
弥散加权成像单指数模型和体素内不相干运动(IVIM)模型对肺结节的诊断初探
2017-01-12 01:48周舒畅夏黎明王玉锦
华中科技大学学报(医学版) 2016年6期
周舒畅, 夏黎明, 王玉锦, 吴 维
华中科技大学同济医学院附属同济医院放射科,武汉 430030
弥散加权成像单指数模型和体素内不相干运动(IVIM)模型对肺结节的诊断初探
周舒畅, 夏黎明△, 王玉锦, 吴 维
华中科技大学同济医学院附属同济医院放射科,武汉 430030
目的 研究弥散加权成像(diffusion-weighted imaging,DWI)单指数模型和基于体素内不相干运动(intravoxel incoherent motion,IVIM)模型对肺结节的诊断价值。方法 2013年9月~2015年8月同济医院收治的66例肺部结节患者,其中49例男性,17例女性,平均年龄53.1岁(27~76岁),行多b值(0、20、50、100、150、200、400、600、1 000 s/mm2)DWI扫描,利用DWI单指数模型计算综合表观扩散系数值(standard ADC),IVIM模型计算慢速表观扩散系数(slow ADC)、快速表观扩散系数(fast ADC)、快速扩散所占容积分数(F),比较这些参数在肺部良恶性病变和肺癌不同病理类型之间的差异。并应用ROC曲线评价各参数的诊断效能。结果 肺部恶性肿瘤的standard ADC值为1.290(1.040~1.440)×10-3mm2/s,slow ADC值为0.988(0.661~1.139)×10-3mm2/s,良性结节standard ADC和slow ADC值分别为2.000(1.737~2.246)×10-3mm2/s和1.453(1.054~1.668)×10-3mm2/s,恶性肿瘤明显低于良性(P<0.01);fast ADC值变异大,恶性肿瘤的fast ADC值为44.167(7.385~87.050)×10-3mm2/s,良性结节的fast ADC值为7.704(4.861~72.375)×10-3mm2/s,恶性肿瘤明显高于良性(P=0.025);恶性肿瘤的F值为(34.1±16.8)%,良性结节为(51.3±31.8)%,二者差异无统计学意义(P=0.05)。standard ADC阈值取1.569×10-3mm2/s时,鉴别诊断的敏感度、特异度和准确率分别为87.5%、75.0%、83.9%,slow ADC阀值取1.250×10-3mm2/s时,鉴别诊断的敏感度、特异度和准确率分别为95.0%、56.3%和84.4%,联合应用standard ADC与slow ADC诊断的敏感度、特异度与准确率达到97.4%、75.0%和92.2%。鳞癌slow ADC值明显高于小细胞癌。结论 DWI单指数模型和IVIM模型对于肺部良恶性病变均具有鉴别诊断价值,可利用多个不同参数对肺部病变弥散和灌注进行独立评估,standard ADC、slow ADC这两个指标最具诊断价值,联合应用可为鉴别诊断提供重要的定量依据,slow ADC能更为准确地反映肿瘤的实际弥散,对肺癌亚型鉴别有一定意义,而fast ADC由于变异较大故诊断价值有限。
肺结节; 弥散加权成像; 单指数模型; 体素内不相干运动; 表观扩散系数
