淡蓝色嵴对Barrett食管及胃黏膜肠上皮化生诊断价值的Meta分析
2013-04-18 08:54王蕾陈有为杨建民黄伟
浙江医学 2013年23期
王蕾 陈有为 杨建民 黄伟
淡蓝色嵴对Barrett食管及胃黏膜肠上皮化生诊断价值的Meta分析
王蕾 陈有为 杨建民 黄伟
目的 系统评价窄带成像结合放大内镜观察淡蓝色嵴对诊断Barrett食管及胃黏膜肠上皮化生的诊断价值。 方法收集关于淡蓝色嵴对诊断Barrett食管及胃黏膜肠上皮化生准确性研究的文献,进行Meta分析。 结果 4篇文献(包含285例患者的854例标本)纳入异质性分析,以同质性较高的3篇文献,包括247例患者的626例标本进行合并分析,合并敏感度0.895(95%CI:0.861~0.923)、特异度0.900(95%CI:0.862~0.931)、SROC曲线下面积0.957。 结论 窄带成像结合放大内镜观察淡蓝色嵴对诊断胃黏膜肠上皮化生具有较高的敏感度及特异度。
窄带成像 放大内镜 淡蓝色嵴 肠上皮化生
上消化道黏膜,如食管、胃黏膜出现肠上皮化生(intestinal metaplasia,IM)被认为是癌前状态[1-2]。对癌前状态进行监测能够早期发现病灶的进展,对肿瘤进行早期干预可以提高患者的生存期[3]。IM分布呈局灶性,且在白光胃镜下缺乏特异表现,内镜诊断率偏低,而传统活检由于具有一定盲目性,阳性率亦不高[4-5]。窄带成像(narrow band imaging,NBI)通过滤光片对蓝绿光进行窄化,可在内镜视野下突显黏膜血管网及黏膜表面结构等组织细节,从而提高内镜对病灶的诊断价值[6-7]。淡蓝色嵴(light blue crest,LBC)是指NBI联合放大内镜(NBI-magnification endoscopy,NBI-ME)下黏膜表面蓝白相间的斑驳区,被认为可能是IM的内镜下特异表现[4,8]。本文通过Meta分析讨论LBC对诊断Barrett食管、胃黏膜IM的敏感度及特异度,现报道如下,以期为临床提供参考。
1 资料和方法
1.1 文献检索 我们检索了截止至2013年3月的Pubmed、Embase、Web of Science及Cochrane library、万方、维普、CNKI等中外文献数据库,检索词为"narrow band imaging"与 "intestinal metaplasia"及"diagnosis"或者"intestinal metaplasia"与"light blue crest"。所有语言的文献均纳入检索范围。为尽量减少漏查文献,对已检索文献中提供的参考文献进行二次检索。采用以下标准对搜索文献进行筛选。纳入标准:(1)研究目的为LBC与Barrett食管、胃黏膜IM诊断符合率;(2)以悉尼标准或中国慢性胃炎共识为病理诊断标准;(3)所有研究对象均进行了NBI-ME检查及病理检查,并以LBC有或无为内镜诊断IM的标准;(4)受检人群为非特定人群;(5)能直接或间接获得LBC诊断IM的真阳性、假阳性、真阴性和假阴性值。排除标准:(1)研究对象为特殊人群,限制年龄、性别及病因;(2)文摘、综述、讲座及述评类文献;(3)未标明诊断标准或诊断标准不符的文献。
1.2 诊断标准
1.2.1 IM在NBI-ME下诊断标准 NBI-ME下任何区域见到LBC,即内镜下诊断为IM;如无,则诊断为非IM[4]。
1.2.2 IM的病理标准 IM的病理诊断标准依据新悉尼标准的直观图评价,由于中国慢性胃炎共识标准直观图评价与新悉尼标准完全一致,采用这一病理诊断标准的文献同样允许纳入[9-10]。
1.3 文献质量评价 根据QUADAS-2文献质量评价工具[11]对入选文献质量进行评估。根据QUADAS-2结合本研究实际设计评价文献质量的表格。由2位评价者独立进行文献检索、纳入及评价,遇有分歧时讨论解决。
1.4 统计学处理 采用Meta-Disc软件分别计算Spearman及Cochran-Q讨论阈值及非阈值效应导致的异质性,如提示有异质性,则采用随机效应模型进行Meta分析,如无异质性,则采用固定效应模型进行Meta分析。Meta分析按照相应的效应模型。计算LBC对IM的合并敏感度、特异度、阳性似然比、阴性似然比。使用Meta-Disc软件绘制SROC曲线,并计算合并SROC曲线下面积。
2 结果
2.1 入选文献结果 初步检出文献158篇,排除综述、与本研究目的不相关文献143篇,进一步阅读全文15篇[4-5,8,12-23],排除会议摘要 4篇[15,20-21,23],无关文献 3篇[5,14,22],未达到纳入标准文献4篇(其中1篇未说明病理诊断标准[8],2篇诊断标准与本研究不符合[16,18],1篇未行ME检查[17]),最终纳入4篇[4,12-13,19]。其中探索性研究[4]及第二次随访的病例[19]亦未纳入研究。纳入文献具体资料见表1。

