
The Status and Associated Factors of Successful Aging among Older Adults Residing in Longevity Areas in China*
2016-08-15 03:24SHIWenHuiZHANGHongYanZHANGJuanLYUYueBinMelanieSerenyBrasherYINZhaoXueLUOJieSiHUDongShengFENLeiandSHIXiaoMingDivisionofNCDControlandCommunityHealthChineseCenterforDiseaseControlandPreventionBeijing006ChinaDepar
SHI Wen Hui, ZHANG Hong Yan, ZHANG Juan, LYU Yue Bin, Melanie Sereny Brasher,YIN Zhao Xue, LUO Jie Si, HU Dong Sheng, FEN Lei, and SHI Xiao Ming. Division of NCD Control and Community Health, Chinese Center for Disease Control and Prevention, Beijing 006, China; . Department of Epidemiology and Health Statistics, College of Public Health, Zhengzhou University, Zhengzhou 000, Henan, China; . Department of Sociology and Anthropology, Department of Human Development and Family Studies, University of Rhode Island, Kingston, RI088, USA; . Department of Preventive Medicine Shenzhen University School of Medicine, Shenzhen, Guangdong 8060, Guangzhou, China;. Department of Psychological Medicine, Yong Loo Lin School of Medicine, National University of Singapore 9077, Singapore; 6. Institute of Environment Health and Related Product Safety, Chinese Center for Disease Control and Prevention, Beijing 0000, China
Original Article
The Status and Associated Factors of Successful Aging among Older Adults Residing in Longevity Areas in China*
SHI Wen Hui1, ZHANG Hong Yan2, ZHANG Juan1, LYU Yue Bin1, Melanie Sereny Brasher3,YIN Zhao Xue1, LUO Jie Si1, HU Dong Sheng4, FEN Lei5, and SHI Xiao Ming6,#
1. Division of NCD Control and Community Health, Chinese Center for Disease Control and Prevention, Beijing 102206, China; 2. Department of Epidemiology and Health Statistics, College of Public Health, Zhengzhou University, Zhengzhou 450001, Henan, China; 3. Department of Sociology and Anthropology, Department of Human Development and Family Studies, University of Rhode Island, Kingston, RI02881, USA; 4. Department of Preventive Medicine Shenzhen University School of Medicine, Shenzhen, Guangdong 518060, Guangzhou, China;5. Department of Psychological Medicine, Yong Loo Lin School of Medicine, National University of Singapore 119077, Singapore; 6. Institute of Environment Health and Related Product Safety, Chinese Center for Disease Control and Prevention, Beijing 100020, China
Abstract
Objective This study aims to assess the status of successful aging (SA) in longevity areas in China and explore multiple factors associated with SA among the young-old and oldest-old.
Methods A total of 2296 elderly people aged 65 and older were interviewed in the longevity areas sub-sample of the Chinese Longitudinal Healthy Longevity Survey (CLHLS) in 2012. Baseline assessments included a researcher-administered questionnaire, physical examination, and laboratory testing. A logistic regression model was used to identify factors associated with SA.
Results The prevalence of SA was 38.81% in the CLHLS in 2012. There were significant differences between ages groups, with SA compromising 56.85% among ≥65 years group and 20.31% among ≥100 years group=126.73, P<0.01). The prevalence of SA among females was 33.59%, which was significantly lower than that among males (45.58%)=33.65, P<0.05). In the regression analysis, having anemia (OR=0.744, 95% CI: 0.609-0.910), poor lifestyle (OR=0.697, 95% CI: 0.568-0.854), poor sleep quality (OR=0.558, 95% CI: 0.456-0.682), and central obesity (OR=0.684, 95% CI: 0.556-0.841) were the main factors associated with SA. The promoting SA rate decreased as age increased, and the group of 65-79 years had higher odds than the other age group.
Conclusion Preventing central obesity, improving sleep quality and promoting healthy lifestyle may contribute to achieve SA among the elderly.
Successful aging; Older adults; Evaluation; Associated factors
www.besjournal.com (full text) CN: 11-2816/Q Copyright ©2016 by China CDC
INTRODUCTION
Since the 1980s, China has begun the process of population aging, and by 2030 15.7% of the total population will be elderly. Each person is now facing the menace of aging and related concerns and questions. Scholars and individuals have long been interested in successful aging (SA) what is the ideal physical,mental and social well-being state for older adults and how to achieve this? The concept of SA, as an objective measurable condition at a certain point in time, was proposed by the World Health Organization (WHO) in the 1960s, demonstrating the positive extreme of normal aging, mainly referring to freedom from chronic diseases and the ability to sustain effective physical and mental function in old age[1]. Despite abundant studies of SA, the scientific community has yet to agree on a consensus definition[2]and operational definitions of SA are inconsistent[3]. In the meantime, the oldest-old (individuals over age 80) are a rapidly growing age group that is heterogeneous in terms of health and functioning: they have some health problems but many are independent in basic every day activities and meet the key biomedical criterion of SA. Are they aging successfully or not? Young et al.[4]suggested that SA may coexist with diseases and functional limitations if compensatory psychological and social mechanisms are utilized. Models which emphasize the absence of disease and activity as criteria for SA may be not the most relevant for and applicable to the oldest-old[5]. Models should place greater emphasis on autonomy, adaptation and sense of purpose.
