
Cognitive Training in Older Adults with Mild Cognitive Impairment
2016-08-15 03:24LIUXinYanLILiXIAOJiaQingHEChangZhiLYUXiuLinGAOLeiYANGXiaoWeiCUIXinGangandFANLiHuaCollegeofPublicHealthHarbinMedicalUniversityHarbin0086HeilongjiangChinaHeilongjiangProvincialCenterforDiseaseControlandPrevention
LIU Xin Yan, LI Li, XIAO Jia Qing, HE Chang Zhi, LYU Xiu Lin,GAO Lei, YANG Xiao Wei, CUI Xin Gang, and FAN Li Hua,#. College of Public Health, Harbin Medical University, Harbin 0086, Heilongjiang, China; 2. Heilongjiang Provincial Center for Disease Control and Prevention, Harbin 000, Heilongjiang, China; . College of Management for the postgraduate, Harbin Medical University, Harbin 0086, Heilongjiang, China; . Heilongjiang Provincial Hospital, Harbin 000, Heilongjiang, China; . Department of Public Health,Mudanjiang Medical College, Mudanjiang 7000, Heilongjiang, China
Original Article
Cognitive Training in Older Adults with Mild Cognitive Impairment
LIU Xin Yan1,^, LI Li1,^, XIAO Jia Qing2,^, HE Chang Zhi3, LYU Xiu Lin4,GAO Lei1, YANG Xiao Wei5, CUI Xin Gang5, and FAN Li Hua1,#
1. College of Public Health, Harbin Medical University, Harbin 150086, Heilongjiang, China; 2. Heilongjiang Provincial Center for Disease Control and Prevention, Harbin 150040, Heilongjiang, China; 3. College of Management for the postgraduate, Harbin Medical University, Harbin 150086, Heilongjiang, China; 4. Heilongjiang Provincial Hospital, Harbin 150040, Heilongjiang, China; 5. Department of Public Health,Mudanjiang Medical College, Mudanjiang 157000, Heilongjiang, China
Abstract
Objective We investigated the feasibility and efficacy of cognitive training for older adults in rural settings and with low education levels, who have mild cognitive impairment (MCI).
Methods Forty-five older adults (ages >65 years) with MCI were assigned to treatment or control groups, at a 2:1 ratio. Cognitive training occurred in the treatment group for 2 months. The cognitive abilities of the participants were assessed at pre-training, metaphase, and post-training time points, using the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Loewenstein Occupational Therapy Cognitive Assessment (LOTCA), and Hamilton Depression Scale (HAM-D).
Results Following training, cognitive abilities improved in the treatment group, based on the total scores of all 4 measures, as well as specifically on the MoCA and LOTCA. There were differences in the main effects of group and time point on some subscales, but these differences had little, if any, effect on the overall analyses.
Conclusion The present study demonstrated that cognitive training has beneficial effects on attention, language, orientation, visual perception, organization of visual movement, and logical questioning in patients with MCI. Furthermore, the observed effects are long-term changes.
Older adults; Rural; Mild cognitive impairment; Cognitive training; Efficacy
www.besjournal.com (full text) CN: 11-2816/Q Copyright ©2016 by China CDC
INTRODUCTION
Mild cognitive impairment (MCI)describes a transitional stage between normal aging and dementia,and is clinically represented by memory complaints and objective evidence of cognitive impairment, in the absence of evidence of dementia[1-3]. MCI is characterized by confusion, disorientation, restricted attention, and memory impairment, as well as restricted learning and language abilities[4]. Prevalence rates of MCI within older adult populations have been estimated at 3%-42%[5], and the conversion rates between MCI and dementia are estimated at 2%-31%, with a mean annual conversion rate of 10.2%[6]. In addition to age andcertain diseases, social, psychological, and lifestyle factors may contribute to declines in cognitive functioning[7]. Dementia has become a serious health problem for older adults, in addition to conditions associated with normal aging[8-9]. Previous research has demonstrated that training and treatment are beneficial for patients with MCI and dementia[10]. Therefore, effective training and treatment may prevent MCI and dementia.
Ball et al. conducted a cognitive training study with 2832 elderly adults. The study included memory training and cognitive processing, and the results demonstrated that cognitive functioning improved in the treatment group after a period of 2 to 5 years[11]. Cognitive functioning and activities of daily living (ADL) also declined slowly in this study. In addition,Jean performed a systematic review and concluded that cognitive training for older adults improves memory capacity[12].