弥散加权成像(diffusion weighted imaging,DWI))是一种对分子运动或弥散进行成像的技术,能无创地显示人体组织中水分子扩散,已被广泛地应用于多个系统器官疾病的诊断和鉴别诊断,亦有肺部相关的研究,但大部分研究均是利用单指数模型计算表观扩散系数(apparent diffusion coefficient,ADC)来诊断和鉴别诊断。然而,ADC值主要是由2种类型的分子运动确定:在实体组织中扩散(即弥散)和微循环血管中扩散(即灌注)[1]。单指数模型计算ADC值同时包括灌注和弥散的成分,不能完全准确评估水分子在组织内的弥散。而体素内不相干运动理论(intravoxel incoherent motion,IVIM)模型是一种通过分析多b值DWI图像的信号衰减,能同时评估灌注和纯分子扩散运动的MRI成像技术[2],现已有不同系统器官病变IVIM模型的研究,如中枢系统[3]、乳腺[4]、肝脏[5]、前列腺[6],但IVIM模型应用于肺部病变诊断极少。本研究利用IVIM模型对66例肺结节进行分析,旨在探讨IVIM模型对于肺结节的诊断价值。
1 资料与方法
1.1 研究对象
2013年9月~2015年8月在我院行MSCT检出肺结节或肿块的患者,所有病例均经手术或活检得到病理证实,且患者均签署知情同意书。纳入标准:①结节直径≥1 cm;②混杂密度病灶者,空洞或钙化面积小于50%,呈磨玻璃表现者,磨玻璃成分不超过50%[7];③无MRI检查禁忌证;④患者扫描前未经过放化疗。排除标准:呼吸运动伪影大或病灶明显变形。
1.2 MRI检查方法
1.2.1 成像设备 GE signa HDxt 1.5T磁共振扫描仪和8通道相控阵心脏线圈。
1.2.2 常规MR平扫 ①轴位SE/T1WI:心电门控(R波激发),TR/TE 800 ms/8.0 ms,层厚/层间距5.0 mm/1.0 mm,NEX 2,FOV 41 cm×41 cm,矩阵320×160,带宽62.5 kHz,扫描时间6 min。②轴位FRFSE/T2WI:呼吸触发,TR/TE(7 100~9 236)ms/(90~110)ms,层厚/层间距5.0 mm/1.0 mm,NEX 2,ETL 18,FOV 41 cm×41 cm,矩阵320×224,扫描时间3.6 min,施加预饱和脂肪抑制技术得到轴位压脂T2WI。③冠状位SSFSE/T2WI:屏气,TR/TE 823 ms/(70~75)ms,采集次数2,层厚/层间距5.0 mm/1.0 mm,FOV 41 cm×41 cm,扫描时间21 s。
1.2.3 多b值DWI 扫描前先行ASSET校准,再采用单次激发自旋回波-回波平面成像序列(spin echo-echo planar imaging,SE-EPI)行轴位DWI扫描,呼吸触发,FOV 41 cm×41 cm,矩阵256×128,层厚/层间距5.0 mm/1.0 mm,b值取0、20、50、100、150、200、400、600、1 000 s/mm2,NEX最高为6,同时在X、Y、Z轴3个方向上施加弥散敏感梯度脉冲。
1.3 图像后处理与数据测量
应用GE Advantage 4.4工作站的Function tool工具包的MADC软件,结合轴位T2WI在DWI图像上手工勾画感兴趣区(ROI)。ROI选取原则为,所选ROI尽可能包括最大的信号均匀区,避开肉眼可辨的坏死和空洞区。由2位分别有7年和8年磁共振诊断经验的医师在不知道病例临床资料和诊断的基础上独立手工勾画ROI,并利用软件通过DWI单指数和IVIM模型计算综合表观扩散系数值(standard ADC)、慢速表观扩散系数(slow ADC)、快速表观扩散系数(fast ADC)及快速扩散所占容积分数(F),所有数据均测量3次取平均值。
1.4 统计学分析
对2位观察者分别测量所得的10例患者的standard ADC、slow ADC、fast ADC及F值,采用组内相关系数(intra-class correlation coefficient,ICC)评估观察者间的一致性,得出各参数ICC值分别为0.904、0.970、0.980和0.930,均呈良好相关,故在后续统计学分析中仅采用观察者1测量的数据。数据分析采用SPSS 19.0软件,对良恶性病变组间的F值采用t检验,standard ADC、slow ADC和fast ADC采用Mann-Whitney U检验。对于肺癌不同病理类型之间的各指标,服从正态分布和方差齐性者,采用单因素方差分析,方差分析有意义者进行LSD两两比较,差异无统计学意义,则不再进行后续的分析;资料不服从多组正态分布的,采用非参数Kruskal-Wallis H检验。以P<0.05为差异有统计学意义。