China is currently facing challenges, such as a lack of specialist physicians and systems in place to care for the elderly, which will aggravate the negative effects of anaging population. To offset such negative effects, it is imperative to tackle the issue from different perspectives. With increasing life expectancy, the number of nonagenarians and centenarians has dramatically increased. Since 1982,the Chinese Medical Association on Gerontology Branch has formulated relevant content and dimensions of the Health Chinese Elderly and relative policies and programs on aging, yet ideas about advocating and promoting successful aging are limited. The increases in life expectancy make it important to remain healthy for as long as possible[6]. The longevity phenomena has been studied extensively with a focus on various factors, including nutrition and health status, such as the oldest-old having lower risk of chronic disease[7]. Other research has found that anemia was a serious problem[8]leading to a higher risk of mortality[9]. Few studies, however, have focused on the relationship between SA and the longevity-phenomena in China. Contrary to common opinion[10], some researchers thought SA was more critical than simply longevity. It is important to identify the specific factors that can promote longevity and SA at the individual level. In this study, survey data in longevity areas from the 2012 wave of the Chinese Longitudinal Healthy Longevity Survey (CLHLS) were utilized to examine factors associated with SA among the elderly.
METHODS
Subjects and Design
Data was collected in the Chinese Longitudinal health Longevity Survey (CLHLS) in 2012. The study design of CLHLS has been reported in elsewhere[7,11-12]. The baseline survey of this current study was conducted in seven longevity areas of China in 2009, including Laizhou City in Shandong province, Xiayi County in Henan province,Zhongxiang City in Hubei province, Mayang County in Hunan province, Yongfu County in Guangxi province, Sanshui District in Guangdong province,and Chengmai County in Hainan province. A total of 2036 people aged 65 or older participated in the baseline survey. The follow-up survey was undertaken in the same seven longevity areas in August in 2012 and Rudong County in Jiangsu province was added. The survey included all centenarians in such areas and randomly paired with three persons at the age of 90-99 years-old, 80-89 years-old, and 65-79 years-old residing in the area. In 2012, 2352 subjects over 65 years old were surveyed,and 56 subjects were excluded because of missing data on key variables including cognitive function,and blood or urine samples. Finally, 2296 subjects were selected for this analysis. The study was endorsed by the Ethics Committee of Peking University and the Ethics Committee of the National University of Singapore. Written inform consent was received from all participants and/or their relatives.
Data Collection
The study included two components: an in-house face-to-face interview and physical examination. The interview was conducted by atrained physicians or public health workers from the regional Centers for Disease Control and Prevention and community hospitals. All the responses to questions should be provided by the participants themselves. For those respondents who were unable to complete the interviews, responses came from family members. The questionnaire elicited information related to demographics, behaviors and lifestyle parameters, self-rated health status and self-reported chronic diseases, cognitive function,and the performance of activities of daily living (ADL). The physical examination was carried out by experienced clinicians using standardized instruments to measure height, weight, waist circumference (WC), systolic blood pressure (SBP),and diastolic blood pressure (DBP). WC was measured to the nearest 0.1 cm by using a non-elastic plastic tape at the level of the midpoint of the waist between the lower rib margin and the iliac crest. SBP and DBP were calculated based on two measurements with a mercury sphygmomanometer.
Biochemical Analyses
Participants were required to fast overnight. Five milliliters of venous blood and urine were collected in the morning. Venous blood samples were collected in heparin anticoagulant vacuum tubes, and then centrifuged at 20 °C, 2500 rpm for 10 min. Plasma was isolated and frozen in -20 °C,and then samples were shipped on wet ice to the central laboratory of Beijing Capital Medical University in Beijing, where they were stored at -80 °C until analysis. Serum creatinine concentration was determined with the picric acid method and albumin urine concentration was measured by dry chemistry reagent test strips (Siemens Diagnostics,NY, USA). Fasting plasma glucose, hemoglobin,low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) were measured by an automatic biochemistry analyzer (Hitachi 7180, Japan) using commercially available diagnostic kits (Roche Diagnostic, Mannheim,Germany) at the Beijing Capital Medical University in Beijing. Urine samples were tested for microfilming and creatinine using Siemens Microalbustix (Siemen Healthcare Diagnostic, USA).
Key Variables and Definitions
Hypertension was defined as SBP≥140 and/or DBP≥90 mmHg, or being on anti-hypertensive therapy or having previously diagnosed hypertension. Diabetes was defined as a fasting plasma glucose (FBG) ≥7.0 mmol/L or previously diagnosed on Type 2 diabetes or taking anti-diabetes medicine. Dyslipidemia was defined as the concentration of total cholesterol (TC) ≥6.22 mmol/L, Triglycerides (TG) ≥2.26 mmol/L or high-density lipoprotein cholesterol (HDL-C) <1.04 mmol/L. Central obesity was defined as WC ≥85 cm for males or WC ≥80 cm for females. Body mass index (BMI) was defined as weight (kg)/height2(m). A healthy weight is considered to be a BMI less than 24. A BMI of 24 to 27.9 is considered overweight. A BMI of 28 and above is considered obese. Anemia was defined as hemoglobin<130 g/L for males or hemoglobin <120 g/L for females. Chronic kidney disease (CKD) was assessed from the estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2and/or albuminuria. The eGFR was calculated with the modification of diet in renal disease (MDRD)equations for China: eGFR=175×(creatinine)-1.234× age-0.179×1 (if male) or ×0.79 (if female).
