认知障碍简明评价量表在行为异常型额颞叶痴呆及阿尔茨海默病病人照料者负担评估中的应用
2017-10-20 09:01
实用老年医学 2017年10期
认知障碍简明评价量表在行为异常型额颞叶痴呆及阿尔茨海默病病人照料者负担评估中的应用
汤群英徐俊顾小花胡月洪音李琳陶带花成佳星
目的探讨认知障碍简明评价量表(Cog-12)在评估行为异常型额颞叶痴呆(bvFTD)及阿尔茨海默病(AD)病人照料者负担中的应用价值。方法研究对象取自2007年1月至2015年11月来自中国阿尔茨海默病与相关疾病研究协作组(CARDS)研究课题登记的基线调查部分的对象,共计入组了临床痴呆量表(CDR)评分为1~2分的206例痴呆病人(AD组120例,bvFTD组86例)。所有病人均完成Cog-12量表、Addenbrooke改良认知评估量表(ACE-R)、额叶行为量表(FBI)的测评,所有照料者均完成照料者负担问卷(caregiver burden inventory,CBI)、神经精神问卷(NPI)、焦虑自评量表(SAS)、抑郁自评量表(SDS)的测评。结果(1)bvFTD组病人ACE-R,FBI,Cog-12,NPI评分均高于AD组。bvFTD组照料者CBI,SAS,SDS评分均高于AD组,其中,bvFTD组时间依赖负担及情感负担较AD组重,2组发展受限评分、身体负担评分及社交负担评分差异无统计学意义;(2)bvFTD组CBI与Cog-12,NPI,FBI均呈显著正相关,AD组CBI与Cog-12,NPI呈显著正相关;2组SAS、SDS 与CBI呈显著正相关;(3)bvFTD组照料者负担主要来源于病人的神经精神及行为症状,而AD组照料者负担主要来源于神经精神症状。结论bvFTD照料者负担较AD照料者负担更重,出现抑郁、焦虑风险更高。bvFTD照料者负担重与病人神经精神症状及行为紊乱密切相关,AD照料者负担主要与神经精神症状相关,Cog-12可推广作为间接评估痴呆病人照料者负担的工具。专业照料指导、心理支持等减轻照料者负担措施迫在眉睫。
行为异常型额颞叶痴呆; 阿尔茨海默病; 照料者负担; 认知障碍简明评价量表