2 结果
2.1 病例临床资料
66例患者纳入研究,49例男性,17例女性,平均年龄53.1岁(27~76岁)。按照病理检查结果分为2组:①良性病变组,19例,其中肺隔离症1例,错构瘤1例,硬化性血管瘤2例,炎性肉芽肿3例,结核6例,机化性肺炎6例;②恶性肿瘤组,47例,其中鳞癌12例,腺癌16例,小细胞癌6例,肉瘤样癌3例,大细胞癌2例,典型类癌1例,绒毛膜癌肺转移1例,未能确定病理类型的肺癌6例。
2.2 肺部良恶性病变之间各组参数比较
standard ADC、slow ADC、fast ADC值在良恶性病变之间均有显著性差异,恶性肿瘤的standard ADC和slow ADC明显低于良性,恶性肿瘤的fast ADC明显高于良性,F值在良恶性病变之间的差异则无统计学意义。具体见表1、图1。
用ROC曲线分析各参数的诊断效能,standard ADC、slow ADC、fast ADC的曲线下面积(AUC)分别为0.727、0.709和0.675,差异均有统计学意义(均P<0.05),F值的AUC无明显统计学意义(P=0.05)。根据约登指数得出诊断阈值,并计算各指标敏感度、特异度、准确率,可见slow ADC具有最高的敏感度(95.0%)和准确率(84.4%),而standard ADC具有最高的特异度(75.0%),见表2、图2。当联合应用standard ADC与slow ADC(即取standard ADC≤1.569×10-3mm2/s且slow ADC≤1.250×10-3mm2/s诊断为恶性)时,诊断的敏感度、特异度与准确率达到97.4%、75.0%和92.2%。典型病例MRI影像图见图3。
表1 肺部良恶性病变各参数比较
Table 1 Comparison of ADC and IVIM parameters between malignant and benign nodules

分组standardADC(×10-3mm2/s)slowADC(×10-3mm2/s)fastADC*(×10-3mm2/s)F(%)恶性1.290(1.040~1.440)0.988(0.661~1.139)44.167(7.385~87.050)34.1±16.8良性2.000(1.737~2.246)1.453(1.054~1.668)7.704(4.861~72.375)51.3±31.8统计量-3.679-3.636-2.2471.950P值<0.001<0.0010.0250.050
*非参数检验值用p50(p75~p25)表示
表2 肺部良恶性病变各参数诊断效能
Table 2 Comparison of diagnostic efficacy of parameters between malignant and benign nodules

参数AUC阈值敏感度(%)特异度(%)准确率(%)standardADC0.7271.569×10-3mm2/s87.575.083.9slowADC0.7091.250×10-3mm2/s95.056.384.4fastADC0.67513.288×10-3mm2/s65.068.883.9F0.6690.40372.556.367.9
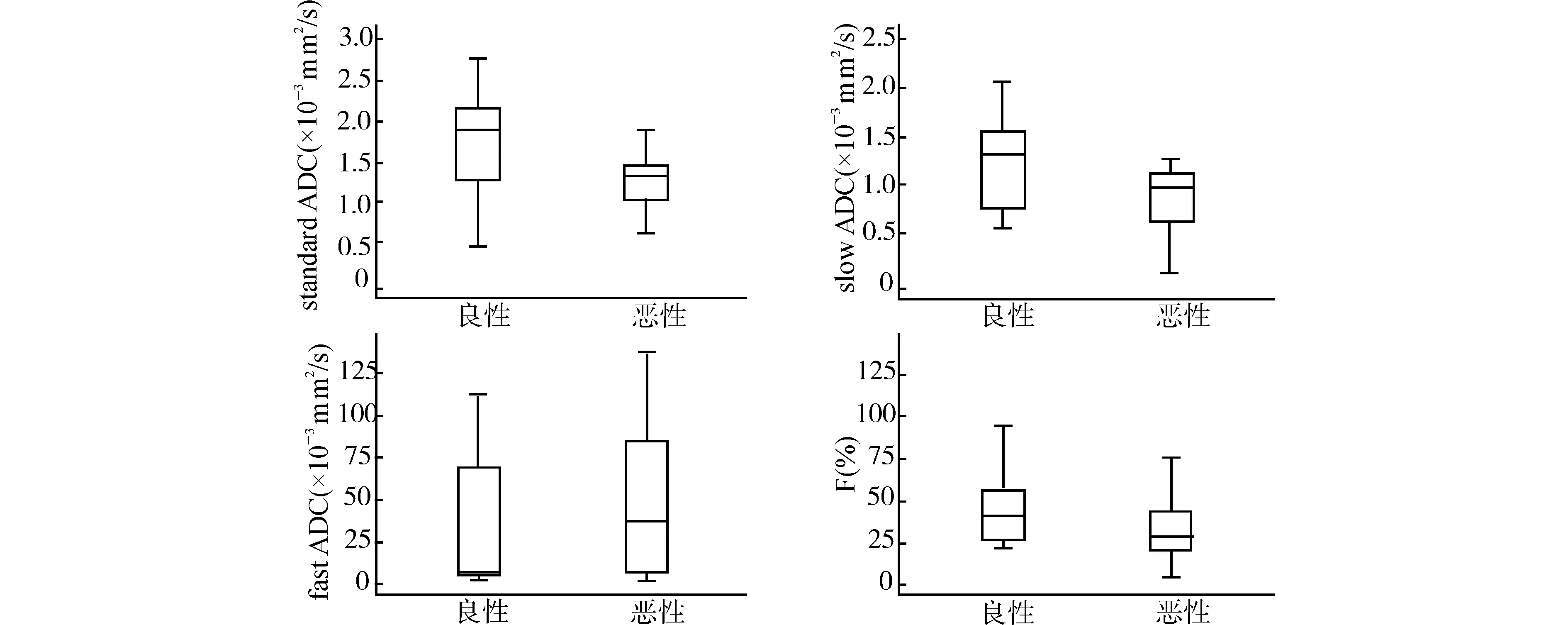