Research on cognitive functioning began in China in the 1980s[13-15]. This initial research primarily focused on basic cognitive research and factors relevant to MCI. After 2000, researchers found that early training and treatment for MCI reduce the conversion rate from MCI to Alzheimer's disease (AD), and this topic has gained progressively more interest in China[16-17]. Qiao et al. conducted a self-control study and provided training to 30 patients with MCI, including for self-management,maintaining a healthy lifestyle, self-help intelligence (such as intelligence tests or games), self-help physical skills, and communication[18]. After training,cognitive functioning improved significantly in patients with MCI. Zhang et al. conducted cognitive functioning training with older adults in the community, including that for tasks such as recognizing photographs, arithmetic, memory,attention, orientation, ability to calculate, and executive ability[19]. After 6 months, the cognitive abilities of these older adults were enhanced,especially for memory, attention, and orientation. Previous research on MCI in China involved older adults who lived in the city and had high education levels[20-21]. Education levels of older adults residing in rural China are low[22]and previous studies have not investigated whether cognitive training is effective in these populations. In addition, the previous research on cognition did not focus on the effects of training[23]. Thus, we evaluated the effects of cognitive training in older adults with MCI who reside in rural areas, using a variety of standardized scales.
METHODS
Data Source
Data were derived from research funded by the Department of Health (Heilongjiang province; study on mild cognitive impairment of older adults residing in rural Heilongjiang province). The research was conducted at a health center in Si Duan village. We used cluster sampling to select 520 participants from the data set, including 66 older adults who were diagnosed with MCI. Forty-five patients with MCI were available and willing to attend our cognitive training.
Participants and Criteria
We adopted the criteria established by Petersen et al. for clinical diagnosis of MCI: 1) subjective patient, other informant, or a clinician report of cognitive decline over time, 2) objective evidence of cognitive impairment in one or more cognitive domains using formal or bedside testing, 3) the impact of cognitive impairments on daily functioning does not preclude independence, and 4) the patient does not meet criteria for dementia[1].
Training and Assessment Instruments
We established a training research group consisting of trained researchers. Forty-five patients with MCI who met our inclusion criteria were randomly assigned to treatment or control groups at a 2:1 ratio. These patients with MCI were first assigned numbers from 1-45, and 45 random 2 digit numbers were then selected in any 2 rows of a random number table. Based on this process,patients with numbers 1-30 were assigned to the training group and patients with numbers 31-45 were assigned to a no treatment control group. Prior to training, we conducted between group comparisons for demographic information and cognitive abilities [age, years of education, gender,Mini-Mental State Examination (MMSE) scores, and Activities of Daily Lving (ADL)], in order to ensure that there were no preexisting differences between the groups. The control group did not receive any treatment, in order to allow us to evaluate potential non-treatment related changes over time and ensure accurate interpretations of the results. The treatment group consisted of 30 patients with MCI,and was further divided into 8 subgroups (3-5 patients per subgroup). The at-home training occurred for 2 months, with each subgroup receiving 2 h/d of training. There were 5 aspects of training, including training for attention, memory,cognition, language, andtaskperformance. Participants were not assigned homework,and training only occurred for 2 h/d.Training was also flexible with regard to individual changes in cognitive ability.The components of training are described in Table 1.
The cognitive abilities of participants were evaluatedatpre‐training, metaphase, and post‐training time points.Participants completed the MMSE,Montreal CognitiveAssessment Chinese version(MoCA),Loewenstein Occupational Therapy CognitiveAssessment(LOTCA),andHamilton Depression Scale(HAM‐D;17‐item Chinese version). The Chinese version of the MMSE,revised by Yuanming ZHANG et al.,is widely used.The test has goodreliabilityandtheintraclasscorrelation coefficient of the joint inspection is 0.99.Convergent validity between the Wechsler Adult Intelligence Scale and the MMSE is also ideal.Many researchers have conducted cross‐sectional investigations with results indicating that the construct validity and internal consistency of the MoCA are excellent;the Cronbach's alpha coefficient is 0.818 and total scores are correlated with scores on the MMSE.The Chinese version of the MoCA consists of 7 items and has a maximum total score of 30 points,with diagnosis of MCI indicated if the score is 15‐24[24]. Fourteen cooperative groups from the Chinese Psychiatric Union evaluated the 17‐item version of the HAM‐D and found that the reliability coefficient of the total score was 0.88‐0.99.Older adults may be depressed if scores are between 7 and 17[25]. Compared with other authoritative scales,the LOTCA is widely used with patients who have traumatic brain injuries and cerebral vascular disease(both children andadults)[26‐28].Thecorrelationcoefficientof different results is 0.8[29‐30].The maximum score is 119 points and higher scores represent better cognitive function.The cognitive tests used in the present study aresummarized in Table2.