随着人口老龄化,痴呆人数迅速增加,目前已成为各国面临的主要公共卫生难题。目前我国大陆老年期痴呆人群高达900万[1],阿尔茨海默病(Alzheimer’ s disease, AD)是导致老年期认知障碍最常见病因,而额颞叶痴呆(frontotemporal lobar dementia, FTD)是第二大常见痴呆类型[2]。行为异常型额颞叶痴呆(behavioral variant of frontotemporal dementia, bvFTD)是其中最常见的亚型。目前,我国尚缺乏完善的痴呆病人照料管理措施,痴呆病人给照料者带来沉重的身心负担,因2种痴呆具有不同的病理类型及受累部位,导致了不同的临床表现,可能给照料者带来不同程度及类型的负担。近年来一系列研究评估了AD及FTD的照料者负担[3-8],但研究结果尚有争议,且目前国内尚缺乏AD及bvFTD照料者负担的比较研究,本研究拟探讨认知障碍简明评价量表(brief cognitive impairment rating scale, Cog-12)在评估AD及bvFTD照料者负担中的应用价值。
1 对象和方法
1.1 研究对象 选取2007年1月至2015年11月来自中国阿尔茨海默病与相关疾病研究协作组(CARDS)研究课题登记的研究对象。共纳入206例,其中bvFTD组86例,男39例,女47例,发病年龄44~80岁,平均(60.7±7.3)岁;AD组120例,男47例,女73例,发病年龄55~88岁,平均(69.0±7.3)岁。bvFTD病人入组标准:(1)根据国际行为变异型额颞叶痴呆标准联盟(International Behavioural Variant FTD Criteria Consortium,FTDC)2011新版 bvFTD诊断标准[9],诊断为“很可能bvFTD”;(2)临床痴呆量表(clinical dementia rating, CDR)[10]评分为1~2分。AD病人入组标准:(1)符合美国国立神经病、语言交流障碍和卒中研究所-老年性痴呆及相关疾病学会(NINCDS/ADRDA)的“很可能AD”标准诊断[11];(2)CDR评分为1~2分。排除标准:(1)不符合bvFTD或AD诊断标准;(2)合并严重焦虑、抑郁症或严重精神症状;(3)合并可导致失去生活自理能力的其他严重疾病。最终由长期从事认知功能障碍专科的医生做出诊断。
照料者入组标准:(1)照料者对病人病情比较了解,是病人主要照料人,每天照料病人6 h以上;(2)照料者依从性好,同意并配合此项研究,并签署知情同意书。照料者排除标准:合并语言或听力障碍,无法完成量表评估者。
本研究符合医学伦理学标准,通过了江苏省苏北人民医院医学伦理委员会的审核 (批准号:SBYY2015003)。
1.2 方法
1.2.1 一般资料收集:收集所有入组病人性别、年龄、教育程度等人口学特征,照料者与病人关系,照料年限,工作类型,家庭收入情况等一般资料。