Education was classified as ‘yes' if the subject reported at least one year of any formal schooling or ‘no' if reported less than one year. Sleep quality was considered to be ‘good' by self-reported ‘very good or good', others as ‘not good'. The duration of sleep was moderate if the reported sleeping hours were 6-9 h, others as not moderate.
The measurement of lifestyle[13]included the following items and each item contributes one point:(1) no smoking currently; (2) no drinking currently, or drinking a volume ≤100 mL alcohol/day for males,≤50 mL alcohol/day for females; (3) daily exercise; (4)eating fresh fruits every day; (5) eating fresh vegetables every day; (6) having meat 1-6 times each week; (7) eating fish at least once a week; (8)drinking milk or dairy products every day. Subjects whose total score was higher than 4[13], are considered to have a good lifestyle.
SA definition in the study was defined by having a score (based on the following items) of more than 3 points, otherwise the respondent is considered non-successful aging (NON-SA). Points come from the following five items and each item is worth one point[13]. (1) self-rated health is scored 1 if subjects rated their health as good or excellent; (2) good self-related psychological status or mood as good is scored 1; (3) normal cognitive function is scored 1. Cognitive function was assessed by the Mini-Mental State Examination (MMSE)[14], which has been widely applied in epidemiological studies. This assessment tool involves five domains including orientation,registration, attention, memory, language and visual construction skills. The scores ranged from 0 to 30 points. Subjects with an MMSE score less than 24 are considered to have cognitive impairment while subjects with an MMSE score higher than 24 are considered normal; (4) activities of daily life (ADL) is scored 1, if a subject's ADL is defined as normal. Disability was assessed based on self-reported performance of the following six self-care tasks:dressing, eating, toileting, bathing, indoor activities,and continence[15]. ADL was defined as normal if an individual could carry out all six tasks independently;otherwise ADL was defined as restricted; (5) normal physical activity is scored 1, if a subject is able to regularly walk or exercise continuously for 1 km, lift a 5 kg weight, or being able to squat three consecutive times.
Statistical Methods
The questionnaires were inputted in Epidata 3.0 software using the double-entry method. All the data were statistically analyzed using SPSS 20.0 software. A Chi-square test was used to compare the differences in the basic situation of SA and non-SA. A logistic regression model was carried out to explore the relationship between SA and related factors. A backward stepwise elimination was used in the logistic regression. Results of logistic regression analysis are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Two-sided P values (P<0.05) are considered statistically significant. Table 1. Descriptive Statistics by SA Group for Chinese Longevity Areas Sample
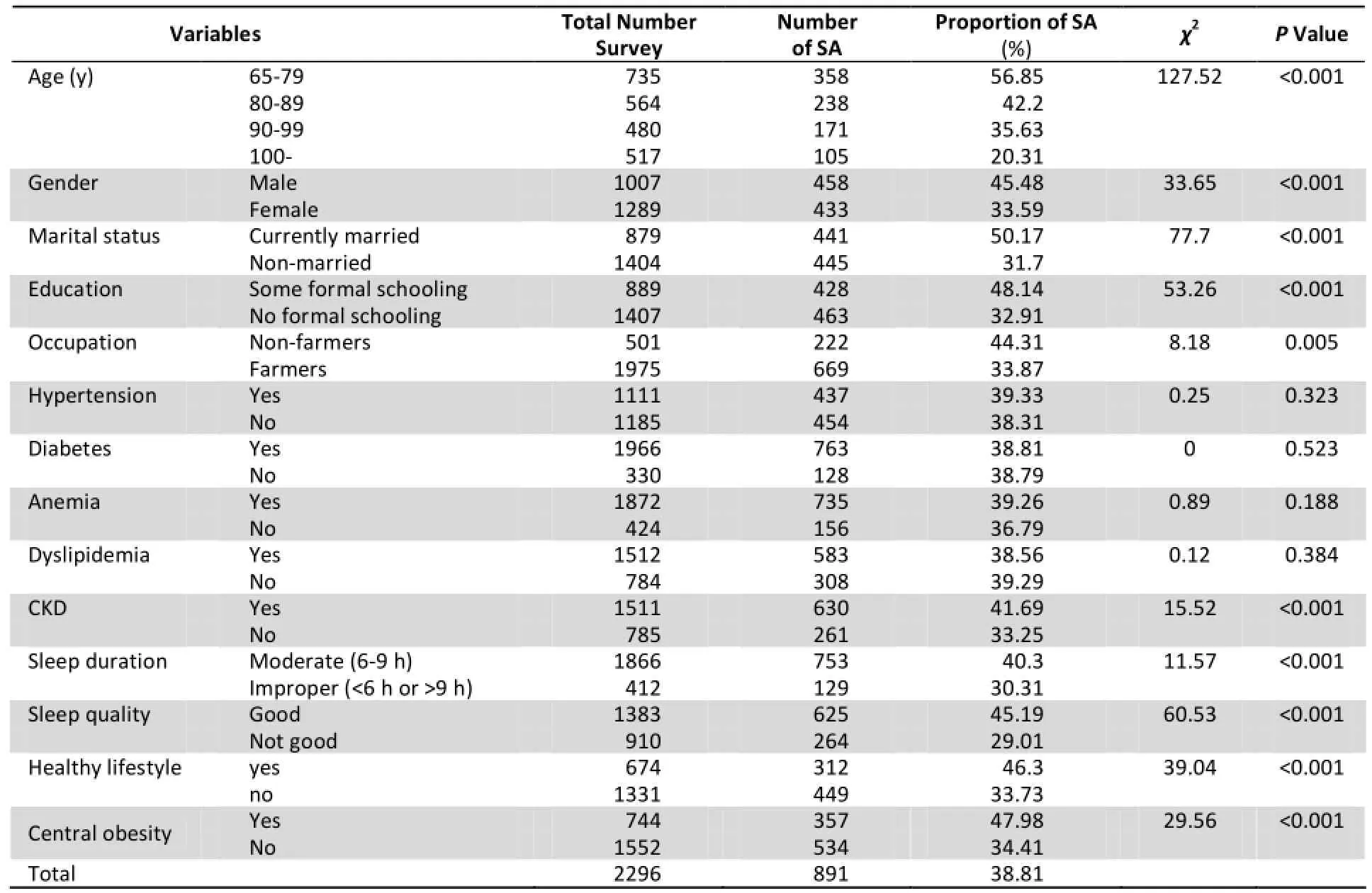
Note. SA, successful aging; CKD, chronic kidney disease; GP, general practice; WC, waist circumference;Missing data for marital status (13); education and sleep quality (3); sleep duration (18) and GP (291).
