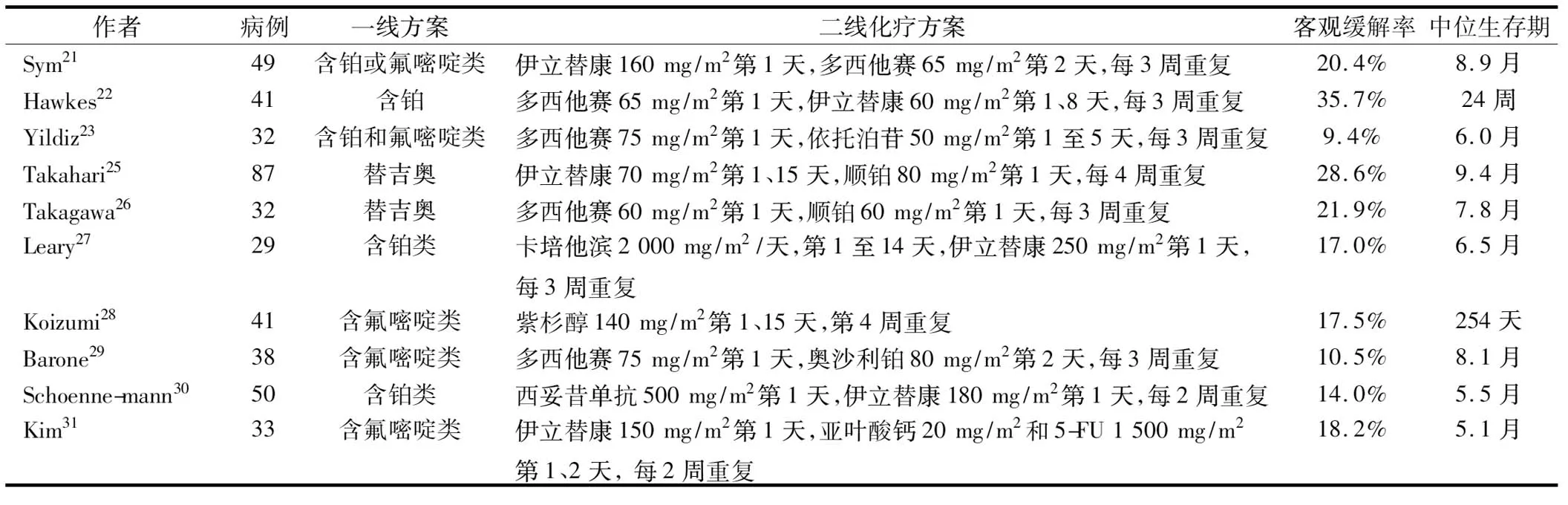
作者病例一线方案二线化疗方案客观缓解率中位生存期Sym 2149含铂或氟嘧啶类伊立替康160 mg/m2 第1天,多西他赛65 mg/m2 第2天,每3周重复20.4%8.9月Hawkes2241含铂多西他赛65 mg/m2 第1天,伊立替康60 mg/m2 第1、8天,每3周重复35.7%24周Yildiz2332含铂和氟嘧啶类多西他赛75 mg/m2 第1天,依托泊苷50 mg/m2 第1至5天,每3周重复9.4%6.0月Takahari2587替吉奥伊立替康70 mg/m2 第1、15天,顺铂80 mg/m2 第1天,每4周重复28.6%9.4月Takagawa2632替吉奥多西他赛60 mg/m2 第1天,顺铂60 mg/m2 第1天,每3周重复21.9%7.8月Leary2729含铂类卡培他滨2 000 mg/m2/天,第1至14天,伊立替康250 mg/m2 第1天,每3周重复17.0%6.5月Koizumi2841含氟嘧啶类紫杉醇140 mg/m2 第1、15天,第4周重复17.5%254天Barone2938含氟嘧啶类多西他赛75 mg/m2 第1天,奥沙利铂80 mg/m2 第2天,每3周重复10.5%8.1月Schoenne-mann3050含铂类西妥昔单抗500 mg/m2 第1天,伊立替康180 mg/m2 第1天,每2周重复14.0%5.5月Kim3133含氟嘧啶类伊立替康150 mg/m2 第1天,亚叶酸钙20 mg/m2 和5-FU 1 500 mg/m2 第1、2天, 每2周重复18.2%5.1月
伊立替康联合多西他赛二线治疗氟嘧啶或顺铂化疗失败的晚期胃癌,显示出良好的抗癌活性,但需要严格掌握给药方法和剂量。Sym等[21]入组氟嘧啶或铂类药物一线化疗失败的晚期胃癌患者49例,拟给予伊立替康160 mg/m2第1天+多西他赛65 mg/m2第2天,每三周重复的方案化疗,因不可接受的不良反应,剂量降低至伊立替康120 mg/m2,多西他赛50 mg/m2。结果RR为20.4%,mOS为8.9个月,mTTP为2.7个月。3/4级不良反应包括粒细胞减少 (90%)、粒细胞减少性发热 (50%)、腹泻 (10%),2例可疑的治疗相关性死亡。如果采用周剂量方案化疗,即伊立替康60 mg/m2第1、8天+多西他赛35 mg/m2,第1、8天,每3周重复,则疗效确切且不良反应较轻[22]。