Table 1.Components of Training
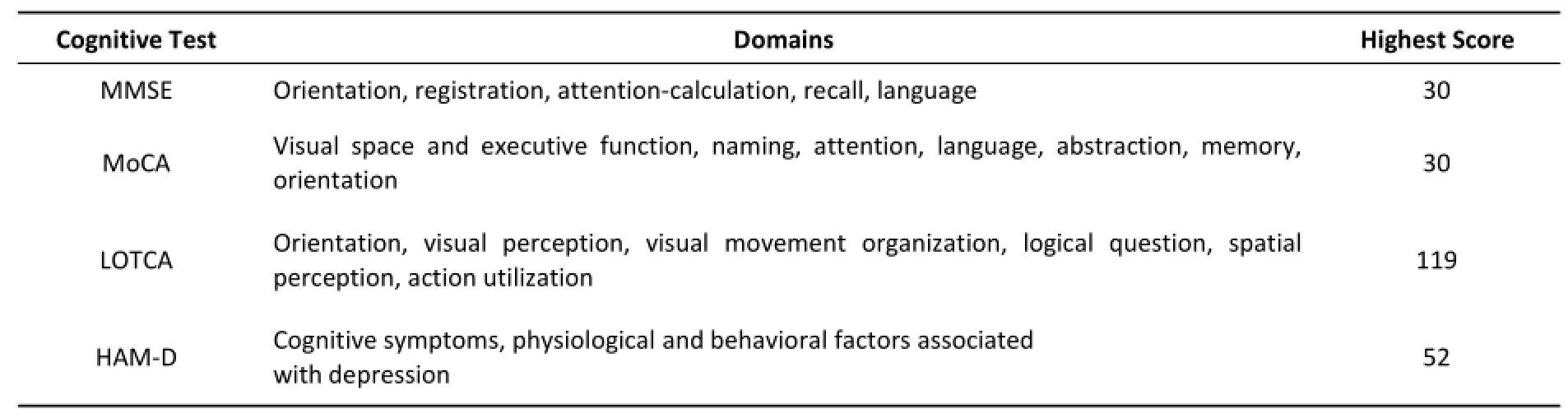
Table 2.Components of Cognitive Tests
Analyses
In order to ensure comparability between the treatment and control groups,we used t‐tests and chi‐square tests for pre‐treatment comparisons and usedconsistentmethodsduringtraining.SPSS (version 16.0,IBM,Armonk,NY,USA)was used to conduct statistical analyses,such as applied analysis of variance forrepeated measures and mean comparisons.Mauchly's test of sphericity is a statistical test used to validate repeated measures analyses of variance(ANOVAs),and is an important assumption of these analyses.Sphericity refers to the condition where the variances of the differences between all possible pairs of groups are equal. Therefore,violation of sphericity occurs when the variancesofthedifferencesbetweenall combinations of the groups are not equal.Mauchly's tests of sphericity were calculated for all cognitive evaluation data(P<0.05).If sphericity was violated,we corrected the degrees of freedom prior to performing ANOVAs,using the Geisser‐Greenhouse (G‐G)method.
RESULTS
Participants
The treatment and control groups were 73.5±6.1 and 70.3±4.3 years of age,respectively.Most older adults were illiterate or had achieved only primary school levels of education.Twenty‐five participants had not completed any formal education and only 9 patients had completed 6 years of education.The number of years of education in the treatment and control groups was 2.1±2.7 and 2.2±2.5,respectively. There were 10 men and 20 women in the treatment group(1:2 ratio),whereas there were 6 men and 9 women in the control group(1:1.5 ratio).In the treatment group,the total pre‐training MMSE score was 16.2±2.9 and the ADL score was 16.5±1.3.In the control group,the total pre‐training MMSE score was 15.0±3.4 and the ADL score was 16.4±1.2.We concludedthattherewerenopre‐training differences between the groups(P>0.05).Patient characteristics are given in Table 3.

Table 3.Patient Characteristics
Analyses of Results
Results of Repeated Measures AnalysisThe results of repeated measures analyses demonstrated that most P values were<0.001,except those for the main effect of time point for the HAM‐D score (P=0.097)and the total time to complete the LOTCA (P=0.011).The results are given in Table 4.
All P values for main effects of group were <0.001,indicating significant differences between treatment and control groups.The P values for the MMSE and LOTCA scores were<0.01 at metaphase and the P value for the MoCA data was<0.05 at metaphase.The P values of scores from all 4 measures were<0.01 at post‐training(Table 5).
Analyses of Repeated Measurements for MoCA Scores
The visual space and executive function(VE)scores increased more in the treatment group compared to the control group from pre‐to post‐training(P<0.05).There were no differences between the groups or for the interaction between groups and time point;however,the naming score increased in the treatment group compared to the control group(P<0.01).Significant differences were observedbetweengroupsandnointeraction occurred between group and time point;there were similar effects for the attention and orientation scores,but the P value indicated greater statistical confidence(P<0.01).Thereweredifferences betweengroupsandinteractionsbetween group and time point;however,the language scoresbetween the two groups were stable from pre‐to post‐training.There was a statistically significant difference between groups(P<0.01)and interactions between group and time point for abstraction and memoryscores.Therewerealsosignificant differences between groups but no interaction between group and time point.These results are given in Table 6.