图1 肺部良恶性病变standard ADC、slow ADC、fast ADC和F值箱式图Fig.1 Box plots of standard ADC,slow ADC,fast ADC and F of malignant and benign nodules
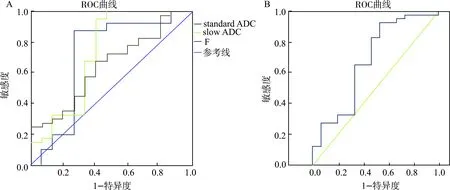
A:standard ADC、slow ADC和F值ROC曲线;B:fast ADC的ROC曲线图2 肺部良恶性病变各指标ROC曲线图Fig.2 Receiver operating characteristic(ROC)curves for ADC and IVIM parameters
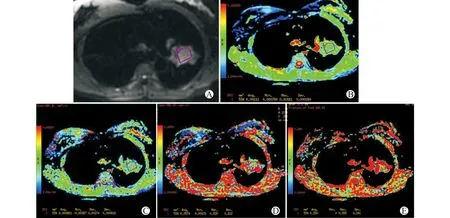
A:轴位平扫DWI图(b=600);B~E:DWI单指数模型和IVIM模型参数伪彩图,分别示standard ADC=1.111×10-3 mm2/s,slow ADC=0.861×10-3 mm2/s,fast ADC=57.4×10-3 mm2/s,F=28.0%图3 某63岁女性左肺上叶腺癌患者的MRI弥散参数图Fig.3 Representative MRI of a lung cancer case (The patient was a 63-year-old woman with adenocarcinoma in the left upper lobe)
2.3 肺癌不同病理类型之间各参数比较
将肺癌不同病理类型的各参数进行比较,发现小细胞癌与非小细胞癌之间各参数差异均无统计学意义。而在肺癌各亚型之间,仅发现鳞癌slow ADC值高于小细胞癌,差异有统计学意义;其他组之间各参数无明显差异,见表3。
表3 肺癌不同病理类型各参数比较
Table 3 Comparison of parameters in different pathological types of lung cancer

分组standardADC(×10-3mm2/s)slowADC(×10-3mm2/s)fastADC(×10-3mm2/s)F(%)鳞癌1.207(0.920~1.423)1.093(0.904~1.140)56.619(8.348~83.494)27.23(17.43~59.84)腺癌1.400(1.105~1.469)1.000(0.811~1.160)45.950(8.113~120.250)26.35(17.68~42.55)小细胞癌1.008(0.768~1.350)0.664(0.454~1.048)35.234(6.491~62.544)31.93(20.14~44.45)其他1.240(0.982~1.377)0.698(0.570~0.865)7.235(5.739~59.735)38.83(34.34~43.30)统计量3.7629.2653.7982.652P值0.2880.0260.2840.448
3 讨论
3.1 DWI单指数模型和IVIM模型
目前国内外[7-8]关于肺部病变的DWI研究主要是基于传统单指数模型的,单指数模型是采用两点法反映两点之间的线性关系,其拟合公式为Sb/S0= Exp(-bD),其中,Sb为相应b值时的DWI信号强度,S0为b=0 s/mm2时DWI信号强度。而各种病变从微观结构上看是由细胞及细胞周围结构所组成,由于体素内包含了细胞内外成分,所以水分子所在的微环境不同时其弥散也不同。因此,有的学者认为基于单指数模型计算出的ADC值其影响因素较多,不足以表征体素内全部水分子的弥散情况,而人体组织的DWI信号衰减也并非简单的线性关系,故通过单指数模型计算得到的ADC与实际存在偏差[9]。