ECF和DCF方案在晚期胃癌NCCN指南中是作为1类证据推荐使用的,在我们的临床实践中也最为常见。Yildiz等[23]采用多西他赛联合依托泊苷治疗ECF方案化疗失败的晚期胃癌32例,方案为多西他赛75 mg/m2第1天+依托泊苷50 mg/m2第1-5天,每3周重复。结果RR为9.4%,mOS为6个月,mPFS为3个月。3/4级毒性反应包括粒细胞减少(28.8%)、粒细胞减少性发热(18.8%)、恶心和呕吐(15.6%)。Sym等[24]回顾性研究FOLFIRI挽救性治疗PTX+DDP+5-Fu一线化疗失败的晚期胃癌131例,具有可测量病灶者97例,RR为12.3%,mTTP为2.2个月,mOS为6.2个月。
替吉奥是日本晚期胃癌一线化疗最常使用的药物。Takahari等[25]报道伊立替康联合顺铂二线治疗替吉奥耐药的晚期胃癌患者87例,给药方案为:伊立替康 70 mg/m2第1、15天+顺铂80 mg/ m2第1天,每4周重复,结果RR为28.6%,mOS为9.4个月,mTTP为4.3个月,1年生存率为34.6%。Takagawa等[26]采用多西他赛联合顺铂治疗替吉奥一线化疗失败的晚期胃癌32例,给药方案为:多西他赛 60 mg/m2第1天+顺铂60 mg/m2第1天,每3周重复。结果RR为21.9%,mOS为7.8个月,mTTP为4.0个月。
综上所述,紫杉类和伊立替康单药二线化疗能延长晚期胃癌患者的生命,改善生活质量,而且疗效无差别。目前,尚无足够证据支持二线化疗中联合用药的疗效优于单药的疗效,但从横向比较,联合化疗试验中患者的总生存时间比单药化疗更长,可能与入组患者的特征不同有关。二线化疗时,为避免不必要的痛苦和减轻医疗负担,选择可能获益的患者具有一定的现实意义。期待更多更大样本Ⅲ期临床试验的开展,从而建立晚期胃癌一线化疗失败后的标准挽救方案。
[1] Bertuccio P,Chatenoud L,Levi F,et al.Recent patterns in gastric cancer:a global overview〔J〕.Int J Cancer,2009,125(3):666-673.
[2] Jemal A,Bray F,Center MM,et al.Global cancer statistics〔J〕.CA Cancer J Clin,2011,61 (2):69-90.
[3] Macdonald JS.Gastric cancer--new therapeutic options〔J〕.N Engl J Med,2006,355(1):76-77.