Analyses of Repeated Measurements for LOTCA Scores
The results verified that the orientation,visual perception(VP),visualmovementorganization (VMO),and logical questioning(LQ)scores increased in the treatment group compared to the control group from pre‐to post‐training(P<0.01).Significant differences were observed between groups and there was an interaction between group and time point;the spatial perception(SP)scores demonstra‐ted particularly large differences between groups. There was also a statistically significant difference between groups,but no interaction between group and time point;the action utilization(AU)score was notdifferentbetweenpre‐andpost‐training. However,there were differences between groups (P<0.01),but no interaction between group and time point.The LOTCA results are presented in Table 7.
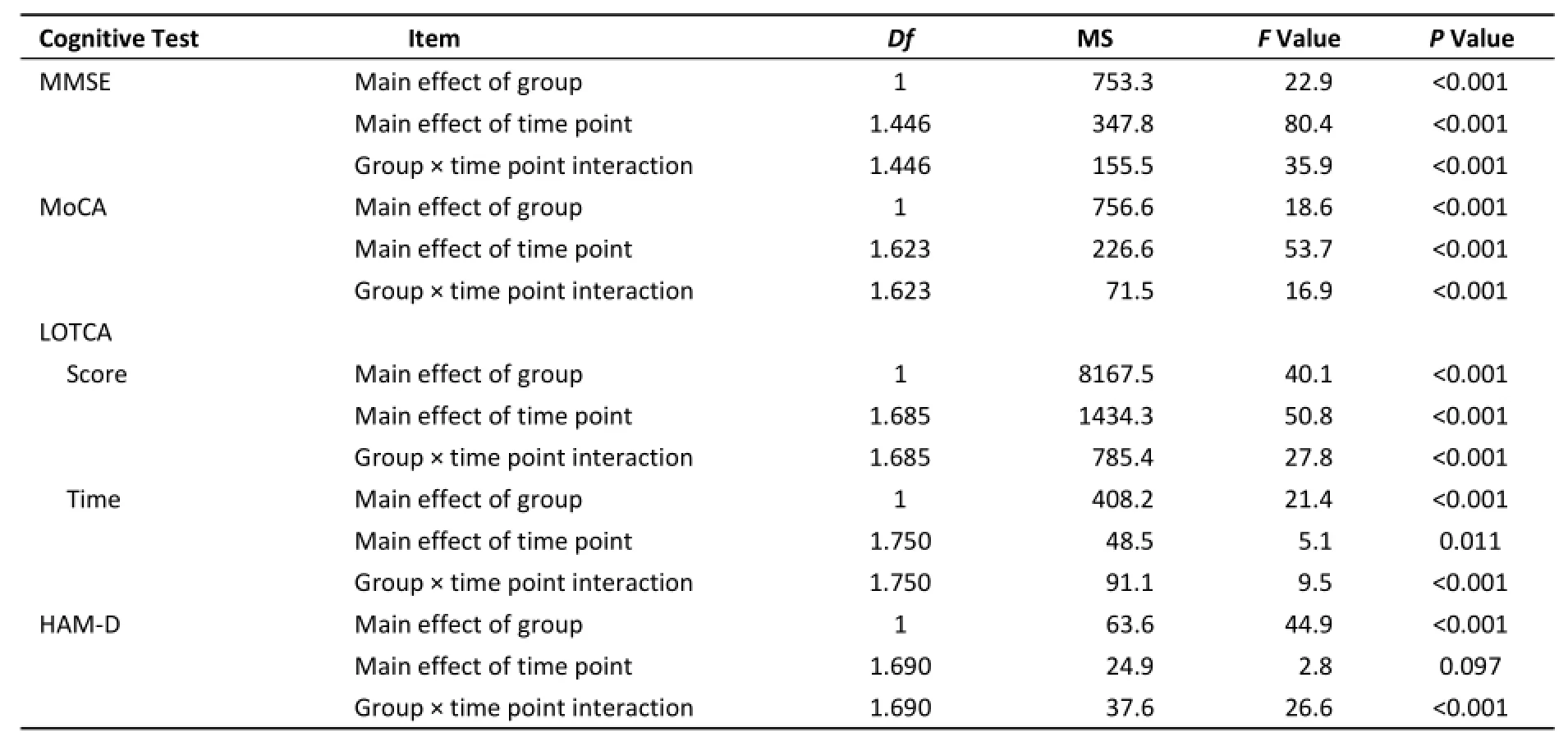
Table 4.Outcomes of Repeated Measures Analyses
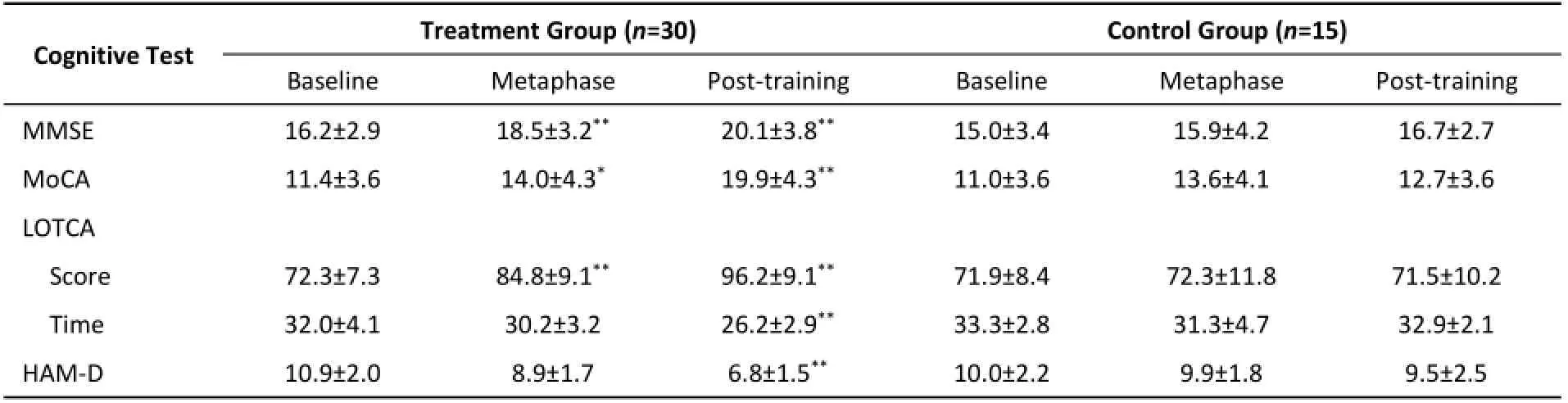
Table 5.Between‐group ComparisonsAcross Time Points
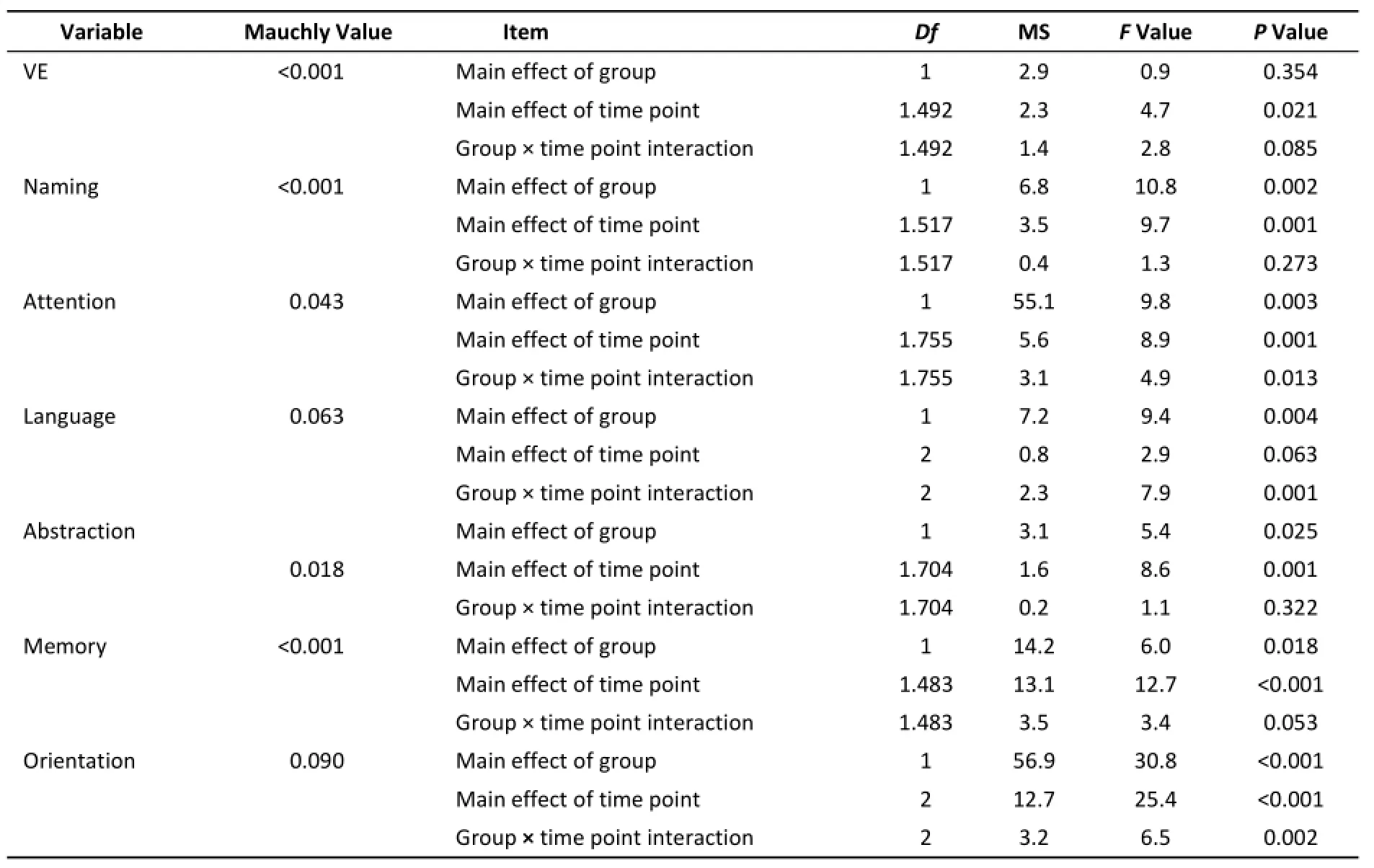
Table 6.Analyses of MoCA Scores

Table 7.Analyses of LOTCA Data
DISCUSSION
Many studies have concluded that age is an important factor affecting cognitive functioning in older adults[20-21]. The participants in the present study were >65 years of age and the mean age was 72.5±5.8 years. Declines in bodily functions,especially in the nervous and perception systems,greatly influence cognitive abilities and ADL. The settings of this study were remote villages in relatively poor areas of China that have been influenced by historical events that have contributed to a lack of educational resources. The results demonstrated that level of education may affect cognitive abilities, with an association between fewer years of education and faster declines in cognitive ability with age, which is consistent with the findings of previous studies[31-32].
