
A review of the epidemic and clinical study on scrub typhus in China(2010-2020)
2024-01-08 10:24XIEXiaofeiWANGGaoyuHUANGYiTANGChuanningPENGRuoyanHUXiaoyuanDUJiangQINAipingYINFeifei
Journal of Hainan Medical College 2023年19期
XIE Xiao-fei, WANG Gao-yu, HUANG Yi, TANG Chuan-ning, PENG Ruo-yan,HU Xiao-yuan, DU Jiang, QIN Ai-ping, YIN Fei-fei,3✉
1.Key Laboratory of the Ministry of Tropical Medicine, Hainan Medical College, Haikou 571199, China
2.Hainan Medical College Joint Laboratory of Tropical Infectious Diseases at the University of Hong Kong, Haikou 571199, China
3.Public Health and One Health International College of Hainan Medical College, Haikou 571199, China
4.National Institute for Infectious Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 102206, China
Keywords:
ABSTRACT Scrub typhus is an acute febrile vector-borne zoonotic disease caused by the obligate intracellular growth bacterium Orientia tsutsugamushi (Ot).Mites are the primary vectors and rodents play a pivotal role in the transmission of scrub typhus.Due to the climate warming,increased human activity and other factors, cases of scrub typhus have been increased sharply during the past decade in China, especially in the northern China.To understand the incidence trend, epidemic pattern, clinical sign, diagnosis and therapy of this diseases as well as genotype evolution of Orientia tsutsugamushi, we summarized and analyzed the current knowledge of scrub typhus in China from 2010 to 2020.The data indicated that the dominate genotypes of scrub typhus in China were Karp, Kato and Gilliam.Although the disease was distributed national wide, Yunnan, Guangzhou and Fujian showed the highest incidence rate.The main vector of scrub typhus in southwest, middle east and southeast of China appeared a geographic preference respectively.Seasonal timing, age and occupation were the key factors that relate to the peak incidence of scrub typhus.Notably, farmer was the occupation with the highest risk of Ot infection.Further study on the epidemic characteristics, risk factors, diagnosis and treatments of scrub typhus will be of benefit to a comprehensive guideline for prevention and control of this ancient disease.
1.Introduction
Scrub typhus, whose pathogen is Orientia tsutsugamushi (Ot), is an acute infectious disease mainly caused by the bite of chigphus mites.Scrub typhus first belonged to the genus Rickettsia of Rickettsiaceae,but it is very different from the other Rickettsia species,so it has another genus, called scrub typhus[1].Nonspecific clinical manifestations such as fever, rash and ulcers often occur in the early stage of scrub typhus, A proportion of the patients had eschars.It is difficult to distinguish from other diseases, so the misdiagnosis rate and missed diagnosis rate is high.Improper treatment can aggravate the condition, such as damage to the liver,kidney and other organs, which can lead to death[2].Mortality in scrub typhus increased with age and was 14.3% ~ 70% in patients undiagnosed[3].The cure rate of this disease is related to the course of the disease, The study showed cure rates of 100%, 88% and 71%for patients whose course within one week, two weeks and over two weeks, respectively[4].
The traditional scrub typhus epidemic area is mainly located in the“scrub typhus triangle”, ranging from eastern Russia to Pakistan,Afghanistan, Australia, and also including the island states near the southwest pacific and indian ocean islands.In recent years, the range of infections has been wide in areas outside this triangle,such as the isolation of O.chuto strain in the United Arab Emirates,seropositive patients in Chile, and reports of scrub typhus in some African countries[5](figure 1).Tscrub typhus is mainly prevalent in tropical and subtropical areas in China,Yunnan, Fujian, Guangdong and other provinces are the high incidence area of scrub typhus in China.In recent years, the epidemic area of scrub typhus in China has been expanding from south to north, and the seasonal difference between the north and the south is obvious[6].