1.2.2 神经心理学评估:所有资料收集均由接受过培训的专科医师或调查员完成问卷评估及填写。
1.2.2.1 问卷调查:所有病人完成CDR,Addenbrooke改良认知评估量表(Addenbrooke’s Cognitive Examination-revised, ACE-R),Cog-12,额叶行为量表(frontal behavior inventory, FBI),神经精神问卷(NPI)评估。CDR是医生通过六项功能(记忆力,定向力,判断和解决问题的能力,社会事物,家庭生活业余爱好,个人照料)的每个方面分别作出从无损害到重度损害五级评估,但每项功能的得分不叠加,而是根据总的评分标准将六项能力的评定综合成一个总分,其结果以0,0.5,1,2,3分表示。ACE-R是包括简易精神状态量表(mini-mental state examination,MMSE) 在内的神经心理测评量表,ACE-R中包涵MMSE各项得分[12]。Cog-12是由知情者完成的,反映痴呆病人常见认知损害的客观量表,共12个条目。FBI是通过照料者角度评估bvFTD病人行为紊乱症状的量表[13],包含24个测评项目,根据症状严重程度分为0~3分。NPI主要用于评估病人的神经精神症状,包含12个测评项目,根据症状严重程度分为1~3分,根据症状的出现频率分为1~4分,根据各症状的频率×严重程度总和计算总分[14]。
1.2.2.2 所有照料者完成照料者负担问卷(caregiver burden inventory, CBI)、焦虑自评量表(SAS)及抑郁自评量表(SDS):CBI是由Novak和Guest编制,主要用于测量照料者的照料负担,包含24个测评项目,根据负担严重程度分为0~4分,包括5个负担分类:时间依赖负担,发展受限负担,身体负担,社交负担,情感负担[15]。SAS、SDS用于评估照料者的焦虑、抑郁症状,SAS标准分:总粗分×1.25后取整,焦虑分界值为50分;SDS标准分:总粗分×1. 25 后取整,其中抑郁分界值为53分。
1.3 统计学方法 采用EpiData 3.1软件建立数据库并进行双录入核查。采用SPSS 13.0统计软件进行分析,符合正态分布的计量资料用均数±标准差表示,2组间比较采用两独立样本t检验,率或构成比比较采用χ2检验,用Person相关分析评估量表之间相关性;用多重线性回归分析各影响因素对照料者负担的影响。P<0.05为差异有统计学意义。