而基于体素内不相干运动理论(IVIM)的DWI双指数模型,是在对活体组织弥散研究优化后的处理模型,该假设指出,组织的弥散由两部分组成,一部分是分子的布朗运动,即细胞内弥散(慢速成分,slow ADC),代表了组织内弥散成分,另一部分为压力梯度所致血液流动的快速扩散成分,即细胞外弥散(快速成分,fast ADC),代表了组织的微循环灌注,其拟合公式为Sb/S0= F Exp[-b(Dfast+Dslow)]+(1-F)Exp(-bDslow)[10],其中Sb为相应b值的DWI信号强度,S0为b值为0时的DWI信号强度,Dfast、Dslow分别是快慢两种成分的弥散系数,即前述的fast ADC和slow ADC,F为快速成分所占的百分比,Exp为指数函数。DWI的双指数模型将水分子弥散和组织微循环灌注分开,使得模型模拟的情况更接近真实活体组织,可以得到更准确的实际ADC值,更好反映生物组织的弥散特征[11]。
3.2 DWI单指数模型和IVIM模型在肺部良恶性病变中的诊断价值
目前,已有IVIM在全身不同系统器官应用的研究,如肝纤维化[12]、鼻咽癌[13]、脑梗死[14]、肾脏病变[15]、胎盘功能[16]、乳腺癌[17]等,但此类研究尚少,在本研究测算的4个参数,单指数模型参数standard ADC值表示为综合ADC值(同时受弥散和灌注影响),IVIM模型参数slow ADC为弥散相关参数,fast ADC及F为灌注相关参数。我们的研究显示,肺癌的standard ADC和slow ADC明显低于良性结节,这符合多个研究报道得出的由于肺癌细胞密度明显增加、细胞外间隙减小、核质比增大等改变,导致肿瘤内弥散明显较正常及良性病变减低的结论,且slow ADC值在良性病变和恶性病变中均比standard ADC值低,表明IVIM模型剔除了血流灌注因素,更准确地反映了肿瘤细胞内水分子弥散程度。
有研究报道,fast ADC可以反映肿瘤的血流速度,在肝纤维化中fast ADC明显降低,与硬化的肝脏灌注减低相关[18],同样在头颈部纤维化的组织中该参数也明显减低,提示与头颈部肿瘤的血管生成直接相关[19],本研究中肺部恶性肿瘤的fast ADC明显较良性病变高(P=0.025),可能反映了肺部恶性肿瘤新生血管形成及供血血管血流速度较快、血供增加。但在本研究中此参数变异极大,在肺癌中,fast ADC为44.167(7.385~87.050)×10-3mm2/s,良性结节的fast ADC值为7.704(4.861~72.375)×10-3mm2/s,提示可能此指标并不适用于IVIM模型,且可靠性不高,这点与早前的研究结果[20-21]一致,这些研究指出,fast ADC的测量可重复性不高,稳定性不如slow ADC和F。fast ADC值的不稳定性,可能与DWI图形畸形变、心脏大血管搏动伪影和fast ADC图噪声较高有关。关于这个参数对于肺部病变是否是一个潜在有意义的指标,仍需进一步扩大样本、重复及优化实验条件后进行。
本研究中,肺恶性肿瘤的F值低于良性,但差异无统计学意义。F和fast ADC均是灌注相关参数,理论上来说,由于肿瘤新生血管生成,F值应该高于良性病变,但某些研究报道也不尽如此,如Lai等[22]发现鼻咽癌相对于治疗后纤维化组织的F值低,Shinmoto等[23]发现前列腺癌比周围正常组织的F值低。产生这样的现象,可能与Sumi等[24]提到的F值同时受到灌注和纯分子弥散的T2贡献的影响有关,理论上来说,IVIM模型中F值定义为毛细血管和肿瘤组织的信号强度比,在这种设定之下,所有的弛豫效应都被忽略了,当肿瘤和毛细血管的弛豫时间相似,这种假设是成立的,但有时肿瘤和毛细血管的T2贡献相差巨大,因而F值是两者的综合作用结果,此外,肺癌和良性病变供血血管的差异亦可能对F值的变异性产生影响。在本研究中,良性病变主要由炎性肉芽肿、感染、机化性肺炎、硬化血管瘤等病变构成,这些病变的血供也较为丰富,因而导致良性F值数值上更高的结果。今后,应该考虑通过校正T2弛豫时间来分析F这个参数,且在病例选择上,选择更多数量的同类型良性病变对比,可能对F值的分析更具科学性。