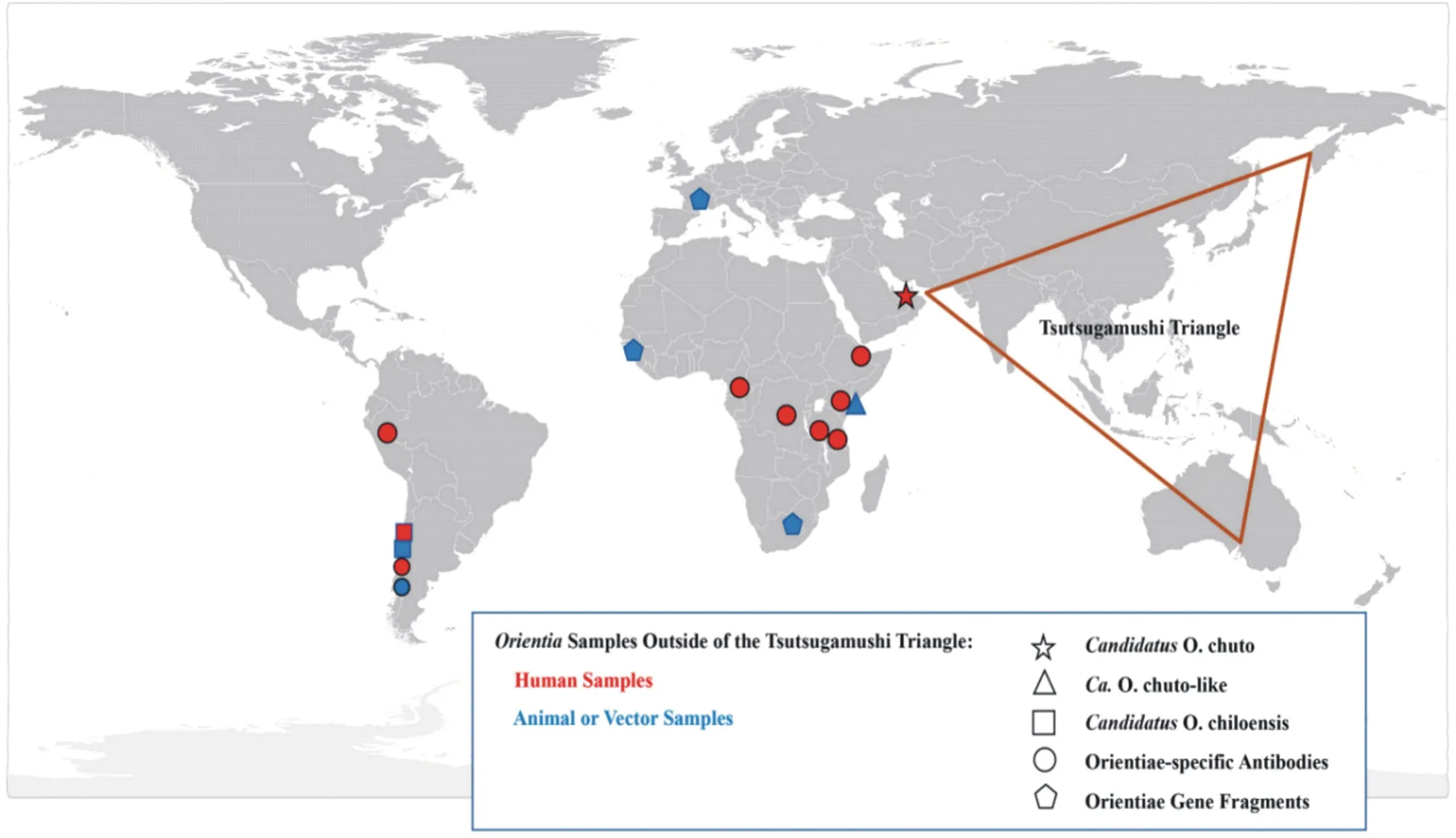
Fig 1 Geographic distribution of scrub typhus worldwide[7]
To understand the incidence trend, epidemic pattern, clinical sign,diagnosis and therapy of this diseases as well as genotype evolution of scrub typhus, we summarized and analyzed the current knowledge of scrub typhus in China from 2010 to 2020.
2.History of Orientia tsutsugamushi
The prevalence of scrub typhus has been reported in many countries, the emergence of cases during the 1951 Korean War brought to awareness of the disease; during the Vietnam War in the 1960s, screening febrile patients among American soldiers and support crew identified the patients[8].Japan had erupted from 1976 to 1984, when it was also called the Japanese River fever[9].Since the 1980s, the incidence of scrub typhus has expanded and the incidence increased, its involved areas have gradually expanded to non-infectious disease epidemic areas such as the Middle East,Africa and South America[8].On a global scale, about a billion people located in the scrub typhus triangle are estimated to be at risk for the disease[10].
China is the first country to record scrub typhus.In 313 AD, Ge Hong of the Jin Dynasty’s “Prescriptions for emergent reference”called it “sand lice poison”[8].In 1943, the presence of scrub typhus was confirmed in Wei Xi et al.In 1948, scrub typhus was first isolated in the blood by Peng et al[11].Before 1986, scrub typhus was mostly prevalent in southern Chinese provinces, such as Hainan, Guangzhou, Taiwan, Zhejiang, Hubei and so on.However,since the 1990s, the disease has often been prevalent in northern provinces, such as Jiangsu, Henan, Tianjin and other regions[12].China has stopped the legal testing of scrub typhus since 1990, but due to the expanding of the disease and the increasing number of infections, China once again included it in the national legal disease surveillance system in 2006.Recent years, with the influence of economic development, climate change and the flow of population,the epidemic of scrub typhus has appeared in various provinces[13].