The present study utilized 4 authoritative scales to evaluate cognitive decline. Scores on each scale,as well as time to complete the test, demonstrated that main effects of group differed depending on the measure. Except for the HAM-D scale, there were main effects of time point (P<0.05). There was an interaction between group and time point for all scores. We compared scores at different time points and concluded that the MMSE and LOTCA scores were statistically different between groups during training and that these effects were more robust for the MMSE, MoCA, HAM-D, and LOTCA scores and for the completion time point after training. These results demonstrate that training improved the cognitive ability of patients with MCI who reside in rural areas. The treatment group experienced improvements during metaphase and post-training,which were greater than improvements in the control group. Furthermore, this effect of training was more robust with the passage of time. Older adults with MCI, who reside in rural areas, participated in this training. Training may stimulate brain activity and promote cognitive ability by using cognition to complete all tasks independently. Our results are consistent with those of cognitive training studies of older adults in urban communities[33-35].
Main effects of group occurred for all MoCA subtests except VE, which required participants to think about the relationship between 2 items while using logical abilities and spatial imagination. Due to historical events and living conditions, older adults in China have not had the opportunity to receive training that would promote their abilities in these types of tasks. Some cognitive abilities, such as language, attention, and orientation, which are closely related to daily life, improved after training. Regarding the main effect of time, all subtests except language improved in the treatment group compared to the control group. There were interactions between group and time point for language, attention, and orientation. We concluded that the interaction between group and time point indicates that this 2 month training easily enhances these abilities. In contrast, cognitive abilities such as VE, naming, abstraction, and