RESULTS
Characteristics and Prevalence of SA
In this study, a total of 2296 elderly people were included and 38.81% (891) demonstrate SA, 45.48% (458) among males and 33.59% (433) among females,and this difference in SA is statistically significant=33.65, P<0.01). As shown in Table 1, by age group, there are statistically significant differences in SA=127.52, P<0.05), with each older age group exhibiting a smaller proportion of SA=124.08,P<0.05).
The proportion of SA is lower among currently unmarried respondents (31.70%, 445/1404), versus currently married respondents (50.17%, 441/879)=77.70, P<0.05). Significant differences were also found for different categories of education and occupation=53.26, P<0.001=8.18,P<0.005). The association between chronic conditions and SA varied by condition. There were no significant differences in the proportion of SA among groups with or without hypertension,diabetes, dyslipidemia and anemia=0.25,=0.00=0.89=0.12, P>0.05). While in the groups suffering from CKD, improper sleep duration, poor sleep quality, lifestyle score less than 4, central obesity, there were significant differences in the proportion of SA by categories of the variable.
Factors Associated with SA
In our study, factors including age, gender, marital status, education, occupation, lifestyle, sleep quality, sleep duration, and health conditions including hypertension, diabetes, dyslipidemia,chronic kidney disease, and anemia were candidate variables in the logistic regression with backward elimination as factors possibly associated with SA. Only age, marriage, having anemia, healthy lifestyle, sleep quality and central obesity were kept in the final logistic regression model and was responsible for explaining 67.4% of the total variation. Compared to the more than 100 years old age group, those aged 65-79 were more likely to exhibit SA, and the OR value varied from 2.784 in the 65-79 years old age group to 2.163 in the 90-100 years old age group as age increased. Married respondents were more likely to achieve SA than the unmarried. The index of poor quality of sleep, unhealthy lifestyle, central obesity and suffering anemia reduce the odds of achieving SA.
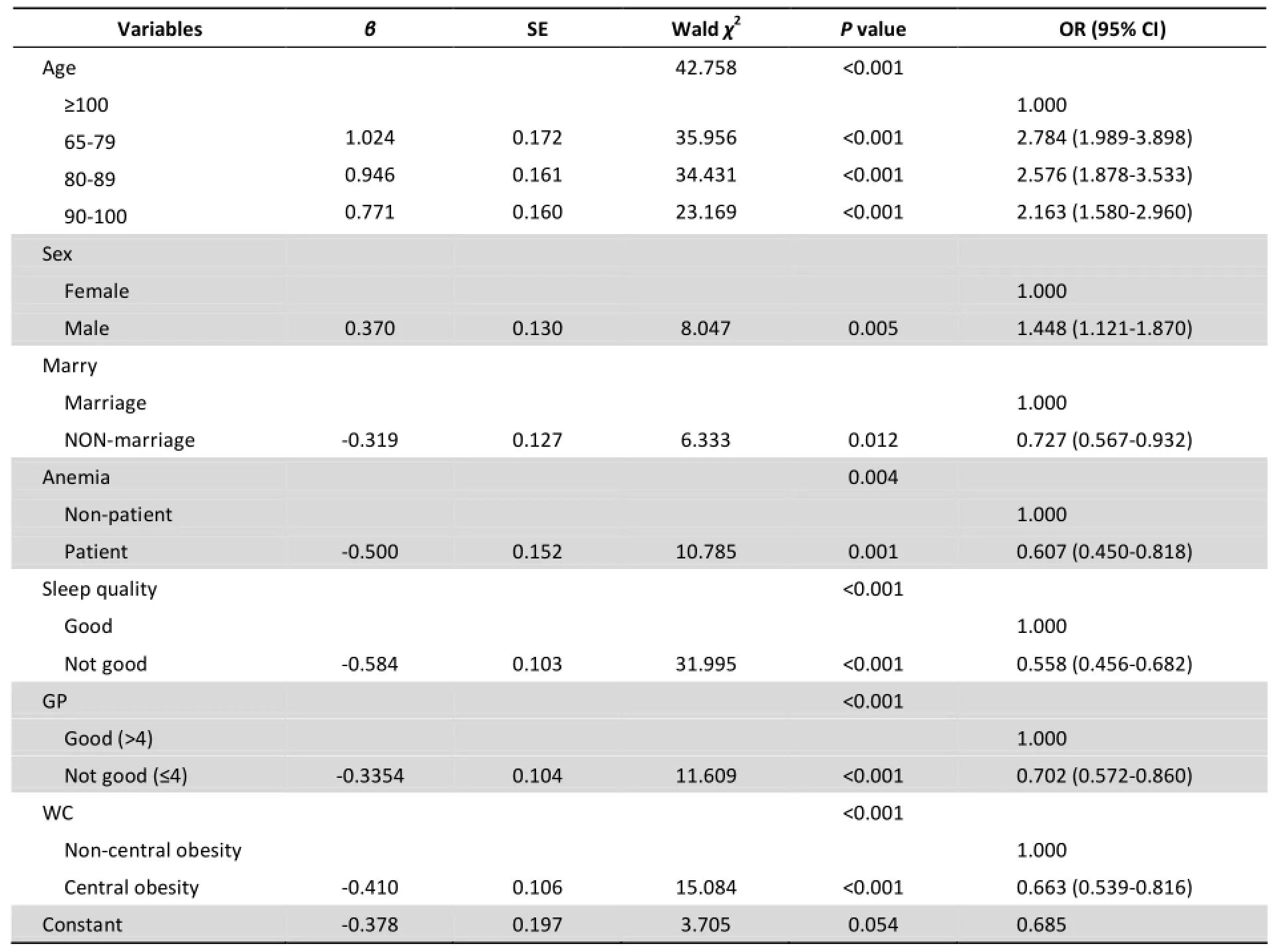
Table 2. Multivariable Logistic Analysis of Associated Factors of SA in Longevity Areas of China
DISCUSSION
The Characteristics of Operational Definitions of SA in the Study
Older adults face unavoidable physical decline,such as organ aging, functional impairment, and a variety of chronic diseases. Self-rated health status has been regarded as a better indicator to reflect the health state of the elderly than objective indicators such as mortality, etc.[16-17], making reliable results more effectively compared among different populations. This study collected self-assessed data to define SA.
