氯吡格雷血小板反应性对经皮冠脉介入术后患者出血及缺血风险的评估效果
2020-10-09 10:29张剑波史琦玉胡亚民
中国当代医药 2020年22期
张剑波 史琦玉 胡亚民
[摘要]目的 探討氯吡格雷血小板反应性对经皮冠脉介入术(PCI)后患者出血及缺血事件的评估效果。方法 选取2017年1月~2018年1月沧州市中心医院收治的306例经PCI置入药物洗脱支架且术后48 h内进行了氯吡格雷血小板反应性测定的患者作为研究对象,所有患者平均氯吡格雷血小板反应性的值为(31.2±12.9)%。所有患者在术前及术后均服用阿司匹林和氯吡格雷。收集患者的基线资料及1年出血及缺血事件发生情况。结果 1年内,共35例(11.4%)患者发生出血事件,23例(7.5%)患者出现缺血事件。氯吡格雷血小板反应性对出血事件评价的受试者工作特征曲线下面积(AUROC)为0.88,敏感度和特异度分别为74.3%和89.3%,切点值为≤15.0%。氯吡格雷血小板反应性对缺血事件评价的AUROC为0.74,敏感度和特异度分别为73.9%和77.0%,切点值为>43.7%。氯吡格雷血小板反应性在≤15.0%、>15.0%~43.7%、>43.7%这三个区间内发生出血及缺血事件的人数分别为26和1例、9和5例、17和0例。结论 氯吡格雷血小板反应性对PCI后1年出血及缺血事件具有较好的评价效果,尤其是出血事件。但其治疗窗需要更进一步的研究来证实,从而为制定更加个性化的抗栓治疗策略提供依据。
[关键词]氯吡格雷血小板反应性;出血事件;血栓事件;经皮冠脉介入术后
[中图分类号] R541 [文献标识码] A [文章编号] 1674-4721(2020)8(a)-0008-04
Evaluated effect of Clopidogrel platelet reactivity on the risk of bleeding and ischemia in patients after percutaneous coronary intervention
ZHANG Jian-bo SHI Qi-yu HU Ya-min▲
The Sixth Department of Cardiology, Cangzhou Central Hospital, Hebei Province, Cangzhou 061000, China
[Abstract] Objective To investigate evaluated effect of Clopidogrel platelet reactivity on the risk of bleeding and ischemia events after percutaneous coronary intervention (PCI). Methods A total of 306 patients admitted to Cangzhou Central Hospital from January 2017 to January 2018 who had undergone PCI with drug-eluting stents and had undergone Clopidogrel platelet reactivity measurement within 48 hours after surgery were selected as the study subjects. The mean value of Clopidogrel platelet reactivity was (31.2±12.9)%. Aspirin and Clopidogrel before and after surgery were taken. Baseline information and the occurrence of bleeding and ischemia events were collected within 1 year. Results Within 1 year, bleeding events merged in 35 patients (11.4%), with ischemia events in 23 patients (7.5%). The area under the receiver operating characteristic curve (AUROC) of Clopidogrel platelet reactivity for bleeding events was 0.88, sensitivity and specificity were 74.3% and 89.3%, respectively, and the cut-off value was ≤15.0%. The AUROC of Clopidogrel platelet reactivity for ischemic events was 0.74, sensitivity and specificity were 73.9% and 77.0%, respectively, and the cut-off value was >43.7%. The number of Clopidogrel platelet reactivity in the three intervals ≤15.0%, >15.0%-43.7%, >43.7% occurring bleeding and ischemic events was 26 and 1, 9 and 5, 17 and 0, respectively. Conclusion Clopidogrel platelet reactivity presents good evaluated performance for bleeding and ischemic events in 1 year after PCI, especially for bleeding events. However, its therapeutic window needs to be further verifyed, so as to provide evidence for more individualized antithrombotic strategies.