memory, which were difficult to learn, did not improve. Although the mean MoCA score increased,it was still below the standard scores of 15-24 for patients with MCI. This finding likely occurred because these MoCA score values were not standardized in older adults with low levels of education. However, the elevated scores observed in the present study do still represent improvements in cognitive functioning.
The LOTCA scores demonstrated that the main effect of group differed between subscales. Main effects of time point indicated that all subscales except AU differed, although there were varied effects at different time points. There were differences in orientation, VP, VMO, and LQ, as well as interactions between group and time point. Differences between the LOTCA scores at different time points indicate that cognitive training improves cognitive abilities such as VP, orientation, VMO, LQ,SP, and AU in older adults who reside in rural areas,although the magnitude of effects differed. Tasks that are easier to learn, such as VP and orientation,as well as vivid tasks such as VMO and LQ, improved significantly. In contrast, there were no significant effects for tasks such as SP and AU, which the participants had less interest in learning.
Cognitive training is an effective method to promote improvements in the cognitive abilities of patients with MCI[36]. After training, improvements in attention, language, orientation, VP, VMO, and LQ confirmed that this training is suitable for older adults with low education levels who reside in rural areas, and that the training contributes to rehabilitating cognitive function in these patients with MCI. Continued improvements in the scores of the treatment group indicate that the training has continuing benefits over time. During the training,we also observed that older adults were interested in the more entertaining tasks and could experience benefits within a short period of time, but theirprogress was slower in tasks that most participants found less interesting, such as arithmetic.