表1 纳入文献具体资料
2.2 文献质量评估结果 见表2。

表2 纳入文献质量评价
由表2可见,4篇文献均具有较高的文献质量。
2.3 Meta分析结果 4篇文献(包含285例患者的854例标本)最终纳入Meta分析。对这4篇文献进行异质性检验,阈值效应Spearman相关系数=-0.200,P=0.800,非阈值效应Cochran-Q=21.99,P=0.001,提示存在非阈值效应性异质性。应用随机效应模型行SROC曲线分析(图1),发现1篇文献[19]与其余3篇存在明显的偏移,将其剔除之后,对剩余3篇文献进行异质性检验,提示无明确阈值效应及非阈值效应异质性,对其应用固定效应模型分析,发现合并敏感度0.895(95%CI:0.861~0.923)、特异度0.900(95%CI:0.862~0.931)、阳性似然比8.985(95%CI:6.420~12.575)、阴性似然比0.117(95%CI:0.088~0.155),SROC曲线下面积0.9571(图2)。
3 讨论
上消化道黏膜IM被公认为癌前状态,需正确诊断及长期随访。基于新悉尼系统的IM病理诊断标准被认为是其诊断的金标准,而内镜下IM诊断准确性一直不高。Kaminishi等[24]发现传统内镜下胃黏膜的灰色结节对诊断IM的特异度较强(98%~99%),但敏感度较低(6%~12%)。后期发展的ME联合亚甲蓝染色能克服传统胃镜诊断IM的不足[25],但是这种方法非常耗时,且染料可能会导致细胞DNA损伤[26],不适于大规模应用。NBI依据光学原理直接在镜下观察黏膜细节,为改善内镜下IM诊断提供了可能。因此,我们以研究NBI下IM特异表现——LBC诊断准确性为目的,对相关文献进行了收集整理及分析,获得了较高的敏感度及特异度,SROC曲线下面积亦较大(均较接近1),提示LBC作为NBI-ME下IM的诊断标准准确性较高,存在进一步推广价值。
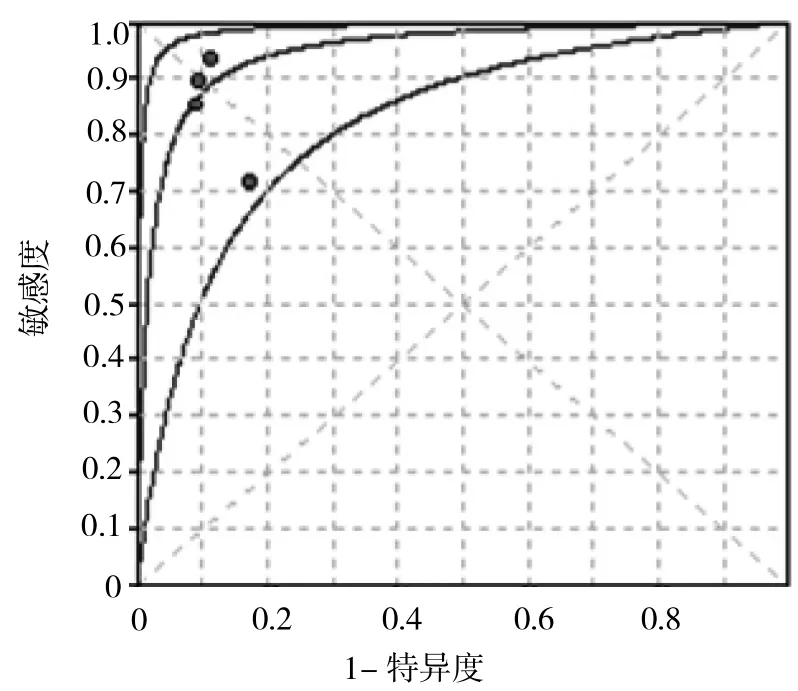
图1 4项研究的操作者曲线

图2 3项研究的操作者曲线
但是,其作为新的技术及诊断方式,仍存在一些问题需要进一步改进。
首先,NBI下诊断IM的标准尚不确定。在纳入全文阅读的文献中,有文献采取了不同标准。一项研究以LBC范围在每视野>10%为LBC阳性的判定指标,得出其敏感度72.1%,特异度96%,准确性为84.5%[16]。另一项研究以LBC伴不规则黏膜形态为标准,得出敏感度、特异度分别为71%及58%[18]。LBC阳性的判断标准差异及是否合并黏膜及微血管形态改变可能导致对IM诊断灵敏度及特异度的差异,因此,临床中进行更大规模的对比研究以进一步探讨及统一LBC的判断标准是必要的。
其次,纳入文献存在异质性。最终纳入的4篇文献存在明显异质性,依据ROC曲线分析发现,来自泰国的1篇文献偏移明显[19],将其剔除后,剩余3篇来自中国和日本的文献同质性较好,LBC诊断IM的合并灵敏度及准确度均较4篇为高。该偏移可能与其所选取的人种差异及内镜使用差异相关,亦有可能有其他存在因素如医师的训练水平等与之相关,需要更多的文献以进一步探讨。
再次,LBC对食管黏膜IM的诊断是否与胃黏膜相同尚未确定。我们在检索文献中仅找到1篇LBC对 Barretr食管合并IM诊断的文献[8],敏感度、特异度及准确性分别为79%、97%及89%。LBC对于诊断Barretr食管伴IM同样存在较高准确性,但需要更多研究进一步加以证实。
总之,通过本Meta分析,我们认为NBI-ME观察LBC对诊断消化道黏膜IM具有较高的敏感度及特异度,应用这一诊断方法,可以提高内镜下消化道黏膜IM的诊断率,指导内镜下活检,提高病理活检的阳性率。
[1]Correa P.A human model of gastric carcinogenesis[J].Cancer Res,1988,48(13):3554-3560.
[2] 房殿春,林三仁,于中麟,等.Barrett食管诊治共识(修订版)[J],胃肠病学, 2011,16(8):485-486.
[3]de Vries A C,van Grieken N C,Looman C W,et al.Gastric cancer risk in patients with premalignant gastric lesions:a nationwide cohort study in the Netherlands[J].Gastroenterology,2008,134(4): 945-952.
