
下颌神经管在下颌磨牙区CBCT横截面的可见性分析
2016-12-08 06:29陈闰香蒋娟雯潘志文
浙江临床医学 2016年10期
陈闰香 蒋娟雯 潘志文
下颌神经管在下颌磨牙区CBCT横截面的可见性分析
陈闰香蒋娟雯潘志文
目的 分析下颌神经管在下颌磨牙区锥体束CT(CBCT)横截面中的可见性,并分析其可见性在年龄、性别及左右侧方面是否有显著性差异。方法 按纳入标准收集临床拍摄的110例患者的CBCT影像资料,由三名口腔医生对双侧下颌第一磨牙及第二磨牙区域的CBCT横截面进行评阅。横截面中下颌神经管的可见性分为容易辨认、大致可辨和无法辨认三个等级,结果进行统计学分析。结果 下颌第一磨牙及第二磨牙区域CBCT横截面中下颌神经管容易辨认、大致可辨和无法辨认的总体比率分别为48.41%、33.87%、17.73%;不同磨牙位置组及不同性别组之间下颌神经管可见性差异无统计学意义(P>0.05);20~30岁年龄组不同部位下颌神经管可见性差异有统计学意义(P<0.05)。结论 大部分患者牙种植术前可通过CBCT横截面辨认其下颌神经管的位置,为治疗提供重要参考,但仍有部分患者无法通过CBCT横截面明确其下颌神经管的位置,临床需仔细分析。年龄和左右侧可能是影响下颌神经管可见性的因素。
下颌神经管 锥体束CT 可见性
下颌神经管是下颌后牙区进行种植牙手术需要避开的重要解剖结构,牙种植体过于接近下颌神经管可导致其内血管损伤及下牙槽神经损伤,产生出血、下唇麻木等并发症。因此,种植牙术前下颌神经管的准确定位及下颌神经管上方骨质的精确测量非常重要。可用于种植牙术前测量分析的方法有全景片、计算机体层摄影、锥体束CT(CBCT),甚至MRI[1]。有文献报道CBCT可以完全清晰地显示下颌神经管[2],有的学者认为下颌神经管仅在半数患者的CBCT中可辨认,不同文献报道可辨认的比率差异较大[3-5],且尚无文献报道国人下颌神经管在CBCT横截面中的可见性。本研究通过分析110例患者的CBCT影像资料,旨在阐明国人下颌磨牙区(下颌牙种植最多的区域)CBCT横截面中下颌神经管的可见性及其影响因素。

图1 下颌磨牙区CBCT横截面中下颌神经管
1 临床资料
1.1一般资料 从浙江省口腔医院2013年1月至2015年12月放射科拍摄的CBCT影像资料中按以下选片标准筛选。纳入标准:(1)年龄>18周岁。(2)双侧下颌骨扫描完整。排除标准:(1)图像晃动模糊。(2)明显颅颌面畸形。(3)双侧下颌第二前磨牙至第二磨牙连续缺失或重度拥挤。(4)双侧下颌后牙区颌骨病变。(5)下颌神经管存在分支或副管。共筛选出110例资料,其中男52例,女58例,年龄18~44岁。影像拍摄仪器为CBCT(New Tom 3G,意大利,轴位间距0.29mm,轴位宽度0.29mm,FSV:110KV,FSV:5.94mA,SSV:110KV,SSV:1.16mA,FOV:9″,曝光时间:9.0s)。1.2 方法 将观察对象的DICOM影像文件导入三维软件(InVivo Dental,Anatomage,San Jose,Calif)。根据Jung等的研究方法将下颌神经管可见性分为容易辨认、大致可辨和无法辨认三个等级[6]。若能通过一张横截面直接辨认下颌神经管的位置定为“容易辨认”;若需通过多张连续横截面反复辨认,定为“大致可辨”;若通过多张横截面反复辨认亦无法确定下颌神经管的位置,则定为“无法辨认”。初始横截面定为下颌磨牙根分叉处。阅片由经验丰富的一位口腔放射医生及一位口腔外科医生各自独立完成,对比结果,存在分歧处由另一位经验更丰富的外科医生阅片。每例资料阅读右侧第一磨牙、右侧第二磨牙、左侧第一磨牙、左侧第二磨牙四个区域CBCT横截面中下颌神经管的显示情况,共获得440份阅片结果。
1.3统计学分析 采用SPSS 16.0 统计软件包。计数资料比较采用χ2检验,P<0.05为差异有统计学意义。
2 结果
2.1总体特征 110例观察对象,平均年龄25.70岁(SD=6.74)。下颌第一磨牙区域CBCT横截面中下颌神经管容易辨认、大致可辨和无法辨认率分别为45%(98/220)、35%(77/220)、20%(45/220);下颌第二磨牙区域CBCT横截面中下颌神经管容易辨认、大致可辨和无法辨认率分别为52%(115/220)、33%(72/220)、15%(33/220);总体容易辨认、大致可辨和无法辨认率分别为48.41%(213/440)、33.87%(149/440)、17.73%(78/440)。