According to the definition of health by WHO,evaluation of SA should be based on three components: physical, psychological, and sociological. The most influential model of SA was Rowe-Kahn's three-dimensional model[18-19], key aspects of which are low probability of disease and disease-related disability, high cognitive and physical functional capacity, and active engagement with life. In our survey, health was measured by self-rated health status, cognition was measured by MMSE score, and physical function was measured by ADL disability status. While our study is similar to a previous study in urban China[20], there are also some key differences. The previous study was conducted in an urban community in Shanghai,which is very different from the mostly rural longevity areas that we studied. In addition, their measure of SA and ADL disability was very strict-ADL evaluation consisted of 14 items and an old participant should be without injury or disability at the survey time, which was too strict to evaluate the health status of the old. This would discourage the elderly to improve their health at individual level. In previous study[15], ADL was assessed by using six items involving only indoor activity, and excluding outdoor physical activity. This study includes both indoor and outdoor activities to evaluate the state of physical independence and functioning of the elderly[21]. While subjective well-being was another indicator[13]used to assess recent mental health, it was not suitable for evaluating depression. Depression is a major psychological problem among older adults in China and is associated with an increased risk of dementia and Alzheimer's disease (AD) in older males and females[22], possibly emerging as a consequence of subjectively perceived worrisome cognitive deterioration[23], and depression also was one of the diseases needed to be managed in the elderly[24]. So preliminary screening on depression was taken to show the mental state. To sum up, based on the Rowe-Kahn's model, self-rated health status, current state of mind,emotional self-evaluation, cognitive ability, daily life/physical ability, and age were supported by our study to assess SA. Our data showed the common chronic conditions (such as hypertension, diabetes,dyslipidemia, CKD) were not significantly associated with SA, which confirms a previous study[25]. The prevalence of successful aging among previous community-based studies ranges from 0.4% to 95.0% based on various definitions[26-27]. The rate of SA in CLHLS carried out in 2012 in eight regions was 38.81%, which was similar to the SA prevalence of 35.3% among Canadian seniors aged 65 years old[28].
Correlates of SA
The relationship between age and SA has been widely documented: a significantly higher proportion of younger individuals achieve SA versus older individuals. Research showed that for each additional 5 years of age, the probability of SA would be lowered by 64%[29]. While another study showed that longevity was the third element of SA[30]. However, the present study revealed that after controlling for factors potentially affecting SA,compared to the age group 100- years, the elderly from younger age group (65-year-old to 99-year-old)are more likely to have successful aging. The trends decline with increasing age. The average life expectancy was 74-years-old in China in 2015. With population aging, Chinese people are living much longer lives and increasingly, individuals have the potential to live even longer and achieve SA. According to Tengku et al, SA is more likely to be among younger age groups of the elderly[31], special attention should be paid to 65-79 years old people,who have more opportunity to achieve and benefit more from SA than others.