[4]Uedo N,Ishihara R,Iishi H,et al.A new method of diagnosing gastric intestinal metaplasia:narrow-band imaging with magnifying endoscopy[J].Endoscopy,2006,38(8):819-824.
[5]Anagnostopoulos G K,Yao K,Kaye P,et al.Novel endoscopic observation in Barrett's oesophagus using high resolution magnification endoscopy and narrow band imaging[J].Alimentary pharmacology&therapeutics,2007,26(3):501-507.
[6]Wong Kee Song L M,Adler D G,Conway J D,et al.Narrow band imaging and multiband imaging[J].Gastrointestinal Endoscopy, 2008,67(4):581-589.
[7]Gono K,Obi T,Yamaguchi M,et al.Appearance of enhanced tissue features in narrow-band endoscopic imaging[J].Journal of biomedical optics,2004,9(3):568-577.
[8]Norimura D,Isomoto H,Nakayama T,et al.Magnifying endoscopic observation with narrow band imaging for specialized intestinal metaplasia in Barrett's esophagus with special reference to light blue crests[J].Digestive Endoscopy,2010,22(2):101-106.
[9]Dixon M F,Genta R M,Yardley J H,et al.Classification and grad-ing of gastritis:the updated Sydney system[J].The American journal of surgical pathology,1996,20(10):1161-1181.
[10]林三仁,于中麟,胡品津,等.全国慢性胃炎研讨会共识意见[J].现代消化及介入诊疗,2000,5(2):1-4.
[11]Whiting P F,Rutjes A W S,Westwood M E,et al.QUADAS-2:a revised tool for the quality assessment of diagnostic accuracy studies[J].Annals of Internal Medicine,2011,155(8):529-536.
[12] 周颖,周忠杰,赵佳宏.窄带成像放大内镜在胃黏膜肠上皮化生随访中的应用[J].胃肠病学,2012,17(1):36-38.
[13]刘变英,王颖,雷宇锋,等.内镜窄带成像技术诊断胃黏膜肠上皮化生的临床应用价值[J].中华消化杂志,2009,29(5):293-295.
[14]Ang T L,Fock K M,Teo E K,et al.The diagnostic utility of narrow band imaging magnifying endoscopy in clinical practice in a population with intermediate gastric cancer risk[J].European journal of gastroenterology&hepatology,2012,24(4):362-367.
[15]Corbo M,Dulbecco P,Gemignani L,et al.The Diagnostic Value of Narrow-Band Imaging With Magnifying Endoscopy in the Detection of Gastric Intestinal Metaplasia:A Prospective Study in an Unselected Population[J].Gastroenterology,2012,142(5): 335.