3.Progress in the national epidemiological investigation of Orientia tsutsugamushi from 2010 to 2020
3.1 Time distribution characteristic
The Chinese Center for Disease Control and Prevention counted the distribution of scrub typhus cases in different months in the 12 provinces in China from 2006 to 2018, and concluded that the transmission of scrub typhus had obvious seasonality, increasing rapidly from May, reaching a peak from June to August, and decreasing from September to December.South of the boundary is mainly the summer type, with the onset of peak in May-November,consistent with the active period of vector chigmites.North of the boundary line is mainly the autumn and winter type, with onset of peak in October and November[5], coincides with the autumn harvest.New research has found that these types may occur in the same province or region[13].
3.2 Spatial distribution characteristic
Scrub typhus has been reported in Chinese provinces except Qinghai.Currently the disease has spread from the south, southwest,southeast, and eastern coasts of China to the central, northern,northeast, and northwest regions of Chinese mainland[14].The representative areas of scrub typhus disease in China are as follows.Autumn and winter type has Shandong, Jiangsu, Anhui, Beijing and Tianjin border area, Some areas in southern Anhui province and central Jiangxi Province belong to the transitional zone[15].
Small-scale epidemics of scrub typhus have occurred in many parts of China, such as Nanjing City, Jiangsu province, Fuyang City,Anhui Province, Mengyin City, Shandong Province, Baodi District,Tianjin, etc[16].The high incidence region of scrub typhus can be divided into three sub-regions: the northern region are Shandong,Anhui and Jiangsu.The southwest region are Yunnan and Sichuan provinces.The southern regions are Hainan, Guangxi, Guangdong,Fujian, Hunan, Jiangxi and Zhejiang[17].
3.3 Host and media
The spread of scrub typhus depends on vector and natural hosts,Its prevalence trend is closely related to the host distribution and seasonal change.Chigger mites are vectors of Orientia tsutyphus infecting humans, and rodents are intermediate hosts.
The confirmed media mites in China are Leptotrombidium deliense,L.scutellare, L.rubellum,L.kaohuense,L.insulare and L.jishoum.Chigger mites mainly grow in places and different regions have different types.Leptotrombidium deliense are mainly distributed in the south of the Changjiang River, its the main mite species in the summer epidemic area; L.scutellare are widely distributed in China , its the major mite species north of the Yangtze river[13].
Rattus losea, Apodemus agrarius and Tscherskia triton are the hosts of mites, and insectivores, such as shrews, can also serve as hosts;some birds, cats and rabbits may also be infected[9].
New natural and social factors can affect the activities of hosts and media, such as the reduction of industrial land, vegetation restoration, and the prohibition of straw burning that have provided a favorable environment for the reproduction of rodents and mites in recent years, forming a new natural epidemic areas[17].
3.4 Vulnerable populations
The age of onset in each region is mainly mainly 41~70, among which the elderly are more likely to get sick.Farmers are the most vulnerable occupation.Working longer hours in the field, lack of protective clothes and less washing of clothes and skin were all risks factors of scrub typhus[18].Moreover, socioeconomic factors have been identified as one of the risk factors for scrub typhus, such as occupational factors, education level, etc[19].Unexpectedly, children under 10 years old were at increased risk of disease in recent years ,especially in southern provinces.Implicating children as a neglected group, for whom the education and preventive measures need to be intensified[20].
4.Genotype and pathogenesis of Orientia tsutsugamushi
The 56-kDa specific protein is the main outer membrane protein of Orientia tsutsugamushi and the specific antigen determination cluster of this protein is the basis of strain typing and immunological characteristics of scrub typhus.At present,The most common genotype among the more than 40 genotypes identified globally is Karp, followed by Gilliam, and other types such as Kato, Kawasaki,Kuroki, Shimokoshi, etc[21].
The main popular de genotypes in China are Karp, Kato, Gilliam,which have some regional differences in China.Gilliam, Karp and Kawasaki types are popular south of the Changjiang River.For example, Yunnan province is mostly Karp and Gilliam.Kawasakit are popular north of the Changjiang River, including Karp and Gilliam, such as parts of the Xinjiang[22].