[Key words] Clopidogrel platelet reactivity; Bleeding events; Thrombosis events; After percutaneous coronary intervention
冠状动脉粥样硬化性心脏病是当今威胁人类健康最重要的疾病之一。经皮冠脉介入术(percutaneous coronary intervention,PCI)是治疗冠心病的重要手段[1]。PCI后联合服用阿司匹林和以氯吡格雷为代表的P2Y12受体拮抗剂的双抗治疗是预防术后缺血事件发生的重要措施,但同时也增加了出血风险[2]。氯吡格雷的抗血小板效应在不同患者中有所差别,称为血小板多反应性(VPR)。氯吡格雷血小板反应性的检测,即血小板功能检测,是对服用氯吡格雷后血小板残余反应性进行测定以了解患者对抗栓治疗的反应性,从而评估PCI后双抗治疗的出血及缺血风险。抗血小板治疗后氯吡格雷血小板高反应性(HPR)者,体内血小板聚集抑制率下降,发生支架内血栓等缺血事件的风险增加。氯吡格雷血小板低反应性(LPR)者,体内血小板聚集抑制率升高,发生消化道出血等风险增加[3-5]。但以上研究对象多为欧美人群且多聚焦于术后缺血事件,而对出血事件的研究较少,故本研究通过回顾性分析PCI后进行双抗治疗患者出血及缺血事件的发生情况,探讨氯吡格雷血小板反应性对患者出血及缺血事件的评估效果,现报道如下。
1资料与方法
1.1一般资料
回顾性收集2017年1月~2018年1月于沧州市中心医院心内科因急性冠脉综合征(acute coronary syndrome,ACS)行PCI成功置入药物洗脱支架的306例患者,其中男144例,女162例;平均年龄(61.5±9.5)岁;平均体重指数(body mass index,BMI)(25.4±2.6)kg/m2;42例(13.7%)患者曾有心肌梗死病史,170例(55.6%)为ST抬高型心肌梗死;平均接受治疗的血管数及置入的支架数分别为(1.5±0.6)和(1.6±0.5);平均氯吡格雷血小板反应性的值为(31.2±12.9)%。
纳入标准:①所有患者在术前连续服用常规剂量阿司匹林(100 mg/d)和氯吡格雷(75 mg/d)5 d,或术前口服负荷剂量阿司匹林300 mg和氯吡格雷300 mg;②PCI后48 h内对患者进行氯吡格雷血小板反应性测定;③PCI后服用阿司匹林(100 mg/d)联合氯吡格雷(75 mg/d);④ACS的诊断符合2013年及2014年美国ACS防治指南的诊断标准[6-7]。排除标准:①临床资料不完整的患者;②术中及术后48 h内应用替罗非班的患者;③入院前长期服用抗血小板药物的患者;④房颤患者;⑤长期服用抗凝药物的患者;⑥血小板计数<70×109/L的患者;⑦严重肝肾功能损害的患者;⑧伴有外伤、外科手术及败血症的患者;⑨有恶性肿瘤史、血液病史、近期有严重出血病史的患者。本研究经沧州市中心医院医学伦理委员会批准。
1.2方法
氯吡格雷血小板反应性测定采用新型的PL-11血小板分析仪(南京神州英诺华医疗科技有限公司),其以血细胞分析仪为基础,基于库尔特原理的连续自动技术,以“全血连续计数法”原理来动态监测激活前后血小板数量变化,并计算出血小板聚集率。测量时使用微量加样器吸取充分混匀的0.4 ml枸橼酸盐抗凝全血两管加至PL-11检测试管,在诱聚剂诱导下开始自动检测。全血标本经2次血小板基础值计数后,加入诱聚剂(终浓度为4 mmol/L),并连续间隔一定时间对血标本中血小板计数,当得到最低血小板计数时结果自动换算,评价血小板聚集率。最大血小板聚集率(MAR)=(初始血小板数-最低血小板数)/初始血小板数×100%。
1.3观察指标及评价标准
(1)出血事件。依据TIMI出血分级标准[8]:①主要出血:颅内出血或临床可见出血(包括影像学诊断),伴血红蛋白(HGB)下降≥50 g/L;②小出血:临床可见出血(包括影像学诊断),伴HGB下降30~<50 g/L;③轻微出血:临床可见出血(包括影像学诊断),HGB下降<30 g/L。