CONCLUSION
Our cognitive training protocol improved the cognitive abilities of patients with MCI who reside in rural areas and who have low education levels, with particular benefits for attention, language,orientation, VP, VMO, and LQ tasks. The observation of continued improvements in the treatment group over time indicates that cognitive training has long-term efficacy.
Limitations
Although there is previous research on MCI in Chinese populations, this work is limited compared to findings in other ethnic groups, particularly with regard to the effects of cognitive training. In the present study, we did not collect physiological data,such as ERP (event-related potential) recordings. Future research would benefit from the use of such techniques to support associated physical impacts of training. However, the present study provides initial data to contribute to this field in Chinese populations, and will be useful to future researchers. Conflict of Interest Declaration
The authors declare that they have no conflicts of interest.
Description of Author Roles
LXY, LL, XJQ, and FLH, conceived the study and designed it, as well as performing coordination roles. FLH conducted the search for participants, and LXY,XJQ, HCZ, LXL, YXW, and CXG completed data extraction. HCZ and GL conducted the data analyses. LXY, LL, and XJQ drafted the manuscript, and FLH revised and edited the manuscript. All authors read and approved the final manuscript.
ACKNOWLEDGMENTS
This work was supported by the Department of Health, Heilongjiang Province, China. The authors thank the Department of Health, Heilongjiang Province for this support. The authors also thank Chunjie Dai (nurse at the health center in Si Duan village), Yuwen Zou (teacher), and Shulin Wang (director of the health center in Si Duan village) for their contributions to this work.
Accepted: May 3, 2016
REFERENCES
1. Petersen RC, Smith GE, Waring SC, et al. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol, 1999; 56, 303-8.
2. Morris JC, Storandt M, Miller JP, et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch Neurol, 2001; 58, 397-405.
3. Almkvist O, Basun H, Bäckman L, et al. Mild cognitive impairment an early stage of Alzheimer's disease. J Neural Transm Suppl, 1998; 54, 21-9.
4. Feldman H, Scheltens P, Scarpini E, et al. Behavioral symptoms in mild cognitive impairment. Neurology, 2004; 62, ll99-1201.
5. Ward A, Arrighi HM, Michels S, et al. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimer's & Dementia, 2012; 1, 14-21.
6. Bruscoli M, Lovestone S. Is MCI really just early dementia? A systematic review of conversion studies. Int Psychogeriatr,2004; 16, 129-40.
7. Tervo S, Kivipelto M, Hanninen T, et al. Incidence and Risk Factors for Mild Cognitive Impairment: A Population-Based Three-Year Follow-Up Study of Cognitively Healthy Elderly Subjects. Dement Geriatr Cogn Disord, 2004; 17, 196-203.
8. Huckans M, Hutson L, Twamley E, et al. Efficacy of Cognitive Rehabilitation Therapies for Mild Cognitive Impairment (MCI)in Older Adults: Working Toward a Theoretical Model and Evidence-Based Interventions. Neuropsychol Rev, 2013; 23,63-80.
9. Stott J, Spector A. A review of the effectiveness of memory interventions in mild cognitive impairment (MCI). International Psychogeriatrics, 2011; 23, 526-38.
10.GA Boissonneault. MCI and dementia, diagnosis and treatment. JAAPA, 2010; 23, 18-25.
11. Ball K, Daniel B Berch, Helmers Karin F, et al. Effects of cognitive training interventions with older adults: a randomized controlled trial. J the American Medical Association, 2002; 18, 2271-81.
12. Leonie Jean. Cognitive Intervention Programs for Individuals with Mild Cognitive Impairment: Systematic Review of the Literature. Am J Geriatr Psychiatry, 2010; 18, 281-96.
13. Katzman R, Zhang MY, Ouang YQ, et al. A Chinese version of the Mini-Mental State Examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol, 1988; 41, 971-8.
14. Yu ES, Liu WT, Levy P, et al. Cognitive impairment among elderly adults in Shanghai, China. J Gerontol, 1989; 44,97-106.
15. Ding Ding, Hong Zhen. Progression of Epidemiological Studies of Dementia and Mild Cognitive Impairment among Elderly. Chin J Clin Neurosci, 2013; 21, 101-8.