2.2不同性别、年龄、磨牙位置、左右侧组下颌神经管的可见性 不同性别组及不同磨牙位置组CBCT横截面中下颌神经管的可见性差异无统计学意义(P>0.05);然而在不同年龄组及左右侧CBCT横截面中下颌神经管的可见性差异有统计学意义(P<0.05)。见表1。
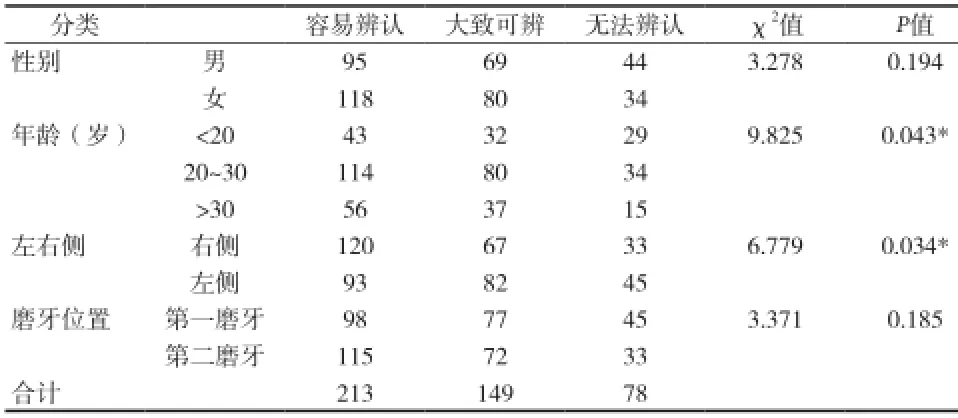
表1 不同性别、年龄、左右侧、磨牙位置的下颌神经管的可见性分析(n)
2.3不同部位CBCT横截面中下颌神经管可见性在不同性别、不同年龄组的差异分析 右侧第一磨牙、右侧第二磨牙、左侧第一磨牙、左侧第二磨牙的CBCT横截面中下颌神经管的可见性在男性对象、女性对象中差异均无统计学意义(P>0.05);在<20岁和>30岁年龄组中差异均无统计学意义(P>0.05),然而在20~30岁年龄组对象中差异有统计学意义(P<0.05)。见表2。

表2 不同部位CBCT横截面中下颌神经管可见性在不同性别、不同年龄组的差异分析
3 讨论
CBCT因其放射剂量小,图像无放大缩小,可查看任意截面及三维重建等性能,已在临床牙种植术前分析中显示出明显优势,同时也为临床研究提供了大量资料。
影响下颌神经管在影像中可见性的因素可从以下几方面分析:(1)拍摄过程,包括拍摄仪器、参数设置等。CBCT拍摄体素是影响影像分辨率的重要因素,较低的体素可获得较高分辨率的图像。Waltrick等[7]认为体素设定为0.3mm,是低放射剂量和较好的影像质量的最佳折衷办法,建议临床选用。多种阅片软件、硬件及不同的阅片方法也可能在一定程度上影响下颌神经管可见性的判定。(2)种族及个体差异。不同种族之间下颌神经管可见性差异尚未有研究报道,个体差异已有部分报道。Carter & Keen(1970)的研究发现部分人的下颌神经血管束可发出分支,或者形成血管神经丛,因而不可能有清晰可见的皮质管[8]。Shokri等[3]的研究结果表明其观察对象中仅56.3%的下颌神经管皮质骨化,且不一定是规则的形态[6,9]。下颌神经管壁无皮质骨化也并非不能将其辨认出。De Oliveira-Santos等[10]研究结果显示41%的下颌神经管无皮质骨化,但这其中有超过半数的下颌神经管可以辨认出位置。主要通过以下两方面辨认:一是下颌神经管的透射性与周围骨小梁影像的差异;二是部分下颌神经管在靠舌侧行走时在下颌骨舌侧骨皮质表面形成了骨凹[3-4]。
本资料中通过分析110例患者下颌磨牙区的CBCT影像资料,揭示了国人临床CBCT中下颌磨牙区下颌神经管的显示情况。结果表明:下颌磨牙区下颌神经管总体可见性为48.41%(213/440)容易辨认,33.87%(149/440)大致可辨、17.73%(78/440)无法辨认。下颌第一磨牙和第二磨牙区域下颌神经管的可见性差异无统计学意义(P>0.05),20~30岁年龄组对象中左右侧下颌神经管可见性差异有统计学意义(P<0.05),其他年龄组左右侧差异无统计学意义(P>0.05)。另外,结果显示性别不影响下颌神经管的可见性,这可能与观察对象的年龄分布等有关。综上所述,国人大部分患者牙种植术前可通过CBCT横截面辨认其下颌神经管的位置,为治疗提供重要参考,但仍有部分患者通过CBCT横截面无法明确其下颌神经管的位置,临床需注意。年龄和左右侧可能是下颌神经管可见性的影响因素。
[1]Imamura H, Sato H, Matsuura T, et al. A comparative study of computed tomography and magnetic resonance imaging for the detection of mandibular canals and cross-sectional areas in diagnosis prior to dental implant treatment.Clin Implant Dent Relat Res, 2004, 6(2):75-81.