(2)缺血事件。心绞痛,再次血运重建,支架内血栓形成,再发心肌梗死及心源性死亡。根据学术研究联盟(ARC)的标准将支架内血栓形成定义为肯定的、可能的或不能排除的支架内血栓形成[9]。心肌梗死定义同第3版心肌梗死全球定义[10],即血清心肌标志物(主要是肌钙蛋白)升高(至少超過99%参考值上限),并至少伴有以下l项临床指标:①缺血症状;②新发生的缺血性心电图改变;③心电图病理性Q波形成;④影像学证据显示有新的心肌活性丧失或新发的局部室壁运动异常;⑤冠状动脉造影或尸检证实冠状动脉内有血栓。
1.4统计学方法
采用SPSS 15.0(Chicago,USA)、Medcalc 9.3(Medcalc Software,Mariakerke,Belgium)统计学软件进行数据分析,计量资料用均数±标准差(x±s)表示,采用受试者工作特征(receiver operator characteristic,ROC)曲线及ROC曲线下面积(area under the ROC,AUROC)评价诊断效力,计算其切点值、精确度、敏感度及特异度。采用柱形图表示依据不同切点值进行分组后,每组的出血及血栓事件。
2结果
2.1患者出血及缺血事件发生情况
PCI后1年内,共35例(11.4%)患者发生出血事件,23例(7.5%)患者出现缺血事件。
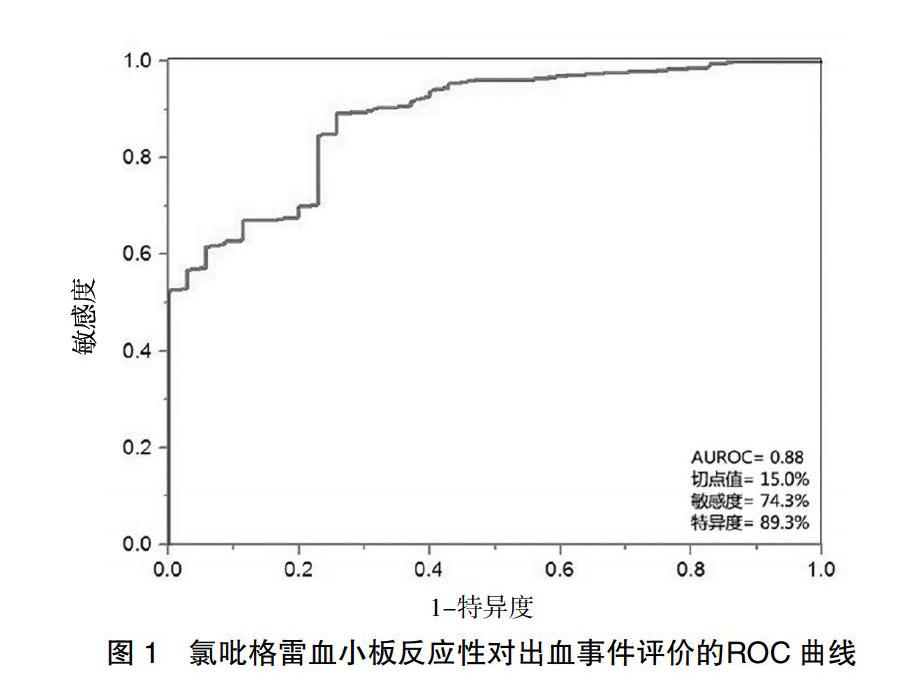
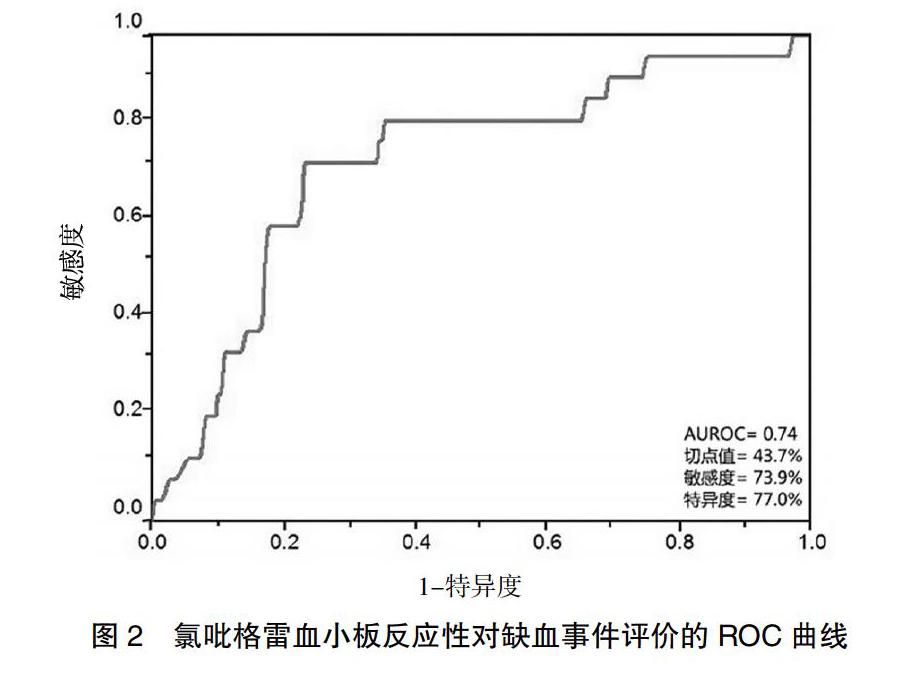
2.2氯吡格雷血小板反应性对出血及缺血事件的评价
氯吡格雷血小板反应性对出血事件评价的AUROC为0.88,敏感度和特异度分别为74.3%和89.3%,切点值为≤15.0%(图1)。氯吡格雷血小板反应性对缺血事件评价的AUROC为0.74,敏感度和特异度分别为73.9%和77.0%,切点值为>43.7%(图2)。
[6]O′Gara PT,Kushner FG,Ascheim DD,et al.2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction[J].J Am Coll Cardiol,2013,61(4):e78-140.
[7]Amsterdam EA,Wenger NK,Brindis RG,et al.2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronarysyndromes:a report of the American College ofCardiology/American Heart Association Task Forceon Practice Guidelines[J].J Am Coll Cardiol,2014,64(24):e139-228.
[8]Wiviott SD,Antman EM,Gibson CM,et al.Evaluation of Prasugrel Compared With Clopidogrel in Patients With Acute Coronary Syndromes: Design and Rationale for the TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioN With Prasugrel Thrombolysis In Myocardial Infarction 38(TRITON-TIMI 38)[J].Am Heart J,2006,152(4):627-635.
[9]Cutlip DE,Windecker S,Mehran R,et al.Clinical end points in coronary stent trials:a case for standardized definitions[J].Circulation,2007,115(17):2344-2351.