通过对DWI单指数模型和IVIM模型参数对肺部良恶性结节鉴别诊断的诊断效能分析,我们发现,IVIM模型参数slow ADC具有最高的敏感度(95.0%)和准确率(84.4%),特异度不佳(56.3%),而单指数模型参数standard ADC具有最高的特异度(75.0%),敏感度(87.5%)和准确率(83.9%)稍逊于slow ADC。当联合应用standard ADC与slow ADC(即取standard ADC≤1.569×10-3mm2/s且slow ADC≤1.250×10-3mm2/s诊断为恶性)时,诊断的敏感度、特异度与准确率达到97.4%、75.0%和92.2%,具有良好的鉴别诊断意义。
此外,本研究发现,在不同肺癌病理类型之间,鳞癌slow ADC值高于小细胞癌,提示小细胞癌较鳞癌有更高的细胞密度,这符合小细胞癌的病理学特征。然而,由于样本量较小,此结论仍需大样本试验进一步证实。
DWI单指数模型和IVIM模型对于肺部良恶性病变均具有鉴别诊断价值,可利用多个不同参数对肺部病变弥散和灌注进行独立评估,standard ADC、slow ADC这2个指标最具诊断价值,联合两者可明显提高鉴别诊断能力,slow ADC能更为准确地反映肿瘤的实际弥散,对肺癌亚型鉴别有一定意义,而fast ADC由于变异较大而诊断价值有限。
[1] Le Bihan D.Diffusion,confusion and functional MRI[J].Neuro Image,2012,62(2):1131-1136.
[2] Le Bihan D.Intravoxel incoherent motion perfusion MR imaging:a wake-up call[J].Radiology,2008,249(3):748-752.
[3] Wu W C,Yang S C,Chen Y F,et al.Simultaneous assessment of cerebral blood volume and diffusion heterogeneity using hybrid IVIM and DK MR imaging:initial experience with brain tumors[J].Eur Radiol,2016.[Epub ahead of print]
[4] Liu C,Wang K,Chan Q,et al.Intravoxel incoherent motion MR imaging for breast lesions:comparison and correlation with pharmacokinetic evaluation from dynamic contrast-enhanced MR imaging[J].Eur Radiol,2016.[Epub ahead of print]
[5] Ichikawa S,Motosugi U,Morisaka H,et al.MRI-based staging of hepatic fibrosis:Comparison of intravoxel incoherent motion diffusion-weighted imaging with magnetic resonance elastography[J].J Magn Reson Imaging,2015,42(1):204-210.