[2]Angelopoulos C, Thomas SL, Hechler S, et al. Comparison between digital panoramic radiography and conebeam computed tomography for the identification of the mandibular canal as part of presurgical dental implant assessment.J Oral Maxillofac Surg, 2008, 66(10): 2130-2135.
[3]Shokri A,Shakibaei Z,Langaroodi A J,et al.Evaluation of the mandibular canal visibility on cone-beam computed tomography images of the mandible.J Craniofac Surg,2014,25(3):e273-e277.
[4]Oliveira-Santos C, Capelozza AL, Dezzoti MS, et al. Visibility of the mandibular canal on CBCT cross-sectional images.J Appl Oral Sci, 2011,19(3):240-243.
[5]Miles MS, Parks ET, Eckert GJ, et al. Comparative evaluation of mandibular canal visibility on cross-sectional cone-beam CT images:a retrospective study.Dentomaxillofac Radiol, 2016, 45(2): 20150296.
[6]Jung YH, Cho BH. Radiographic evaluation of the course and visibility of the mandibular canal. Imaging Sci Dent, 2014, 44(4): 273-278.
[7]Waltrick KB, Nunes MJ, Correa M, et al. Accuracy of linear measurements and visibility of the mandibular canal of cone-beam computed tomography images with different voxel sizes:an in vitro study. J Periodontol,2013,84(1):68-77.
[8]Carter RB,Keen EN.The intramandibular course of the inferior alveolar nerve.J Anat,1971,108(Pt 3):433-440.
[9]De Vos W,Casselman J,Swennen GR.Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region:a systematic review of the literature.Int J Oral Maxillofac Surg,2009,38(6):609-625.
[10]De Oliveira-Santos C, Souza PH, De Azambuja BS, et al. Assessment of variations of the mandibular canal through cone beam computed tomography.Clin Oral Investig,2012,16(2):387-393.
Objective To analyze the visibility of the mandibular canal in mandibular molar areas on cone beam computed tomography(CBCT)cross-sectional images. Methods CBCT images of 110 patients were in accordance with the inclusive criteria. These images were evaluated by one experienced oral radiologist and one experienced dentist.The visibility of the mandibular canal in mandibular molar areas was recorded as easily identifiable,probably identifiable and unidentifiable.And then the data was statistically analyzed. Results On cone beam computed tomography(CBCT)cross-sectional images in the area of mandibular fi rst molar and second molar,the mandibular canal was easily identifi able in 48.41% of the hemi-mandibles,probably identifiable in 33.87% of the hemi-mandibles,and unidentifiable in 17.73% of the hemi-mandibles. No significant difference was detected between mandibular fi rst molar and second molar areas,as well as between men and women. Signifi cant difference was detected between left and right sides as well as age group 20-30 years old. Conclusions In most patients,the mandibular canal in mandibular molar areas can be identifi ed in CBCT cross-sectional images,which provides useful information for clinical treatment;however,we must be more careful when the mandibular canal is unidentifi able in some patients. And age and side may be factors associated with the visibility of the mandibular canal.
Mandibular canal Cone beam computed tomography(CBCT)visibility
310007 杭州市中医院口腔科(陈闰香 蒋娟雯)
310006 浙江大学医学院附属口腔医院放射科(潘志文)
猜你喜欢
口腔医学(2021年10期)2021-12-02
河南医学研究(2021年35期)2021-01-05
中国生育健康杂志(2020年1期)2020-12-31
爱你·健康读本(2019年11期)2019-12-10
中国CT和MRI杂志(2018年12期)2018-12-13
人人健康(2018年3期)2018-03-24
儿童故事画报·发现号趣味百科(2016年7期)2017-02-08
中华老年口腔医学杂志(2016年5期)2016-03-01
中国医疗美容(2015年1期)2015-07-12
中国当代医药(2015年32期)2015-03-01