[10]Thygesen K,Alpert JS,Jaffe AS,et al.Third universal definition of myocardial infarction[J].Eur Heart J,2012,33(20):2551-2567.
[11]Levine GN,Bates ER,Bittl JA,et al.2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease:A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J].J Thorac Cardiovasc Surg,2016,152(5):1243-1275.
[12]徐娜,袁晉青.血小板功能检测对冠心病患者抗血小板治疗出血事件的预测价值[J].中国循环杂志,2017,32(2):193-196.
[13]Gross L,Aradi D,Sibbing D.Platelet function testing in patients on antiplatelet medications[J].Semin Thromb Hemost,2016,42(3):306-320.
[14]Spiliopoulos S,Pastromas G.Current status of high on-treatment platelet reactivity in patients with coronary or peripheral arterial disease:Mechanisms,evaluation and clinical implications[J].World J Cardiol,2015,7(12):912-921.
[15]Collet JP,Cuisset T,Range G,et al.Bedside monitoring to adjust antiplatelet therapy for coronary stenting[J].N Engl J Med,2012,367(22):2100-2109.
[16]Sibbing D,Schulz S,Braun S,et al.Antiplatelet effects of clopidogrel and bleeding in patients undergoing coronary stent placement[J].J Thromb Haemost,2010,8(2):250-256.
[17]Breet NJ,van Werkum JW,Bouman HJ,et al.Comparison of platelet function tests in predicting clinical outcome in patients undergoing coronary stent implantation[J].JAMA,2010,303(8):754-762.
[18]孙彬,周杏,朱蕾,等.新型血小板功能分析仪PL-11监测血小板聚集功能的应用价值[J].标记免疫分析与临床,2015,22(6):569-576.
[19]Choi SY,Kim MH,Serebruany V.The challenge for predicting bleeding events by assessing platelet reactivity following coronary stenting[J].Int J Cardiol,2016,207(1):128-131.
[20]Bonello L,Mancini J,Pansieri M,et al.Relationship between post-treatment platelet reactivity and ischemic and bleeding events at 1-year follow-up in patients receiving prasugrel[J].J Thromb Haemost,2012,10(10):1999-2005.
(收稿日期:2019-12-09)