Successful aging was more prevalent among males[5], because they had more social resources,higher income relatively[32]. In addition, men tend to live fewer years than women. Our study finds this same gender difference, with men having an advantage in SA. There were more elderly women (56.1%) in the CLHLS sample and they lived longer,but major common female diseases incidence about hypertension was 56.1% (705/1289), anemia was 64.15% (791/1289), kidney disease was 41.04% (529/1289) separately, which was higher than male hypertension rate 47.67% (480/1007), anemia rate 32.27% (325/1007), kidney disease rate 25.42%(256/1007), with statistically significant differences by gender, and χ2was 11.179, 34.205, 61.284 respectively and the male had better health status than female. The same conclusion was drawn from the China Health and Retirement Longitudinal Survey ‘Chinese men's health is still significantly better than female's'[33]. Maybe the gender difference about SA was mainly caused by health status difference, not by the social resources and higher income.
Sleep problems are common among elderly people[34-35]. The rate of poor sleep quality in our survey was 39.63% (910/2296), lower than the epidemiologic studies which showed approximately 50% of older adults had sleep problems[36]. Prior research shows a positive correlation between Pittsburgh Sleep Quality Index (PSQI) scores and Beck Depression Inventory (BDI) scores and a significantly positive correlation between life quality and depression[37]. Shorter sleep duration in both males and females were significantly associated with higher BMI and WC measures (P<0.05)[38]. Mental and physical illness can reduce the quality of sleep,resulting in sleep disorders, while sleep disorders can increase the prevalence of the disease or aggravate its severity[39]. Once an older adult develops sleep problems, this condition carries deleterious consequences that affect physical and mental health and also social functioning. However,sleep problems in later life are often unrecognized,and are inadequately treated in clinical practice[40]. The public and individuals should pay more attention to sleep problems, which are an important indicator of health status and life quality. Often times,patients go to hospitals in order to treat sleep disorders. No effort has yet been made to prevent the occurrence of sleep disorders. Our study showed SA was also more likely among those without sleep disorders. Appropriate sleep, as an important indicator, had close relationship with SA, which showed the importance of interventions on sleep problems and action should be taken to be controlled as a risk factor as soon as possible.
In our study, the rate of central obesity assessed by WC[41]was 67.60% (1552/2296), and was shown as a risk factor for SA. WC, known as the accumulation of intra-abdominal fat, is a marker for higher metabolic and cardiovascular disease risk,providing a unique indicator of body fat distribution,helping to identify patients who are at increased risk for obesity-related cardiometabolic disease, above and beyond the measurement of BMI; providing additional information for evaluating the risk factors and monitoring a patient's response to diet and exercise treatment[42]. Very few of the general population measure their waist or know their WC condition. A previous study reported that more than half (59%) of at-risk patients had not been informed by their doctors about the link between abdominal obesity and heart disease[43]. Little attention was paid to the meaning of the old person's WC, not to mention the measures of prevention and control WC and take action to promote SA by decreasing the WC of the old. It is important to spread knowledge about WC in order to increase awareness of the importance of WC.
Older adults, as a vulnerable group, is still on the top of the government's agenda. However, solving the challenges facing the elderly is much more complicated than what we had previously realized. The government has enhanced the health care system to treat diseases suffered by the elderly through establishing new institutions and recruiting doctors and nurses. However, there is little emphasis on calling on individuals to take action. Lifestyle,referring to the habits or behavior of an individual or group in daily life, including eating, resting, exercise habits, and hobbies, can be the dominant factors of SA[4,44], and are often significantly associated with health outcomes[45]. Healthy lifestyles can assist aging well[46]. Our study showed positive relationship between healthy lifestyle and SA-the more the better. Intensive lifestyle intervention, for overweight/obese patients with type 2 diabetes mellitus may reduce the risks of developing clinically significant symptoms of depression and preserve physical health-related quality of life[47]. If a person can make healthy lifestyles change, it would reduce the risk of disease and disability, improve the quality of life and have more chance to achieve SA in later life. The finding is consistent with study conducted by the US Centers for Disease Control and Prevention (USCDC), which showed that the four healthy lifestyle behaviors: the death rate among the persons never smoking, keeping healthy diet, doing adequate exercise and having a small amount of alcohol would decrease 63% of the mortality risk and the hazard ratio was 0.37 (95% CI: 0.28-0.49). Healthy lifestyle also played a key role in the prevention and control of central obesity[48]and should be promoted as an effective strategy for the prevention and control of chronic diseases and the promotion of SA[44]. In particular, healthy lifestyle promotion could focus on changes earlier in the life of an elderly individual. The old people should notonly use the existing health care services to maintain their health, but also try their best to maintain a balanced diet, participate in sufficient physical activity, adequate sleep and get rid of the bad habits,so as to increase the positive factors in SA.