[4] Ajani JA,Moiseyenko VM,Tjulandin S,et al.Quality of life with docetaxel plus cisplatin and fluorouracil compared with cisplatin and fluorouracil from a phase Ⅲ trial for advanced gastric or gastroesophageal adenocarcinoma:the V-325 Study Group〔J〕.J Clin Oncol,2007,25(22):3210-3216.
[5] Kang YK,Kang WK,Shin DB,et al.Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as first-line therapy in patients with advanced gastric cancer:a randomised phase Ⅲ noninferiority trial〔J〕.Ann Oncol,2009,20(4):666-673.
[6] Koizumi W,Narahara H,Hara T,et al.S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial):a phase Ⅲ trial〔J〕.Lancet Oncol, 2008,9(3):215-221.
[7] Cunningham D,Starling N,Rao S,et al.Capecitabine and oxaliplatin for advanced esophagogastric cancer〔J〕.N Engl J Med,2008,358(1):36-46.
[8] Lee J,Lim T,Uhm JE,et al.Prognostic model to predict survival following first-line chemotherapy in patients with metastatic gastric adenocarcinoma〔J〕.Ann Oncol,2007,18(5):886-891.
[9] Casaretto L,Sousa PL,Mari JJ.Chemotherapy versus support cancer treatment in advanced gastric cancer:a meta-analysis〔J〕.Braz J Med Biol Res,2006,39(4):431-440.
[10] Wesolowski R,Lee C,Kim R.Is there a role for second-line chemotherapy in advanced gastric cancer? 〔J〕.Lancet Oncol,2009,10(9):903-912.
[11] Thuss-Patience PC,Kretzschmar A,Bichev D,et al.Survival advantage for irinotecan versus best supportive care as second-line chemotherapy in gastric cancer--a randomised phase Ⅲ study of the Arbeitsgemeinschaft Internistische Onkologie (AIO) 〔J〕.Eur J Cancer,2011,47(15):2306-2314.
[12] Kang JH,Lee SI,Lim do H,et al.Salvage chemotherapy for pretreated gastric cancer:a randomized phase Ⅲ trial comparing chemotherapy plus best supportive care with best supportive care alone〔J〕.J Clin Oncol,2012,30(13):1513-1518.
[13] Kanagavel D,Pokataev IA,Fedyanin MY,et al.A prognostic model in patients treated for metastatic gastric cancer with second-line chemotherapy〔J〕.Ann Oncol,2010,21(9):1779-1785.
[14] Bohanes P,Courvoisier DS,Perneger TV,et al.Survival predictors for second-line chemotherapy in Caucasian patients with metastatic gastric cancer〔J〕.Swiss Med Wkly,2011,141:w13249.
[15] Hasegawa H,Fujitani K,Nakazuru S,et al.Optimal indications for second-line chemotherapy in advanced gastric cancer〔J〕.Anticancer Drugs,2012,23(4):465-470.
[16] Hashimoto K,Takashima A,Nagashima K,et al.Progression-free survival in first-line chemotherapy is a prognostic factor in second-line chemotherapy in patients with advanced gastric cancer〔J〕.J Cancer Res Clin Oncol,2010,136(7):1059-1064.
[17] Wei J,Costa C,Ding Y,et al.mRNA expression of BRCA1,PIAS1,and PIAS4 and survival after second-line docetaxel in advanced gastric cancer〔J〕.J Natl Cancer Inst,2011,103(20):1552-1556.
[18] Shitara K,Matsuo K,Ito S,et al.Effects of genetic polymorphisms in the ABCB1 gene on clinical outcomes in patients with gastric cancer treated by second-line chemotherapy〔J〕.Asian Pac J Cancer Prev,2010,11(2):447-452.
[19] Park SH,Lee WK,Chung M,et al.Paclitaxel versus docetaxel for advanced gastric cancer:a randomized phase Ⅱ trial in combination with infusional 5-fluorouracil〔J〕.Anticancer Drugs,2006,17(2):225-229.