2 结果
2.1 一般资料 bvFTD组及AD组之间性别、教育程度、照料者分布、家庭收入情况、照料者照料年限及CDR评分差异均无统计学意义,而bvFTD组发病年龄显著早于AD。见表1。
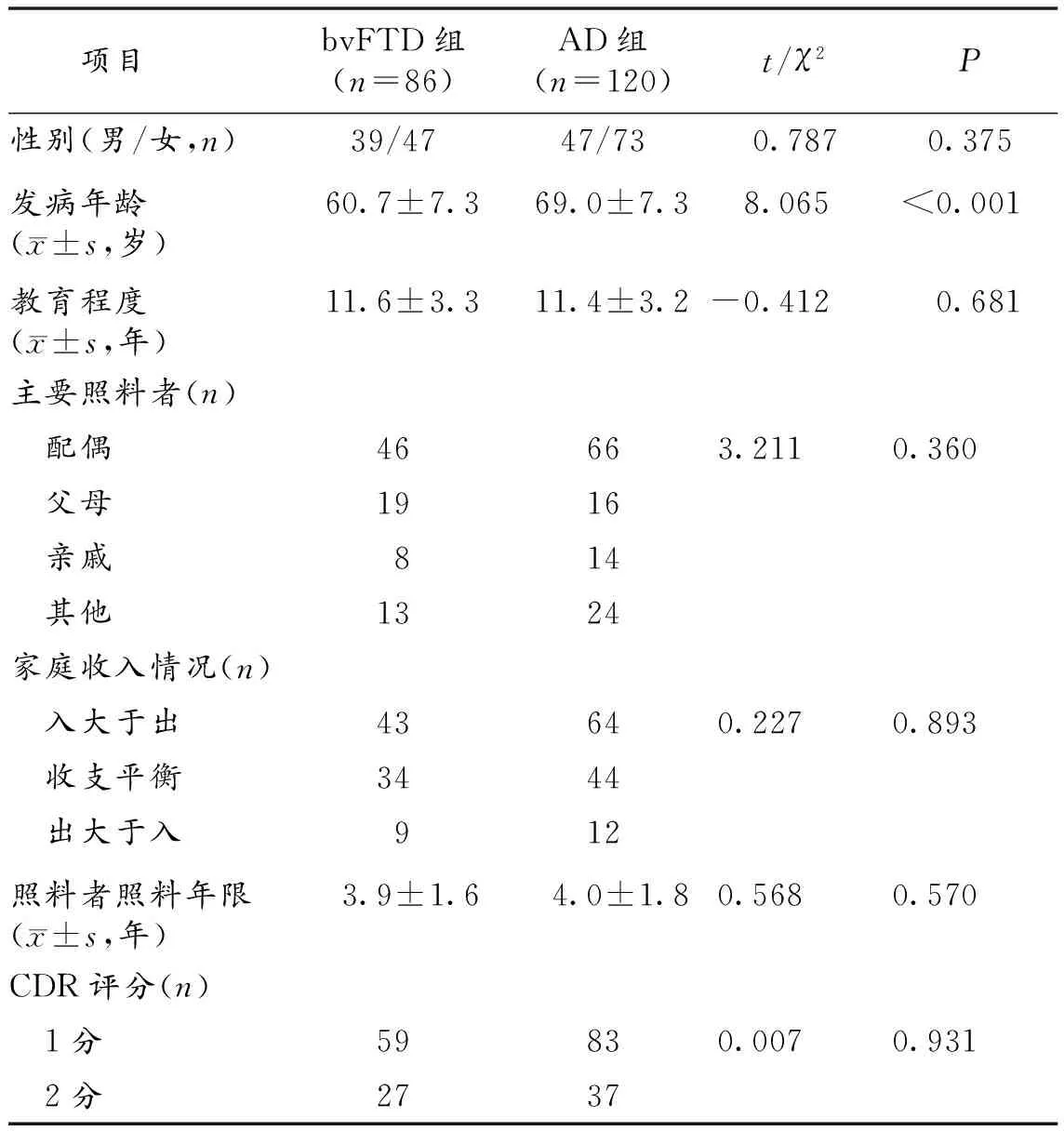
表1 bvFTD组与AD组一般资料比较
2.2 bvFTD组与AD组病人神经心理量表评估及照料者负担评估结果 bvFTD组ACE-R、FBI、Cog12、NPI评分均高于AD组,差异有统计学意义。bvFTD组照料者CBI、SAS、SDS评分均高于AD组,其中,bvFTD组时间依赖负担及情感负担显著较AD组重。bvFTD组与AD组NPI评分比较结果显示,bvFTD组淡漠、脱抑制和异常行为症状评分显著高于AD组,AD组幻觉、妄想症状评分显著高于bvFTD组,而使bvFTD照料者苦恼的主要症状为激越、攻击性,异常运动行为及睡眠障碍,AD照料者苦恼的主要症状为睡眠障碍、幻觉。见表2。

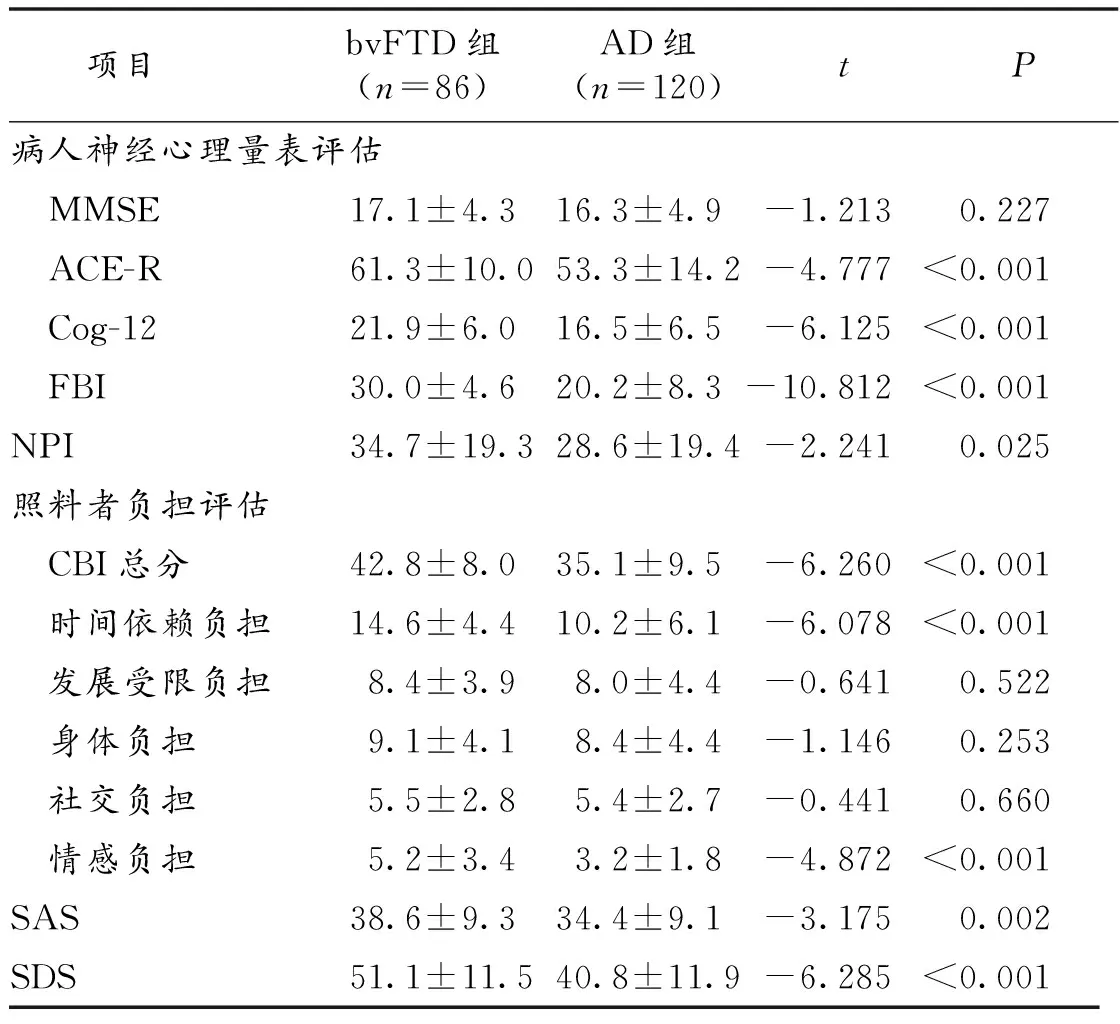
项目bvFTD组(n=86)AD组(n=120)tP病人神经心理量表评估 MMSE17.1±4.316.3±4.9-1.2130.227 ACE-R61.3±10.053.3±14.2-4.777<0.001 Cog-1221.9±6.016.5±6.5-6.125<0.001 FBI30.0±4.620.2±8.3-10.812<0.001NPI34.7±19.328.6±19.4-2.2410.025照料者负担评估 CBI总分42.8±8.035.1±9.5-6.260<0.001 时间依赖负担14.6±4.410.2±6.1-6.078<0.001 发展受限负担8.4±3.98.0±4.4-0.6410.522 身体负担9.1±4.18.4±4.4-1.1460.253 社交负担5.5±2.85.4±2.7-0.4410.660 情感负担5.2±3.43.2±1.8-4.872<0.001SAS38.6±9.334.4±9.1-3.1750.002SDS51.1±11.540.8±11.9-6.285<0.001