This study has some strengthens. As far as we know, this is the first study to explore the prevalence of SA and its independent influential factors in longevity area in China. Our large sample of oldest-old (n=1561) sheds light on the determinants of SA among octogenarians, nonagenarians and centenarians, an understudied group. This study also has some limitations. As a survey conducted in the longevity areas, the information collected were limited, and the extrapolation of the study still have to be verified; lifestyle, sleep quality and the duration of sleep were self-reported, there may be some information bias.
The aging of the Chinese population will continue for the next several decades. A lot of people had made sufficient preparation for the old,and had not known clearly what was the ideal state about himself. So SA should be the basic strategy on aging from the opinion of the individual. In this study,a positive response from the individual perspective was put forward to promote SA: decreasing anemia,improving sleep quality, increasing the number of healthy behaviors, and keeping a healthy lifestyle as long as possible.
Accepted: May 3, 2016
REFERENCES
1. Havighurst RJ. Successful aging. New York: Atherton Press,1963; 299-320.
2. Stephen D, Adam J, Tetso A, et al. Successful aging: Advancing the science of physical independence in older adults. Ageing Res Rev, 2015; 12, 304-27.
3. Cosco T, Prina A, Perales J, et al. Operational definitions of successful aging: a systematic review. Int Psychogeriatr, 2014;3, 373-81.
4. Young Y, Frick KD, Phelan EA. Can successful aging and chronic illness coexist in the same individual? A multidimensional concept of successful aging. J Am Med Dir Assoc, 2009; 2,87-92.
5. Lily N, Tytti S, Antti H. There Successful Aging for Nonagenarians? The Vitality 90+Study. J Aging Res, 2012; 10,868797.
6. Sabia S, Singh A, Cambois E, et al. Influence of individual and combined healthy behaviors on successful aging. CMAJ, 2012;184, 1985-92.
7. Shi XM, Yin ZX, Qian HZ, et al.A study on chronic disease and other related health indicators of centenarians in longevity areas in China. Chinese Journal of Preventive Medicine, 2010; 2,101-7. (In Chinese)
8. Zhai Y, Shi XM, Qian HZ, et al. Association of anemia with cognition among senior female in China. Chinese Journal of Preventive Medicine, 2010; 2, 115-8. (In Chinese)
9. Ly YB, Yin ZX, Luo JS, et al. Association between anemia and 3-year-all-cause mortality among old people in longevity areas in China. Chinese Journal of Epidemiology, 2015; 7, 682-6. (In Chinese)
10. Claudine B, Frédéric B, Hubert B, et al. How to define old age:successful aging and/or longevity. Med Sci, 2012; 3, 281-7.
11.Gu DD. General data quality assessment of the CLHLS healthy longevity in China. Demographic Methods and Population Analysis Healthy Longevity in China, 2008; 1, 39-60.
12.Zeng Y. Towards deeper research and better policy for healthy aging-using the unique data of Chinese Longitudinal Healthy Longevity Survey. China Economic J, 2012; 5, 131-49. (In Chinese)
13.Tombaugh TN, McIntyre NJ. The Mini-Mental State Examination: acomprehensive review. Am Geriatrics Society,1992; 40, 922-35.
14.Feng XQ, Federico G, Lan SM. People with multiple unhealthy lifestyles are less likely to consult primary health care. BMC Fam Prat, 2014; 15, 126, 1-7.
15.Li Y, Zhai FY.The progress of physical activity function research in the elderly. Foreign medical Science (Section Hygiene), 2004;31, 115-20.
16.Bopp M, Braun J, Gutzwiller F. Health risk or resource? Gradual and independent association between self-Rated health and mortality persists over 30 years. PLoS One, 2014; 1, e30795.
17.Jason S, Valerio B. The increasing predictive validity of self-rated health. PLoS One, 2014; 2, e84933.
18.Rowe JW, Kahn RL. Human aging: usual and successful. Science,1987; 4811, 143-9.
19.John W Rowe, Robert LK. Successful Aging. The Gerontologist,1997; 4, 433-40,
20.Li CB, Zhang MY, Zhang XK. A preliminary study of successful aging: criteria and related factors. Chinese Journal of Gerontology, 2000; 2, 67-9. (In Chinese)
21.Anton SD, Woods AT, Ashizawa T, et al. Successful aging:Advancing the science of physical independence in older adults. Ageing Res Revi, 2015; 12, 304-27.
22.Saczynski J, Beiser A, Seshadri S, et al. Depressive symptoms and risk of dementia: the Framingham Heart Study. Neurology,2010; 1, 35-41.
23.Barnes D, Yaffe K, Byers A, et al. Midlife vs late-life depressive symptoms and risk of dementia: differential effects for Alzheimer disease and vascular dementia. Arch Gen Psychiatry,2012; 69, 493-8.
24.Health management technical protocol of aged in China. WS-T,484-2015. 2015; 11-4.
25.Parslow RA, Lewis VJ, Nay R. Successful aging: development and testing of a multidimensional model data from a large sample of older Australians. J Am Ger Soc, 2011; 11, 2077-83.
26.Li CI, Lin CH, Lin WY, et al. Successful aging defined by health-related quality of life and its determinants in community-dwelling elders. BMC Public Health, 2014; 12,1013.
27.Feng, Qiush. Prevalence and correlates of successful ageing: a comparative study between China and South Korea. European Journal of Ageing, 2014; 12, 83-94.