[20] Ueda S,Hironaka S,Yasui H,et al.Randomized phase Ⅲ study of irinotecan (CPT-11) versus weekly paclitaxel (wPTX) for advanced gastric cancer (AGC) refractory to combination chemotherapy (CT) of fluoropyrimidine plus platinum (FP):WJOG4007 trial[abstr].J Clin Oncol,2012,30,(suppl; abstr 4002).
[21] Sym SJ,Chang HM,Kang HJ,et al.A phase Ⅱ study of irinotecan and docetaxel combination chemotherapy for patients with previously treated metastatic or recurrent advanced gastric cancer〔J〕.Cancer Chemother Pharmacol,2008,63(1):1-8.
[22] Hawkes E,Okines AF,Papamichael D,et al.Docetaxel and irinotecan as second-line therapy for advanced oesophagogastric cancer〔J〕.Eur J Cancer,2011,47(8):1146-1151.
[23] Yildiz R,Kalender ME,Dane F,et al.Docetaxel combined with oral etoposide as second-line treatment for advanced gastric carcinoma after failure of platinum- and fluoropyrimidine-based regimens〔J〕.J Oncol Pharm Pract,2010,16(3):173-178.
[24] Sym SJ,Ryu MH,Lee JL,et al.Salvage chemotherapy with biweekly irinotecan,plus 5-fluorouracil and leucovorin in patients with advanced gastric cancer previously treated with fluoropyrimidine,platinum,and taxane〔J〕.Am J Clin Oncol,2008,31(2):151-156.
[25] Takahari D,Shimada Y,Takeshita S,et al.Second-line chemotherapy with irinotecan plus cisplatin after the failure of S-1 monotherapy for advanced gastric cancer〔J〕.Gastric Cancer,2010,13(3):186-190.
[26] Takagawa R,Kunisaki C,Makino H,et al.Second-line docetaxel plus cisplatin for advanced gastric cancer showing resistance to S-1〔J〕.J Chemother,2011,23(1):44-48.
[27] Leary A,Assersohn L,Cunningham D,et al.A phase Ⅱ trial evaluating capecitabine and irinotecan as second line treatment in patients with oesophago-gastric cancer who have progressed on,or within 3 months of platinum-based chemotherapy〔J〕.Cancer Chemother Pharmacol,2009,64(3):455-462.
[28] Koizumi W,Akiya T,Sato A,et al.Second-line chemotherapy with biweekly paclitaxel after failure of fluoropyrimidine-based treatment in patients with advanced or recurrent gastric cancer:a report from the gastrointestinal oncology group of the Tokyo cooperative oncology group,TCOG GC-0501 trial〔J〕.Jpn J Clin Oncol,2009,39(11):713-719.
[29] Barone C,Basso M,Schinzari G,et al.Docetaxel and oxaliplatin combination in second-line treatment of patients with advanced gastric cancer〔J〕.Gastric Cancer,2007,10(2):104-111.
[30] Schoennemann KR,Bjerregaard JK,Hansen TP,et al.Biweekly cet-uximab and irinotecan as second-line therapy in patients with gastro-esophageal cancer previously treated with platinum〔J〕.Gastric Cancer,2011,14(3):219-225.
[31] Kim SH,Lee GW,Go SI,et al.A phase Ⅱ study of irinotecan,continuous 5-fluorouracil,and leucovorin (FOLFIRI) combination chemotherapy for patients with recurrent or metastatic gastric cancer previously treated with a fluoropyrimidine-based regimen〔J〕.Am J Clin Oncol,2010,33(6):572-576.
猜你喜欢
昆明医科大学学报(2021年8期)2021-08-13
肝博士(2021年1期)2021-03-29
宁夏医学杂志(2020年3期)2021-01-21
肝博士(2020年5期)2021-01-18
武警医学(2018年10期)2018-11-06
中成药(2017年3期)2017-05-17
当代化工研究(2016年6期)2016-03-20
中国继续医学教育(2015年1期)2016-01-06
西南军医(2015年1期)2015-01-22
中国中医药现代远程教育(2014年13期)2014-03-01