2.3 照料者负担影响因素的多重线性回归分析 AD组CBI评分与Cog-12,NPI呈显著正相关,Pearson相关系数(r)分别为0.879,0.848(P<0.001),CBI与FBI、ACE-R未见显著相关性。bvFTD组CBI评分与Cog-12,NPI,FBI均呈显著正相关,r分别为0.679,0.694,0.668(P<0.001),CBI与ACE-R未见显著相关性。所有对象SAS、SDS 与CBI评分均呈显著正相关,r分别为0.539,0.661(P<0.001)。分别对2组照料者负担相关影响因素进行多重线性回归分析,以CBI为因变量,以性别、年龄教育程度、照料者分布、家庭收入情况、照料者照料年限,CDR评分及所有神经心理学量表指标为自变量,进行多因素线性回归分析,结果显示,FBI、NPI对bvFTD组照料者负担影响大,这2个因素可解释照料者负担变化的67.5%;NPI评分、Cog-12对AD组照料者负担影响大,这2个因素可解释照料者负担变化的80.7%,见表3。
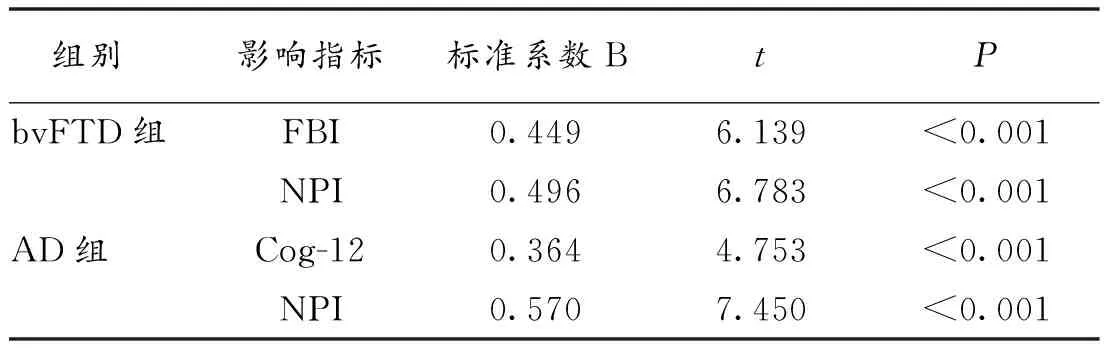
表3 影响2组照料者负担相关因素的多重线性回归分析
3 讨论
既往研究比较了bvFTD及AD的照料者负担,本研究与大多数研究结果一致[6, 8],bvFTD照料者承受负担更重。我们采用了CBI量表评估照料者负担,CBI量表将照料者负担分为5个维度,bvFTD组照料负担主要体现在时间依赖负担及情感负担上。时间依赖负担主要取决于病人的日常生活能力,同等痴呆严重程度下,bvFTD病人常伴有更严重的行为紊乱及精神行为异常,导致其日常生活能力低下,个人自理能力显著下降,对照料者严重依赖,照料者需付出更多时间及精力看护病人[8]。本研究中,bvFTD组情感负担较AD组重,与国外相关研究结果不一致[8],考虑可能与中外不同的文化背景相关,部分bvFTD照料者对病人异常行为感到尴尬、羞耻,甚至导致病人定期门诊随访依从性下降。
与AD组相比,bvFTD组淡漠、脱抑制和异常行为症状更多见,与既往研究一致[9],但值得注意的是,显著增加照料者负担、使照料者苦恼的主要症状为激越、攻击性,异常运动行为及睡眠障碍。攻击性及异常行为显著增加照料者负担[16-17],有时甚至导致病人及照料者意外伤害,照料者需付出更多时间看护,此外,异常行为显著增加了照料者情感负担,可能导致照料者减少病人日常外出活动。淡漠症状在bvFTD组中较常见,Dauphinot等[18]认为淡漠通常伴随着抑郁症状,病人常需要更多帮助来维持日常活动能力,从而可能增加照料者负担。但本研究未发现其与照料者负担有显著相关,可能因本研究中照料者主要为病人家属,未接受专业的照料培训,未将固定时间及强度的日常活动作为照料目标之一,部分照料者甚至认为,与有激越症状相比,淡漠症状显著降低了照料负担。