28.Meng XF, D'arcy C. Successful aging in Canada: prevalence and predictors from a population-based sample of older adults false. Gerontology, 2014; 1, 65-72.
29.Strawbridge W, Cohen R, Shema S, et al. Successful aging:Predictors and associated activities. Am J Epidemiol, 1996; 2,135.
30.Zhang XL, Luo H, Zhang X. A comparison study of influencingfactors of two different successful aging models.Zhejiang Journal of Preventive, 2014; 7, 768-71. (In Chinese)
31.Tengku H, Yadollah M, Rahimah I. Predictors and Prevalence of Successful Aging among Older Malaysians. Gerontology, 2012;6, 366-70.
32.Jang SN, Choi YJ, Kim DH. Association of socioeconomic status with successful aging: differences in the components of successful aging. J Biosoc Sci, 2009; 41, 207-19.
33.Xu Jing. Gender difference of the elderly health in China and its decomposition. Journal of Northwest Normal University (Social Sciences), 2015; 52, 139-44.
34.Luo JF, Zhu GX, Zhao QH, et al. Prevalence and risk factors of poor sleep quality among Chinese elderly in an urban community: results from the Shanghai aging study. PLoS One,2013; 11, 0081261.
35.Crowley K. Sleep and sleep disorders in older adults. Neuropsychology Review, 2011; 1, 41-53.
36.Liu CG, Chen XC, Li JM, et al. Investigation on the quality and habit of sleep among elder people in city and country. Journal of Nursing Administration, 2007; 795, 15-9.
37.Sariarslan H, Gulhan Y, Unalan D, et al. The relationship of sleep problems to life quality and depression. Neurosciences (Riyadh), 2015; 7, 236-42.
38.Gildner T, Liebert MA, KowalP, et al. Sleep duration, sleep quality, and obesity risk among older adults from six middleincome countries: findings from the study on global ageing and adult health (SAGE). Am J Hum Biol, 2014; 12, 803-12.
39.Li CI, Lin CH, Lin WY, et al. Successful aging defined by health-related quality of life and its determinants in community-dwelling elders. BMC Public Health, 2014; 12,1013.
40.Rodriguez J, Dzierzewski J, Alessi C. Normal sleep pattern in older adults is associated with a better quality of life perception. Med Clin North Am, 2015; 3, 431-9.
41.Yumuk V, Tsigos C, Fried M, et al. European Guidelines for Obesity Management in Adults. Obes Facts, 2015; 8,402-24.
42.Samuel K, David BA, Steven B. Waist circumference and cardiometabolic risk: A consensus statement from shaping America's health: association for weight management and obesity prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Obesity, 2007; 5, 1661-6.
43.Smith SC Jr, DHaslam. Abdominal obesity, waist circumference and cardiometabolic risk: awareness among primary care physicians, the general population and patients at risk-the shape of the nations survey. Curr Med Res Opin, 2007; 1,29-47.
44.Nina CF, Charlotte AT. Lifestyle and Successful Aging: An Overview. American Journal of Lifestyle Medicine, 2009; 1,6-11.
45.Woo J, Ho S, Yu A, et al. Lifestyle factors and health outcomes in elderly Hong Kong Chinese Aged 70 Years and Over. Gerontology, 2002; 48, 234-40.
46.Kendig H, Browning C, Thomas S, et al. Health, lifestyle, and gender influences on aging well: an Australian longitudinal analysis to guide health promotion. Frontiers in Public Health,Public Health Education and Promotion, 2014; 6, 1-9.
47.Rubin R, Wadden T, Bahnson J, et al. Impact of intensivelifestyleintervention on depression and health-related quality of life in type 2 diabetes: the look ahead trial. Diabetes Care, 2014; 6, 1544-53.
48.Li JX, Li Y, Chen JC, et al. The effects of lifestyle factors on the incidence of central obesity in Chinese adults aged 35-74 years. Chinese Journal of Preventive Medicine, 2014; 7, 581-7. (In Chinese)
Biomed Environ Sci, 2016; 29(5): 347-355 10.3967/bes2016.045 ISSN: 0895-3988
*This work was supported by National Natural Science Foundation of China [81273160, 71233001, 71110107025]; and United Nations Population Fund and the United States National Institutes of Health [R01AG23627].
#Correspondence should be addressed to SHI Xiao Ming, Professor, PhD, Tel 86-10-67791262, E-mail:shixm@chinacdc.cn
Biographical note of the first author: SHI Wen Hui, female, born in 1971, MD, MSc, Associate Professor, majoring in chronic disease control and prevention.
February 24, 2016;
 Biomedical and Environmental Sciences2016年5期
Biomedical and Environmental Sciences2016年5期
- Biomedical and Environmental Sciences的其它文章
- Development of a Novel PmpD-N ELISA for Chlamydia psittaci Infection*
- Evaluation of Six Recombinant Proteins for Serological Diagnosis of Lyme Borreliosis in China*
- Viral Etiology Relationship between Human Papillomavirus and Human Breast Cancer and Target of Gene Therapy
- Whole Genome Sequencing and Comparisons of Different Chinese Rabies Virus Lineages Including the First Complete Genome of an Arctic-like Strain in China*
- Cognitive Training in Older Adults with Mild Cognitive Impairment
- Dietary Exposure to Benzyl Butyl Phthalate in China*