[6] Merisaari H,Movahedi P,Perez I M,et al.Fitting methods for intravoxel incoherent motion imaging of prostate cancer on region of interest level:Repeatability and gleason score prediction[J].Magn Reson Med,2016.doi:10.1002/mrm.26169.[Epub ahead of print]
[7] Matoba M,Tonami H,Kondou T,et al.Lung carcinoma:diffusion-weighted mr imaging--preliminary evaluation with apparent diffusion coefficient[J].Radiology,2007,243(2):570-577.
[8] Liu H,Liu Y,Yu T,et al.Usefulness of diffusion-weighted MR imaging in the evaluation of pulmonary lesions[J].Eur Radiol,2010,20(4):807-815.
[9] Gruber S,Debski B K,Pinker K,et al.Three-dimensional proton MR spectroscopic imaging at 3T for the differentiation of benign and malignant breast lesions[J].Radiology,2011,261(3):752-761.
[10] Federau C,Maeder P,O’Brien K,et al.Quantitative measurement of brain perfusion with intravoxel incoherent motion MR imaging[J].Radiology,2012,265(3):874-881.
[11] Nilsen L B,Fangberget A,Geier O,et al.Quantitative analysis of diffusion-weighted magnetic resonance imaging in malignant breast lesions using different b value combinations[J].Eur Radiol,2013,23(4):1027-1033.
[12] Patel J,Sigmund E E,Rusinek H,et al.Diagnosis of cirrhosis with intravoxel incoherent motion diffusion MRI and dynamic contrast-enhanced MRI alone and in combination:preliminary experience[J].J Magn Reson Imaging,2010,31(3):589-600.
[13] Jia Q J,Zhang S X,Chen W B,et al.Initial experience of correlating parameters of intravoxel incoherent motion and dynamic contrast-enhanced magnetic resonance imaging at 3.0T in nasopharyngeal carcinoma[J].Eur Radiol,2014,24(12):3076-3087.
[14] Federau C,Sumer S,Becce F,et al.Intravoxel incoherent motion perfusion imaging in acute stroke:initial clinical experience[J].Neuroradiology,2014,56(8):629-635.
[15] Rheinheimer S,Stieltjes B,Schneider F,et al.Investigation of renal lesions by diffusion-weighted magnetic resonance imaging applying intravoxel incoherent motion-derived parameters--initial experience[J].Eur J Radiol,2012,81(3):e310-e316.
[16] Moore R J,Issa B,Tokarczuk P,et al.Invivointravoxel incoherent motion measurements in the human placenta using echo-planar imaging at 0.5 T[J].Magn Reson Med,2000,43(2):295-302.
[17] Sigmund E E,Cho G Y,Kim S,et al.Intravoxel incoherent motion imaging of tumor microenvironment in locally advanced breast cancer[J].Magn Reson Med,2011,65(5):1437-1447.
[18] Luciani A,Vignaud A,Cavet M,et al.Liver cirrhosis:intravoxel incoherent motion MR imaging--pilot study[J].Radiology,2008,249(3):891-899.
[19] Malayeri A A,El Khouli R H,Zaheer A,et al.Principles and applications of diffusion-weighted imaging in cancer detection,staging,and treatment follow-up[J].Radiographics,2011,31(6):1773-1791.
[20] Dyvorne H A,Galea N,Nevers T,et al.Diffusion-weighted imaging of the liver with multiple b values:effect of diffusion gradient polarity and breathing acquisition on image quality and intravoxel incoherent motion parameters--a pilot study[J].Radiology,2013,266(3):920-929.
[21] Woo S,Lee J M,Yoon J H,et al.Intravoxel incoherent motion diffusion-weighted MR imaging of hepatocellular carcinoma:correlation with enhancement degree and histologic grade[J].Radiology,2014,270(3):758-767.
[22] Lai V,Li X,Lee V H F,et al.Intravoxel incoherent motion MR imaging:comparison of diffusion and perfusion characteristics between nasopharyngeal carcinoma and post-chemoradiation fibrosis[J].Eur Radiol,2013,23(10):2793-2801.
[23] Shinmoto H,Oshio K,Tanimoto A,et al.Biexponential apparent diffusion coefficients in prostate cancer[J].Magn Reson Imaging,2009,27(3):355-359.