幻觉、妄想症状在本研究bvFTD组中相对少见,而在AD组较多,尤其以视幻觉多见,被害妄想可导致病人做出异常行为,增加照料者负担[19]。本研究未发现病人教育程度、家庭收入情况、照料者关系及照料年限与照料者负担之间有显著相关性,可能与本研究系单中心研究有关,尚需多中心、大样本研究进一步验证。
本研究中SAS、SDS 与CBI呈显著正相关,提示照料者负担越重,并发抑郁、焦虑可能性越大,程度越重。沉重的照料负担不仅可导致照料者情绪障碍,还可导致一系列器质性疾病[20],早期心理干预、针对性的照料辅导有助于减轻负担。
本研究还发现,bvFTD组CBI与Cog-12、NPI、FBI均呈显著正相关,与ACE-R未见显著相关性,而AD组CBI与Cog-12、NPI呈显著正相关,与FBI、ACE-R未见显著相关性。且线性回归分析也表明ACE-R对2组照料者负担均无显著影响,进一步表明精神、行为紊乱是影响bvFTD照料者负担最重要的因素之一,神经、精神症状是影响AD照料者负担最重要因素[5, 21]。
综上所述,bvFTD组照料者较AD组照料者承受更大的负担及照料压力。 bvFTD组照料者负担重与病人神经精神症状及行为紊乱密切相关,AD组照料者负担主要与神经精神症状相关,NPI、Cog-12可作为间接评估照料者负担的工具,而与NPI相比,Cog-12耗时短,步骤简洁,可推广用于评估痴呆病人的照料者负担。
[1] 徐俊,顾小花. 前言——我国老年期认知障碍诊治现状与展望[J]. 实用老年医学, 2014, 28(7):531-533.
[2] Seelaar H, Rohrer JD, Pijnenburg YA, et al. Clinical, genetic and pathological heterogeneity of frontotemporal dementia: a review[J]. J Neurol Neurosurg Psychiatry, 2011, 82(5):476-486.
[3] Svendsboe E, Terum T, Testad I, et al. Caregiver burden in family carers of people with dementia with Lewy bodies and Alzheimer’s disease[J]. Int J Geriatr Psychiatry, 2016, 31(9):1075-1083.