[16]An J K,Song G A,Kim G H,et al.Marginal turbid band and light blue crest,signs observed in magnifying narrow-band imaging endoscopy,are indicative of gastric intestinal metaplasia[J]. BMC gastroenterology,2012,12(1):169-174.
[17]Pimentel-Nunes P,Dinis-Ribeiro M,Soares J B,et al.A multicenter validation of an endoscopic classification with narrow band imaging for gastric precancerous and cancerous lesions [J].Endoscopy,2012,44(3):236-246.
[18]Capelle L G,Haringsma J,de Vries A C,et al.Narrow band imaging for the detection of gastric intestinal metaplasia and dysplasia during surveillance endoscopy[J].Digestive diseases and sciences,2010,55(12):3442-3448.
[19]Rerknimitr R,Imraporn B,Klaikeaw N,et al.Non-sequential narrow band imaging for targeted biopsy and monitoring of gastric intestinal metaplasia[J].World journal of gastroenterology,2011, 17(10):1336.
[20]Boonlert I,Sukprasert J,Naruemon W,et al.One Year Follow-Up Results of Magnify NBI for Gastric Intestinal Metaplasia Surveillance[J].Gastrointestinal Endoscopy,2009,69(5):182.
[21]Wang A Y,Patrie J T,Cox D G,et al.Single-Operator Experience in Detecting Gastritis,Helicobacter Pylori Infection,Gastric Intestinal Metaplasia,and Dysplasia Before and After Training in Narrow-Band Imaging[J].Gastrointestinal Endoscopy,2010,71 (5):AB362.
[22]Sharma P,Hawes R H,Bansal A,et al.Standard endoscopy with random biopsies versus narrow band imaging targeted biopsies in Barrett's oesophagus:a prospective,international,randomised controlled trial[J].Gut,2013,62(1):15-21.
[23]Imraporn B,Jutaghokiat S,Wisedopas N,et al.Validity of Magnify NBI for Gastric Intestinal Metaplasia Targeted Biopsy[J]. Gastrointestinal Endoscopy,2008,67(5):AB280.
[24]Kaminishi M,Yamaguchi H,Nomura S,et al.Endoscopic classification of chronic gastritis based on a pilot study by the Research Society for Gastritis[J].Dig Endosc,2002,14:138-151.
[25]Dinis-Ribeiro M,da Costa-Pereira A,Lopes C,et al.Magnification chromoendoscopy for the diagnosis of gastric intestinal metaplasia and dysplasia[J].Gastrointest Endosc,2003,57: 498-504.
[26]Olliver J R,Wild C P,Sahay P,et al.Chromoendoscopy with methylene blue and associated DNA damage in Barrett's oesophagus[J].Lancet,2003,362(9381):373-374.
Meta-analysis of diagnostic value of light blue crest for detecting intestinal metaplasia in Barrett's esophageal and gastric mucosa
Objective To access the diagnostic value of light blue crest(LBC)observation by magnification endoscopy (NBI-ME)combined with narrow band imaging for detecting intestinal metaplasia(IM)in Barrett's esophageal and gastric mucosa. Methods A meta-analyis was performed to evaluate the research articles on the accuracy of LBC-based diagnosis of IM.Results Heterogeneity analysis was performed in four articles including 285 patients with 854 lesions met the inclusion criteria,and there was no significant heterogeneity among three studies,including 247 patients with 626 lesions.The pooled sensitivity,specificity and SROC were 0.895(95%CI:0.861-0.923),0.900(95%CI:0.862~0.931)and 0.957 in the diagnosis of IM.Conclusion LBC observation NBI-ME combined with narrow band imaging has higher pooled sensitivity and specificity in the diagnosis of gastric IM,but more studies should be performed to access the diagnostic value of LBCfor detecting intestinal metaplasia in Barrett's esophagus.
Narrow band imaging Magnification endoscopic Light blue crestIntestinal metaplasia

2013-09-05)
(本文编辑:沈昱平)
310014 杭州,浙江省人民医院消化内科
黄伟,E-mail:hw771119@163.com
猜你喜欢
临床肝胆病杂志(2022年8期)2022-11-23
中国临床医学影像杂志(2022年6期)2022-07-26
社会科学战线(2022年5期)2022-07-23
中华骨与关节外科杂志(2021年8期)2021-11-30
现代企业(2021年2期)2021-07-20
西安邮电大学学报(2021年6期)2021-05-10
中国现代药物应用(2018年14期)2018-08-27
家庭用药(2018年11期)2018-01-23
医学研究杂志(2015年9期)2015-07-01
眼科新进展(2012年6期)2012-05-19