16. Hong Chen, Ying Gu, Chunxia Wang, et al. Community Based Training for Mild Cognitive Impairment. Chinese Primary Health Care, 2008; 22, 17-9. (In Chinese)
17. XX Yang, J Wang, JY Luo, et al. Assessment and rehabilitation strategies of mild cognitive impairment. Chinese Journal of Rehabilitation Medicine, 2008; 23, 849-53. (In Chinese)
18. YC Qiao. Study on nursing training for improvement of cognitive function in patients with mild cognitive impairment. Chinese Journal of practical nursing, 2011; 27, 1-4. (In Chinese)
19. Q Zhang, H Zeng, SL Song, et al. Impact of cognitive training on cognitive function in aged community residents. Journal of Nursing Science, 2010; 25, 16-8. (In Chinese)
20. WH Zhang, GF Zhao, XC Liu, et al. Cognitive Function and Related Factors of Urban Elderly: a cross-sectional study. Chinese Mental Health Journal, 2001; 15, 327-30. (In Chinese)
21. ZW Li, YQ Huang, YZ Liu, et al. Influential factors about decline of cognitive ability in the elderly. Chinese General Practice,2008; 11, 174-6. (In Chinese)
22. Jinjie Du, Zhilin Suo. Studies on rural education and rural human resource development in Hei long jiang. Rural economy,2009; 11, 31-2. (In Chinese).
23. Luis CA, Loewenstein DA, Acevedo A, et al. Mild cognitive impairment: directions for future research. Neurology, 2003;61, 438-44.
24. Nasreddine ZS, Phillips NA, Bedirian V, et al. Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of The American Geriatrics Society, 2005; 53, 695-9.
25. Bech P. Rating scale for affective disorders: their validity and consistency. Acta Psychiatrica Scandinavica, 1981; 64, 18.
26. Cermak S, Katz N, McGuire E, et al. Performance of Americans and Israelis with vascular accident on the Loewenstein Occupational Therapy Cognitive Assessment (LOTCA). Am J Occup Ther, 1995; 49, 500-6.
27. Annes G, Katz N, Cermak S, et al. Comparison of younger and older healthy adults on the Loewenstein Occupational Therapy Cognitive Assessment. Occupational Therapy International,1996; 3, 157-73.
28. Katz N, Champagne D, Cermak S, et al. Comparison of the performance of younger and older adults on three versions of a puzzle reproduction task. Am J Occup Ther, 1997; 51, 562-8.
29. Katz N, Itzkovich M, Averbuch S, et al. Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) battery for brain-injured patients: reliability and validity. Am J Occup Ther, 1989; 43, 184-92.
30. Katz N, Elazar B, Itzkovich M, et al. Construct validity of a geriatric version of the Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) Battery. Physical & Occupational Therapy in Geriatrics, 1995; 13, 31-46.
31. Shuqiao Yao, Hui Zeng, Shuiying Sun, et al. Investigation on status and influential factors of cognitive function of the community-dwelling elderly in Changsha City. Arch Gerontol Geriatr, 2009; 49, 329-34.
32. Mendez MF, Cunnings JL. Dementia: A clinical approach.3rded. Butterworth/Heineman, Philadelphia PA. 2008.
33. Vidovich MR, Lautenschlager NT, Flicker L, et al. The PACE study: a randomized clinical trial of cognitive activity (CA) for older adults with mild cognitive impairment (MCI). Trials, 2009;10, 11-4.
34. Edwards JD, Wadley VG, Vanee DE, et al. The impact of speed of processing training on cognitive and everyday performance. Aging & Mental Health, 2005; 3, 262-71.
35. Draganski B, Gaser C, Buseh V, et al. Change in grey matter induced by training. Nature, 2004; 427, 311-2.
36. Kurz A, Pohl C, Ramsenthaler M, et al. Cognitive rehabilitation in patients with mild cognitive impairment. Int J Geriatr Psychiatry, 2009; 24, 163-8.
Biomed Environ Sci, 2016; 29(5): 356-364 10.3967/bes2016.046 ISSN: 0895-3988
^These authors contributed equally to the manuscript.
#Correspondence should be addressed to FAN Li Hua, Tel: 86-451-87502857, E-mail: lihuafan2012@163.com
Biographical notes of the first authors: LIU Xin Yan, male, born in 1981, Master of Management, majoring in community health service and health management; LI Li, female, born in 1978, PhD, majoring in community health management; XIAO Jia Qing, female, born in 1982, MM, majoring in disinfection.
January 7, 2016;
 Biomedical and Environmental Sciences2016年5期
Biomedical and Environmental Sciences2016年5期
- Biomedical and Environmental Sciences的其它文章
- Development of a Novel PmpD-N ELISA for Chlamydia psittaci Infection*
- Evaluation of Six Recombinant Proteins for Serological Diagnosis of Lyme Borreliosis in China*
- Viral Etiology Relationship between Human Papillomavirus and Human Breast Cancer and Target of Gene Therapy
- Whole Genome Sequencing and Comparisons of Different Chinese Rabies Virus Lineages Including the First Complete Genome of an Arctic-like Strain in China*
- The Status and Associated Factors of Successful Aging among Older Adults Residing in Longevity Areas in China*
- Dietary Exposure to Benzyl Butyl Phthalate in China*