[4] Brodaty H, Woodward M, Boundy K, et al. Prevalence and predictors of burden in caregivers of people with dementia[J]. Am J Geriatr Psychiatry, 2014, 22(8):756-765.
[5] Uflacker A, Edmondson MC, Onyike CU, et al. Caregiver burden in atypical dementias: comparing frontotemporal dementia, Creutzfeldt-Jakob disease, and Alzheimer’s disease[J]. Int Psychogeriatr, 2016, 28(2):269-273.
[6] Mioshi E, Foxe D, Leslie F, et al. The impact of dementia severity on caregiver burden in frontotemporal dementia and Alzheimer disease[J]. Alzheimer Dis Assoc Disord, 2013, 27(1):68-73.
[7] Springate BA,Tremont G. Dimensions of caregiver burden in dementia: impact of demographic, mood, and care recipient variables[J]. Am J Geriatr Psychiatry, 2014, 22(3):294-300.
[8] Kucukguclu O, Soylemez BA, Yener G, et al. Examining factors affecting caregiver burden: A comparison of frontotemporal dementia and Alzheimer’s dsease[J]. Am J Alzheimers Dis Other Demen, 2017,32(4):200-206.
[9] Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia[J]. Brain, 2011, 134(Pt 9):2456-2477.
[10] Morris JC. The clinical dementia rating (CDR): current version and scoring rules[J]. Neurology, 1993, 43(11):2412-2414.
[11] McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease[J]. Neurology, 1984, 34(7):939-944.
[12] Mioshi E, Dawson K, Mitchell J, et al. The Addenbrooke’s Cognitive Examination Revised (ACE-R): a brief cognitive test battery for dementia screening[J]. Int J Geriatr Psychiatry, 2006, 21(11):1078-1085.
[13] Kertesz A, Davidson W,Fox H. Frontal behavioral inventory: diagnostic criteria for frontal lobe dementia[J]. Can J Neurol Sci, 1997, 24(1):29-36.
[14] Cummings JL, Mega M, Gray K, et al. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia[J]. Neurology, 1994, 44(12):2308-2314.
[15] Novak M,Guest C. Application of a multidimensional caregiver burden inventory[J]. Gerontologist, 1989, 29(6):798-803.
[16] Liu S, Jin Y, Shi Z, et al. The effects of behavioral and psychological symptoms on caregiver burden in frontotemporal dementia, Lewy body dementia, and Alzheimer’s disease: clinical experience in China[J]. Aging Ment Health, 2017, 21(6):651-657.
[17] Matsumoto N, Ikeda M, Fukuhara R, et al. Caregiver burden associated with behavioral and psychological symptoms of dementia in elderly people in the local community[J]. Dement Geriatr Cogn Disord, 2007, 23(4):219-224.
[18] Dauphinot V, Delphin-Combe F, Mouchoux C, et al. Risk factors of caregiver burden among patients with Alzheimer’s disease or related disorders: a cross-sectional study[J]. J Alzheimers Dis, 2015, 44(3):907-916.
[19] Joshi A, Barsuglia JP, Mather MJ, et al. Evaluation of emotional blunting in behavioral variant frontotemporal dementia compared to Alzheimer’s disease[J]. Dement Geriatr Cogn Disord, 2014, 38(1/2):79-88.
[20] Epstein-Lubow G, Davis JD, Miller IW, et al. Persisting burden predicts depressive symptoms in dementia caregivers[J]. J Geriatr Psychiatry Neurol, 2008, 21(3):198-203.
[21] Lima-Silva TB, Bahia VS, Carvalho VA, et al. Neuropsychiatric symptoms, caregiver burden and distress in behavioral-variant frontotemporal dementia and Alzheimer’s disease[J]. Dement Geriatr Cogn Disord, 2015, 40(5/6):268-275.
ApplicationofbriefcognitiveimpairmentratingscaleinevaluatingcaregiverburdenofpatientswithbehavioralvariantoffrontotemporaldementiaorAlzheimer’sdisease
TANGQun-ying.