[24] Sumi M,Van C M,Sumi T,et al.Salivary gland tumors:use of intravoxel incoherent motion MR imaging for assessment of diffusion and perfusion for the differentiation of benign from malignant tumors[J].Radiology,2012,263(3):125-126.
(2016-09-07 收稿)
Monoexponential and IVIM Model of Diffusion Weighted Imaging in Pulmonary Nodules:A Preliminary Study
Zhou Shuchang,Xia Liming△,Wang Yujinetal
DepartmentofRadiology,TongjiHospital,TongjiMedicalCollege,HuazhongUniversityofScienceandTechnology,Wuhan430030,China
Objective To explore the effect of Mono-exponential and IVIM model of diffusion weighted imaging in the diagnosis of solitary pulmonary nodules.Methods A total of 66 patients with pulmonary nodules(49 men,17 women,mean age:53.1 years;age range 27-76 years)underwent multi-b-factor DWI(b values of 0,20,50,100,150,200,400,600,and 1 000 s/mm2).The biexponential model based on the intravoxel incoherent motion theory(IVIM)was used to calculate parameters as follows:total ADC(standard ADC),slow component apparent diffusion coefficient(slow ADC),fast component apparent diffusion coefficient(fast ADC),and fast diffusion percentage(F).These parameters were compared between benign and malignant lesions and between different pathological types of lung cancer.Receiver operating characteristic(ROC)curves were generated to evaluate the diagnostic performance of each parameter.Results Standard ADC value of malignant tumor and benignity was 1.290(1.040-1.440)×10-3mm2/s and 2.000(1.737-2.246)×10-3mm2/s,respectively.Slow ADC value of malignant tumor and benignity was 0.988(0.661-1.139)×10-3mm2/s and 1.453(1.054-1.668)×10-3mm2/s,respectively.These two parameters were significantly lower in malignant tumor than in benign lesions(P<0.01),fast ADC value of malignant tumor and benignity was 44.167(7.385-87.050)×10-3mm2/s and 7.704(4.861-72.375)×10-3mm2/s,respectively.Fast ADC value of malignant tumor was significantly higher than that of benign lesions(P=0.025).F value of malignant tumor(34.1±16.8)% was lower than that of benign lesions(51.3±31.8)%(P=0.05),with no significantly statistical difference.Taking 1.569×10-3mm2/s and 1.250 ×10-3mm2/s as cutoff values of standard ADC and slow ADC,the diagnostic sensitivity,specificity and accuracy were 87.5%,75.0% and 83.9%,and they were 95.0%,56.3% and 84.4%,respectively.The combined application of standard ADC and slow ADC increased the diagnostic sensitivity,specificity and accurate rate to 97.4%,75.0% and 92.2%.Slow ADC values of squamous cell carcinoma were significantly higher than those of small cell carcinoma. Conclusion Both mono-exponential and bi-exponential model DWI based on IVIM is useful for differentiating benign and malignant pulmonary nodules,and can provide quantitative diffusion and perfusion information independently by multiple parameters.Standard ADC and slow ADC are the most valuable parameters and are able to differentiate benign and malignant nodules.Slow ADC can reflect the actual diffusion of tumor more accurately and help to differentiate subtypes of lung cancer.Fast ADC has limited diagnostic value because of high variability.
pulmonary nodules; diffusion weighted imaging; monoexponential model; intravoxel incoherent motion;apparent diffusion coefficient
R814.4
10.3870/j.issn.1672-0741.2016.06.012
周舒畅,女,1983年生,主治医师,博士研究生,E-mail:zhoushuchang@hust.edu.cn
△通讯作者,Corresponding author,E-mail:cjr.xialiming@vip.163.com
猜你喜欢
中老年保健(2022年6期)2022-08-19
云南医药(2021年3期)2021-07-21
内蒙古林业(2021年6期)2021-06-26
健康之家(2021年19期)2021-05-23
医学食疗与健康(2021年27期)2021-05-13
农业科技与信息(2021年2期)2021-03-27
中国临床医学影像杂志(2019年5期)2019-08-27
中国交通信息化(2018年5期)2018-08-21
中国卫生(2016年9期)2016-11-12
中国继续医学教育(2015年1期)2016-01-06