Orientia tsugamushi infects people through chigger bites, and its cross-immune response is weak, so patients tend to relapse due to infection with different serotypes of Ot.The incubation period of Ot infection is 5 days to 2 weeks, and its able to infect many types of cells, such as macrophages, monocytes, dendritic cells.Dendritic cells and macrophages in the dermis are the target cells during infection, They can transmit the pathogens to the lymph nodes,allowing the T lymphocytes to attack the infected host cells and thus disease occurs[23].
5.Laboratory testing methods for Orientia tsugamushi
Orientia tsugamushi is an obligate intracellular parasitic bacterium,so it is difficult to isolate and cultivate , and serological testing is the main method to diagnose.The IgM antibodies produced after infection reached detectable levels within the first week, and the IgG antibodies appeared at two weeks after the first infection and within one week of re-infection; ELISA is easy to operate, has high sensitivity and specificity, but has high cost, and is susceptible to temperature and time; Weil-Felix test is an earlier and less costly auxiliary diagnostic test, but with poor sensitivity and specificity,Other assays include immunoenzyme staining and complement binding assay[24].
Recently, the wide application of molecular biology technology in the diagnosis of this disease has improved the detection sensitivity and specificity.In the first few days of fever, serological tests are often negative, and the Nested PCR can be applied.This method designs specific primers , but if patients use appropriate antibiotics,PCR often has negative results, and eschar tissue samples can be used as a template for PCR[25].Recombinant polymerase amplification completed DNA amplification for 20 min at 37 ℃, and then observed by immunochromatography strip, with low facility requirments and ligh sensitivity and specificity[27]; Loopmediated isothermal amplification can be used for the acute phase of scrub typhus, with high amplification efficiency and low cost[27].Metagenomics next generation sequencing, mNGS has the advantages of fast and accurate, and can be applied when patients lack specific clinical manifestations[28].Advances and application of molecular technology will detect and confirm more patients, so to some extent the increased number of scrub typhus infections is due to the discovery of new patients using more sensitive and reliable tests, so the molecular biology methods will be an important research direction for the future detection of pathogens[29].
6.Clinical manifestations of patients
Totoxins released by Ot damage a variety of organs, such as the skin, lungs, heart, liver, kidney, blood and the central nervous system[30], Therefore, the clinical presentation of scrub typhus is complicated and requires joint diagnosis by combining clinical characteristics with test results.Some special skin lesions (eschar and ulcers) are common in perineal, groin and other parts, which can be used as the evidence for diagnosis and treatment.However,the clinical manifestations such as fever and enlarged lymph nodes are similar to many diseases, such as influenza, malaria, dengue fever, and these diseases are often co-infected with scrub typhus[31].The best time for patients to visit is within 2 weeks of onset, rest and drink water to maintain the Water-electrolyte balance.Patients with high fever can use antipyretic analgesics; with skin lesions can be applied chloramphenicol, erythromycin.Anti-infective therapy should be using lipid-soluble antibiotics that can pass through the cell membranes, such as tetracyclines, quinolones, macrolides.Aminoglycosides, cephalosporins and penicillin are not effective[32].
7.Summary and prospect of scrub typhus
Scrub typhus is a natural focus infection disease with a worldwide epidemic and expanding scope.Despite its low mortality rate, it imposes a heavy burden on social public health.
Studies show that environmental factors such as rainfall, climate,and vegetation cover affect the prevalence trend and extent of scrub typhus by affecting the activities of the host and the vectors[9].Compared with the important insect-borne infectious diseases such as Aden fever and hemorrhagic fever in renal syndrome, most of the research about influencing factors of scrub typhus stays on the environment, while the research on the future epidemic trend prediction and its association with social and economic development is still lacking.In recent years, the number and scope of scrub typhus cases in China have increased, but the cause is still unknown.Therefore, it is very necessary to study the epidemic, influencing factors and regional distribution of scrub typhus, which can provide scientific basis and guidance for the prevention and control of scrub typhus in China.
 Journal of Hainan Medical College2023年19期
Journal of Hainan Medical College2023年19期
- Journal of Hainan Medical College的其它文章
- Study on the in vitro anti ovarian cancer effect and mechanism of quinazoline derivative (N111)
- m6A modification promotes the proliferation and migration of cervical cancer and regulates the expression of PD-L1
- Expression and correlation of pyroptosis-related markers and PI3K/AKT pathway in endometriosis
- Meta-analysis of the efficacy of volar plate internal fixation versus closed reduction and external fixation in the treatment of adult distal radius fractures
- MiR-15a-5p in neutrophil exosomes promotes macrophage apoptosis through targeted inhibition of BCL2L2
- Clinical efficacy of bushen huatan huoxue recipe in combination with acupuncture in treating patients suffering from polycystic ovary syndrome with insulin resistance