DepartmentofNeurology,JingjiangPeople’sHospital,Taizhou214500,China;XUJun,HUYue,LILin,TAODai-hua,CHENGJia-xing.DepartmentofNeurology;GUXiao-hua.DepartmentofIntensiveCareUnit;HONGYin.HealthManagementCenter,NorthernJiangsuPeople’sHospital,Yangzhou225001,China
ObjectiveTo explore the value of brief cognitive impairment rating scale(Cog-12)in evaluating caregiver burden of patients with behavioral variant of frontotemporal dementia (bvFTD) or Alzheimer’s disease (AD).MethodsThe study was part of China Alzheimer’s Disease and Related Diseases Study, caregivers and patients diagnosed with AD (n=120) or bvFTD (n=86) between January 2007 to November 2015 were selected. The scores of clinical dementia rating (CDR) of all patients were 1 or 2. The Cog-12, Addenbrooke’s cognitive examination-revised (ACE-R), and frontal behavioral inventory (FBI) were applied for evaluating cognitive and behavior performances in all patients. And caregiver burden inventory (CBI), neuropsychiatric inventory (NPI), self-rating anxiety scale(SAS), and self-rating depression scale(SDS) were applied for caregivers of all patients.Results(1) The scores of ACE-R, FBI, Cog12 and NPI in bvFTD group were significantly higher than those in AD group; And the scores of CBI, SAS and SDS in caregivers of bvFTD group were significantly higher than those in AD group. Moreover, the time-dependent burden and emotional burden of caregivers of bvFTD group were remarkably heavier than caregivers of AD group, while there were no significant differences in developmental burden, physical burden and social burden between two groups. (2) The scores of Cog-12, NPI and FBI showed a significant correlation with CBI in bvFTD group, while the scores of Cog-12, NPI showed a significant correlation with CBI in AD group. The scores of SAS or SDS and CBI correlated significantly. (3) The caregiver burden of bvFTD group was mainly due to on neuropsychiatric symptoms and behavior disorder, while the caregiver burden of AD group mainly resulted from neuropsychiatric symptoms.ConclusionsThe caregiver burden of patients with bvFTD are remarkably heavier than patients with AD, so the caregivers of bvFTD patients are vulnerable to depression or anxiety. The caregiver burden of patients with bvFTD is associated with neuropsychiatric symptoms and behavior disorder, while the caregiver burden of patients with bvFTD is associated with neuropsychiatric symptoms. Cog-12 is a reliable assessment tool suitable to assess caregiver burden indirectly. Professional health-care guidance, psychological support and other appropriate interventions should be planned. Only in this way can interventions that aim to reduce the caregiver burden be undertaken.
behavioral variant of frontotemporal dementia; Alzheimer’s disease; caregiver burden; brief cognitive impairment rating scale
国家自然科学基金(81471215,81271211);江苏省社会发展重点病种规范化诊疗项目(BE2015715);江苏省自然科学基金(BK20151592)
214500 江苏省泰州市,江苏省靖江市人民医院神经内科(汤群英);225001 江苏省扬州市,江苏省苏北人民医院神经内科(徐俊,胡月,李琳,陶带花,成佳星);重症医学科(顾小花);健康管理中心(洪音)
徐俊,Email:13611572068@126.com
R 749.16
A
10.3969/j.issn.1003-9198.2017.10.024
2017-05-15)
猜你喜欢
中老年保健(2022年2期)2022-08-24
中老年保健(2022年1期)2022-08-17
保健医苑(2022年5期)2022-06-10
——基于CFPS 2016年数据的实证分析
老龄科学研究(2021年10期)2021-11-04
中老年保健(2021年6期)2021-08-24
汉语世界(The World of Chinese)(2021年3期)2021-07-28
南方人口(2021年1期)2021-02-28
医学新知(2019年4期)2020-01-02
奥秘(2018年9期)2018-09-25
中国火炬(2015年6期)2015-07-31